Acroosteolysis: Primary Hypertrophic Osteoarthropathy
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -2
Published: November 1, 2025
1 University of Missouri–Kansas City School of Medicine, Kansas City, Missouri
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, University of Cincinnati College of Medicine, Cincinnati, Ohio
4 Department of Radiology, Cincinnati Children’s Hospital, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Categories
Case Summary
A school-aged child who has had accelerated growth of the fingers since infancy and a history of excessive sweating was found to have a genetic mutation of the 15-hydroxyprostaglandin dehydrogenase gene located on chromosome 4q34-35 and was subsequently diagnosed with primary hypertrophic osteoarthropathy (PHO). The child has never complained of arthralgias, myalgias, limping, or rashes. Physical exam showed clubbing of the fingers, deformities of the finger joints and lower extremities, edema, leg length discrepancy, excessive sweating of the hands and feet, hypermobile upper extremities, and a rash over the plantar surface of the foot.
Imaging Findings
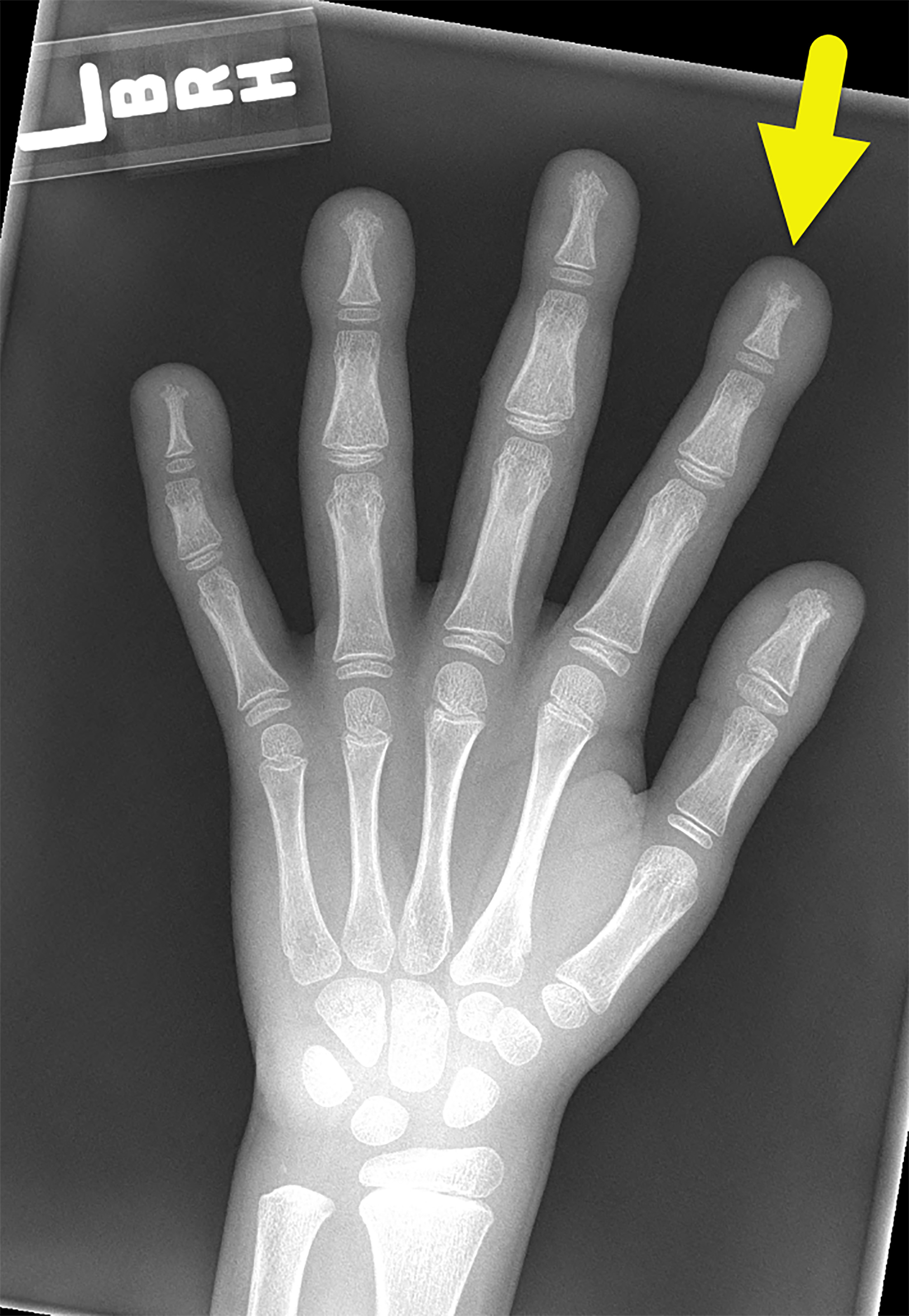
Left-hand radiograph (Figure 1) shows symmetric prominence of the soft tissues surrounding the distal phalanges, as well as early signs of acroosteolysis, most notable at the tuft of the left second finger.
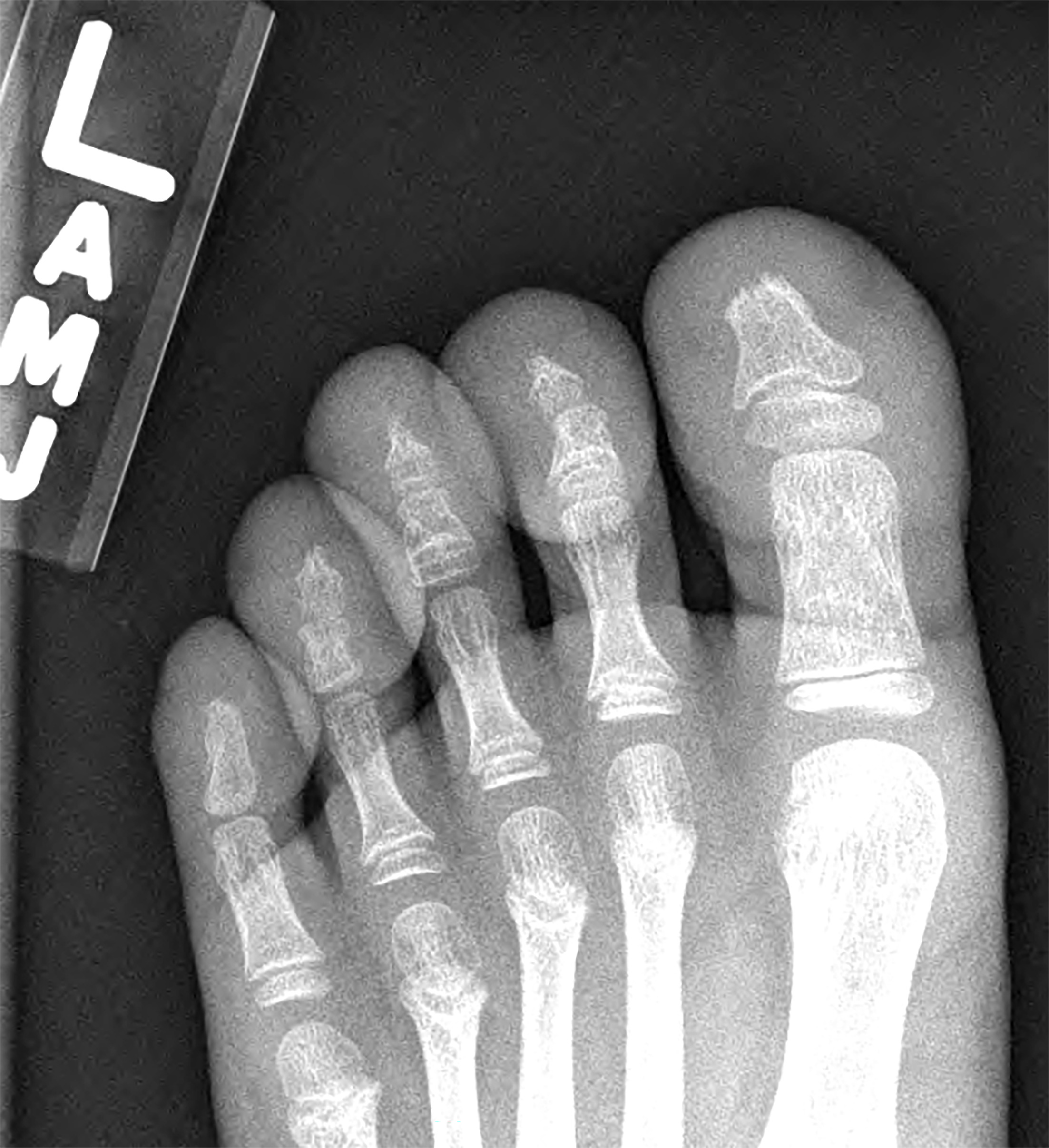
A skeletal survey (Figure 2) confirmed the findings of the hands and highlighted similar findings of the feet with loss of tuft integrity of the distal phalanx of the great toes and pencil deformity of the distal phalanges of the 2nd, 3rd, and 4th toes. There was soft-tissue swelling of virtually every toe. Long-term follow-up radiographs of the feet (at age 15) and hands (at age 21) showed progression of findings (Figures 3, 4).


Diagnosis
Acroosteolysis due to primary hypertrophic osteoarthropathy.
The differential diagnosis of acroosteolysis includes Hajdu-Cheney syndrome, hyperparathyroidism, scleroderma, diabetes, psoriasis, and polyvinyl chloride exposure.
Discussion
Idiopathic hypertrophic osteoarthropathy or PHO, also known as pachydermoperiostosis, was first described in the mid-19th century. 1 In 1935, 3 different forms of PHO were described. The complete form is the most severe type and consists of pachydermia (coarsening of facial features), periostosis (new bone growth), and clubbing of the digits. 1,2 In the incomplete form, the scalp is not involved. Finally, in forme fruste, PHO clubbing and pachydermia are present; however, there is minimal periostitis. 1 PHO has been distinguished from secondary hypertrophic osteoarthropathy, which is associated with underlying cardiac or pulmonary disease. 2,3
PHO is a rare condition that is more severe and 9 times more common in males. 1,4 Only one-third of the affected patients have a positive family history. 1 The condition typically presents during childhood or puberty, after which it progresses for approximately 10 years. PHO is self-limiting, becoming static or resolving spontaneously after adolescence. 3 Symptoms include arthralgia, hyperhidrosis, acne, and blepharoptosis. 1-3 Acroosteolysis, or bone resorption of the distal phalanges, may also be present. 1,2
Inheritance patterns of PHO vary due to the underlying genetic mutation. Mutations in the 15-hydroxyprostaglandin dehydrogenase (HPDG) and solute carrier organic anion transporter family 2A1 (SLCO2A1) genes lay at the root of the condition. HPDG-related PHO has autosomal-recessive inheritance, while SLCO2A1-related PHO can be either autosomal recessive or dominant. 1,2,5 Mutations in the HPDG and SLCO2A1 genes lead to increased levels of prostaglandin E2, causing an increase in osteoclast activity and therefore bone resorption. 4 Ultimately, vascular endothelial growth factor is released, causing vascular hyperplasia, bone growth and loss, and edema. 4
The radiographic pattern of acroosteolysis can help distinguish the different potential entities. In PHO, the tufts of the fingers and toes are affected, with acroosteolysis occurring first in the lower extremities and later in the upper extremities. 4 A key differentiating feature of PHO is terminal resorption, which rules out potential inflammatory causes, such as psoriatic arthritis. However, tuft resorption is not unique to PHO. This finding also may be seen in hormonal disorders such as secondary hyperparathyroidism and neuropathic disorders that lead to repetitive trauma (such as tabes dorsalis and diabetic neuropathy). 2,6 Compared with these other causes, patients with PHO also have shaggy periostosis, affecting the diaphysis of long bones. 3 Depending on the severity, the metaphyses and epiphyses may also be affected. 3 Other imaging modalities such as MR, bone scintigraphy, and PET can highlight the periosteal changes. However, radiographs remain the preferred method of imaging due to their high level of detail and accessibility. 2,3
There is no curative treatment for PHO. Instead, treatment is focused on symptomatic areas. For example, painful synovial effusions can be treated with nonsteroidal anti-inflammatory drugs. In rare cases of excessive periosteal reaction, surgery is an option. Patient outcomes vary depending on the underlying cause.
Conclusion
PHO is a condition associated with pachydermia, periostosis, and clubbing of the digits. Patients typically present during school age or adolescence with arthralgia, hyperhidrosis, and acne. PHO occurs more commonly and more severely in males. Acroosteolysis is a common radiographic feature. Key features differentiating PHO from other causes of acroosteolysis include terminal tuft resorption and periostitis. The condition is typically self-limiting.
References
- Poormoghim H, Hosseynian A, Javadi A. Primary hypertrophic osteoarthropathy. Rheumatol Int. 2012;32(3):607-610. doi:10.1007/s00296-010-1667-z.
- Limenis E, Stimec J, Kannu P, Laxer R. Lost bones: differential diagnosis of acro-osteolysis seen by the pediatric rheumatologist. Pediatr Rheumatol Online J. 2021;19(1). doi:10.1186/s12969-021-00596-0.
- Zhang Z, Zhang C, Zhang Z. Primary hypertrophic osteoarthropathy: an update. Front Med. 2013;7(1):60-64. doi:10.1007/s11684-013-0246-6.
- Martínez-Lavín M. Hypertrophic osteoarthropathy. Best Pract Res Clin Rheumatol. 2020;34(3):101507. doi:10.1016/j.berh.2020.101507.
- Xu Y, Zhang Z, Yue H, Li S, Zhang Z. Monoallelic mutations in SLCO2A1 cause autosomal dominant primary hypertrophic osteoarthropathy. J Bone Miner Res. 2021;36(8):1459-1468. doi:10.1002/jbmr.4310.
- Kemp S. Acro-osteolysis: etiologic and radiological considerations. JAMA. 1986;255(15). doi:10.1001/jama.1986.03370150100036.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Acroosteolysis: Primary Hypertrophic Osteoarthropathy. Applied Radiology. 2025;1(1):1-2. doi:10.37549/JPCR-25-0020.