1 College of Osteopathic Medicine, Kansas City University, Kansas City, Missouri
2 Phoenix Children’s Hospital, Phoenix, Arizona
3 Children’s Mercy Hospital, Kansas City, Missouri
4 Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pediatric achalasia is rare, with an average age at diagnosis of 7 years. Because symptoms overlap with gastroesophageal reflux disease (GERD), diagnosis is often delayed. Patients present with dysphagia with solids and liquids, regurgitation, and a history of failed treatment of GERD. On imaging, the proximal esophagus is dilated with smooth, tapered narrowing distally, forming the classic “bird’s beak” sign. A definitive diagnosis is made with the absence or markedly diminished contractility seen on HRM. Short-term management is performed endoscopically, whereas definitive treatment is surgical.
Keywords
dysphagia, motility disorder
Categories
Case Summary
A mid-childhood male presented with a 3-month history of vomiting and referred to pediatric gastroenterology for evaluation. He reported vomiting and intermittent chest pain several times daily with both liquids and solids and had lost 5 pounds over the past 6 months. The patient subsequently underwent a fluoroscopic evaluation of his upper gastrointestinal tract.
Imaging Findings
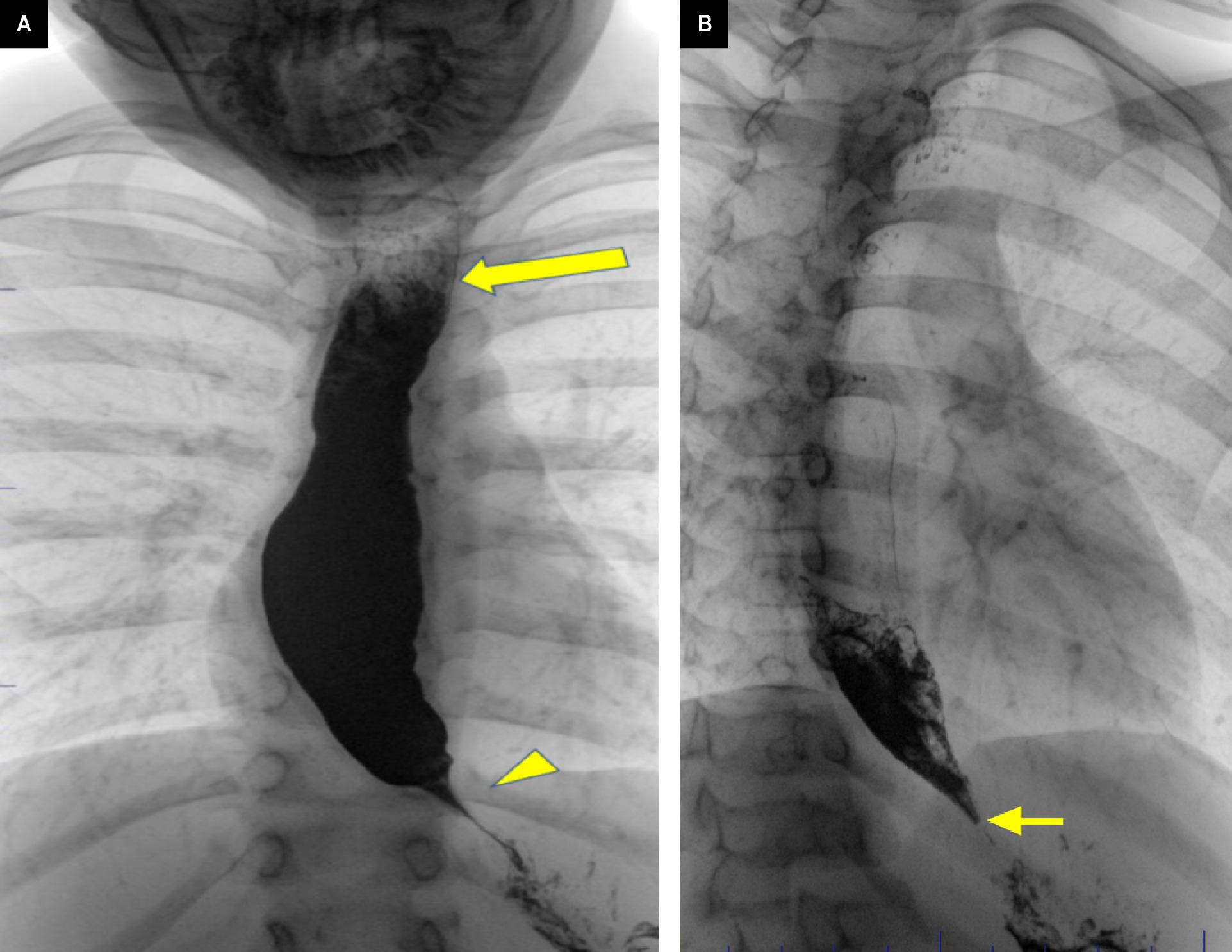
Upper gastrointestinal evaluation (Figure 1) demonstrated a dilated esophagus with abrupt tapered narrowing at the gastroesophageal junction. Delayed esophageal emptying was observed with diminished peristalsis and a persistent fluid/barium level.
Diagnosis
Achalasia.
The differential diagnosis of an esophageal motility disorder in the pediatric population includes achalasia, gastroesophageal reflux disease (GERD), distal esophageal spasm, hypercontractile esophagus, and malignancy-induced pseudoachalasia.
Discussion
Achalasia is an esophageal motility disorder characterized by disinhibited contraction of the lower esophageal sphincter (LES). 1 It occurs with an incidence of 162 per 100,000 adults in the United States. However, it is rarely seen in children. 2 While achalasia is caused by neuronal loss of the myenteric plexus, the etiology of neuronal loss in primary achalasia is unknown. 1 Currently, an autoimmune etiology is thought to have the strongest evidence due to the presence of anti-myenteric plexus auto-antibodies. 3 Other possible causes are viral infections (herpes simplex, measles), Chagas disease, Down syndrome, adrenal glucocorticoid deficiency, and neurodegenerative factors.
Pediatric achalasia can be seen with a rare autosomal-recessive disorder called Allgrove syndrome or triple A syndrome. Since the identification of the syndrome in 1978, there have been about 100 cases reported. This genetic disorder results from mutations of the AAAS gene located on chromosome 12q13 4 and is seen with the classic triad of adrenal insufficiency (Addison disease), alacrimia, and achalasia. However, in situations in which a pediatric patient presents with achalasia and alacrimia but absent adrenal insufficiency, clinicians should be alerted to GMPPA-CDG. 4 This metabolic disorder is characterized by defects in glycosylation, which is essential in the formation of glycoproteins and glycolipids. Since both glycoproteins and glycolipids are essential for molecular communication within the body, a deficiency in glycosylation can cause a variety of mild to life-threatening symptoms seen across multiple organ systems and typically presents in the neonatal period. 3,4
Secondary achalasia is caused by the parasite Trypanosoma cruzi that causes Chagas disease found in Central and South America. 4 Worldwide, there are about 6-7 million people infected with the parasite that leads to about 1200 deaths per year. The disease presents in 2 phases. The acute phase begins when the parasite circulates in the blood, lasts for 1-2 months, and may be asymptomatic or with nonspecific symptoms like fever, headache, adenopathy, muscle, abdominal, or chest pain. The chronic phase occurs when the parasite remains in the body. Patients may be asymptomatic. 20-30% become symptomatic with cardiac (cardiomyopathy, heart failure, arrhythmias, and sudden cardiac arrest) or gastrointestinal manifestations (megaesophagus, megacolon). Late morbidity and mortality come from cardiac arrhythmias or heart failure. Effective treatment with benznidazole or nifurtimox is curative in the early phase of the disease. 5
Patients with achalasia most commonly present with dysphagia of solids and liquids. This symptom is present in 90% of patients. Other common symptoms include regurgitation (75% of patients), weight loss (60% of patients), chest or retrosternal pain (50% of patients), and acid reflux that is not responsive to proton pump inhibitor therapy (40% of patients). 1 In many situations, achalasia is mistaken for GERD, leading to months of discomfort before a definitive diagnosis is made. Clinically, children with achalasia will regurgitate food, while those with GERD bring up partially digested food from the stomach. This insidious presentation underscores the challenges of making the correct diagnosis. In children, the average age of achalasia at diagnosis is 7 years, with a range of 1-14 years. The usual work-up of achalasia often involves upper endoscopy, esophageal manometry, and an upper gastrointestinal series. Upper endoscopy is useful for direct visualization of esophageal dilation, finding food in the esophagus, and ruling out masses but is not considered a diagnostic tool.
Imaging is critical to diagnose achalasia. Chest x-ray shows a widened mediastinum with a dilated air-fluid level in the esophagus. Esophagram will show esophageal dilation with smooth, conical, distal tapering of the distal esophagus, giving a “bird’s beak” appearance. The gold standard for the diagnosis of achalasia is high- resolution manometry (HRM). HRM replaces conventional esophageal manometry, with the biggest difference between the 2 being a more accurate functional mapping of esophageal peristalsis. 5 An HRM that is positive for achalasia will show impaired peristalsis of the lower two-thirds of the esophagus, a high LES resting pressure, absent LES relaxation, and no signs of obstruction.
In general, pediatric achalasia management mirrors adult treatment. It is divided into endoscopic and surgical intervention. Endoscopic intervention is useful, but its effects are short-lived. Thus, multiple procedures are required over time. Surgical intervention is considered to be the definitive treatment. 4,6 First-line endoscopic intervention includes balloon dilation of the narrowed esophageal segment while second-line endoscopic intervention includes botulinum toxin injection. Generally, these options are beneficial for patients who have high-risk factors for surgery. Since the pediatric population is typically healthier than their adult counterparts, children are usually treated surgically.
Surgical intervention includes 2 highly effective myotomies called laparoscopic Heller myotomy (LHM) and peroral endoscopic myotomy (POEM). Both modalities benefit from intraoperative real-time feedback, with LHM utilizing HRM and POEM utilizing an endoscopic functional lumen imaging probe. While both types of myotomy are effective, POEM has a potential advantage due to its minimally invasive surgical approach through the mouth. A meta-analysis performed by Facciorusso et al 7 found POEM and LHM to have a similar efficacy. However, POEM had a lower rate of major adverse events, albeit with an increased rate of GERD. 7-9
Conclusion
Pediatric achalasia is rare, with an average age at diagnosis of 7 years. Because symptoms overlap with GERD, diagnosis is often delayed. Patients present with dysphagia with solids and liquids, regurgitation, and history of failed treatment of GERD. On imaging, the proximal esophagus is dilated with smooth, tapered narrowing distally forming the classic “bird’s beak” sign. A definitive diagnosis is made with absence or markedly diminished contractility seen on HRM. Short-term management is performed endoscopically, whereas definitive treatment is surgical.
References
- Khashab M, Vela M, Thosani N. ASGE guideline on the management of achalasia. Gastrointestinal Endoscopy. 2020;91(2):213-227. doi:10.1016/j.gie.2019.04.231.
- Gaber C, Eluri S, Cotton C. Epidemiologic and economic burden of achalasia in the United States. Clin Gastroenterol Hepatol. 2022;20(2):342-352. doi:10.1016/j.cgh.2021.02.035.
- Furuzawa-Carballeda J, Torres-Landa S, Valdovinos M. New insights into the pathophysiology of achalasia and implications for future treatment. World J Gastroenterol. 2016;22(35):7892-7907. doi:10.3748/wjg.v22.i35.7892.
- Geiculescu I, Dranove J, Cosper G. A rare cause of infantile achalasia: GMPPA-congenital disorder of glycosylation with two novel compound heterozygous variants. Am J Med Genet A. 2022;188(8):2438-2442. doi:10.1002/ajmg.a.62859.
- El Gharib A, Dantas R. Cross-sectional study of swallowing phases in cases of megaesophagus caused by chagas disease. Gastroenterology Res. 2021;14(5):290-295. doi:10.14740/gr1458.
- Pop D, Pop R, Blaga T. New diagnostic and therapeutic procedures applied in pediatric esophageal achalasia in a pediatric tertiary center: a case series. Exp Ther Med. 2023;25(3). doi:10.3892/etm.2023.11800.
- Tashiro J, Petrosyan M, Kane T. Current management of pediatric achalasia. Transl Gastroenterol Hepatol. 2021;6:33. doi:10.21037/tgh-20-215.
- Facciorusso A, Singh S, Abbas Fehmi S. Comparative efficacy of first-line therapeutic interventions for achalasia: a systematic review and network meta-analysis. Surg Endosc. 2021;35(8):4305-4314. doi:10.1007/s00464-020-07920-x.
- Costantini M, Salvador R, Costantini A. Esophageal achalasia: pros and cons of the treatment options. World J Surg. 2022;46(7):1554-1560. doi:10.1007/s00268-022-06495-z.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Achalasia. Applied Radiology. 2025. doi:10.37549/JPCR-25-0019.