Anterior Mediastinal Mass
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -4
Published: September 1, 2025
1 University of Central Florida College of Medicine, Orlando, Florida
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Lymphomas of the anterior mediastinum are more prevalent in the pediatric population compared to the adult population, necessitating the need for accurate differential diagnostic strategies. LBL, HL, and PMBCL are commonly diagnosed malignancies of the mediastinum. The masses are imaged to identify distinguishing features to determine an initial diagnosis, with a biopsy used to confirm the diagnosis. Minimally invasive, image guided biopsy is preferred. If non-diagnostic, surgical approaches can be used to obtain a histologic sample.
Keywords
lymphoma, neoplasm
Categories
Case Summary
An adolescent boy presented with persistent fever, drenching night sweats, fatigue, splenomegaly, and lymphadenopathy. His symptoms began 5 months earlier after a mononucleosis infection.
Imaging Findings
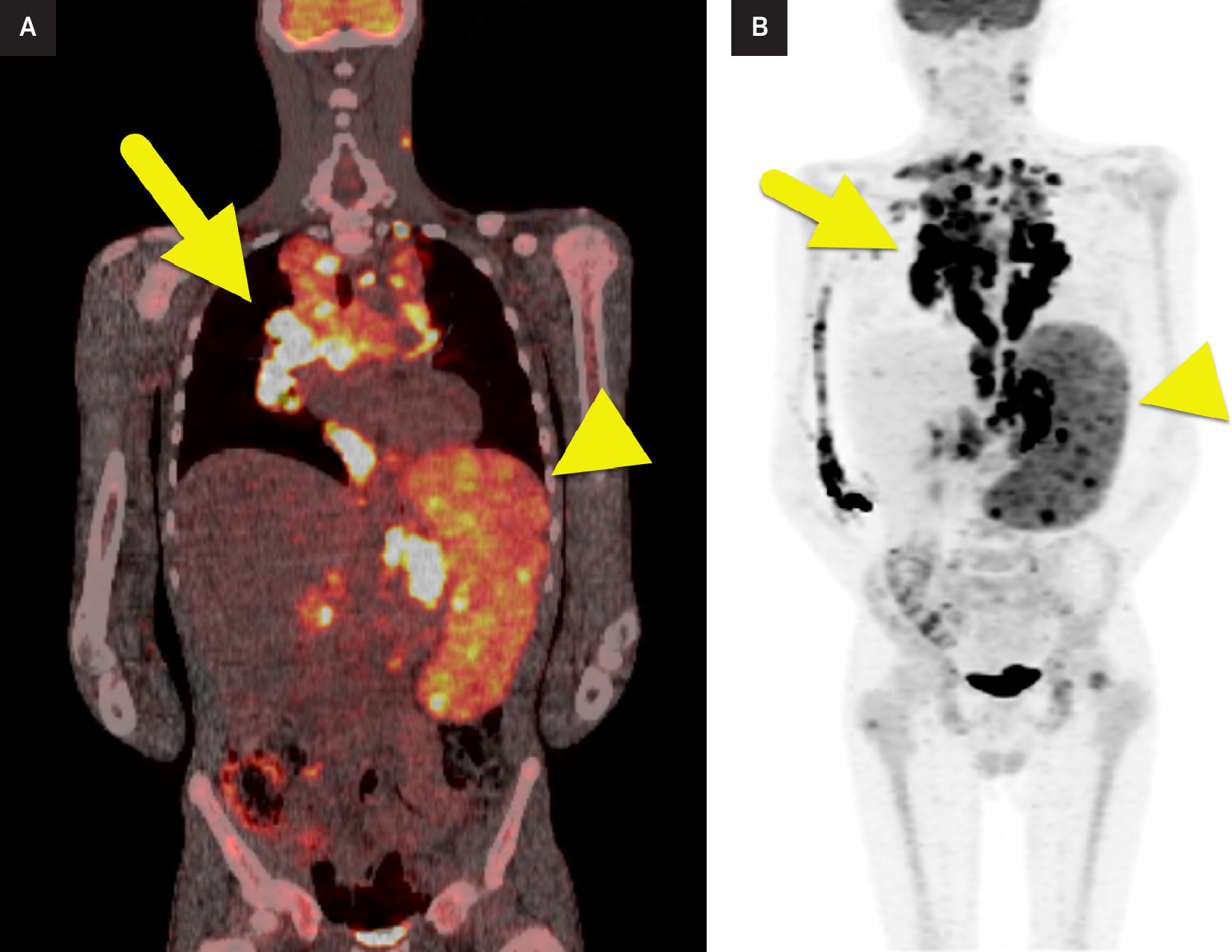
Chest radiograph showed a mediastinal mass with irregular, lobulated borders. Chest CT confirmed the large mediastinal mass that occupied more than one-third the diameter of the chest. F-18 fluorodeoxyglucose (FDG) PET-CT showed the mediastinal mass to be FDG-avid with a maximum standardized uptake value of 15. The spleen was enlarged and FDG avid.
Diagnosis
Hodgkin lymphoma.
Based on the age of the patient, the differential diagnosis includes lymphomas such as lymphoblastic lymphoma (LBL), non-Hodgkin lymphoma (NHL), and primary mediastinal large B cell lymphoma (PMBCL), along with thymoma, teratoma, and thyroid tumors.
Discussion
The mediastinum is the area of the thoracic cavity and is divided into various compartments. The International Thymic Malignancy Interest Group developed divisions to help guide diagnosis and imaging of masses and other pathologies in this region. The anterior mediastinum consists of the thymus, lymph nodes, and mammary vessels. The middle mediastinum contains the heart, roots of the great vessels, trachea, and mainstem bronchi. The posterior mediastinum encompasses the esophagus, descending thoracic aorta, azygos and hemiazygos veins, thoracic duct, and lymphatics. 1
Anterior mediastinal masses are initially recognized by the presence of abnormal or enlarged soft tissue in chest radiography. The mass displaces the lung from structures such as the aorta and heart borders, leading to “silhouette signs,” or the absence of normally visualized thoracic structure borders. CT with intravenous contrast is most used to establish a differential diagnosis. Various imaging features (such as the demonstration of lymphadenopathy for Hodgkin lymphoma [HL] or a large mass with pleural effusion for lymphoblastic NHL) with accompanying clinical symptoms can help distinguish potential diagnoses. MRI or PET/CT is less commonly used but can also assist in diagnosis. 1
Initial diagnosis of masses in the anterior mediastinum is made based on multiple factors, including symptom severity, age, sex, and clinical presentation. Dyspnea, hoarseness, or dysphagia may indicate compression of surrounding organs by any type of mass. Constitutional symptoms such as fever, night sweats, and weight loss suggest lymphoma or other malignancy. Lymphomas are most common in young adulthood and patients above the age of 50 and often present with more aggressive symptoms. Thymomas are common in patients above the age of 40 and often coexist with paraneoplastic syndromes. Teratomas are more common in young women and have a relatively good prognosis. NHL often has rapid onset of symptoms, followed by HL and PMBCL, with thymomas and teratomas having a much slower chronic onset of symptoms. Family history, histopathology, and tumor markers are also valuable tools to help elucidate the diagnosis. 2,3
Mediastinal lymphomas are common in the pediatric population, making up about 50% of mediastinal tumors in children compared with 12% in adults. 1 The most common form of lymphoma in the pediatric age group, up to about 14 years of age, is LBL, followed by HL and PMBCL in older teenagers. Gray zone lymphoma, which exhibits features of both HL and PMBCL, and other NHLs are rare in the pediatric population. 4
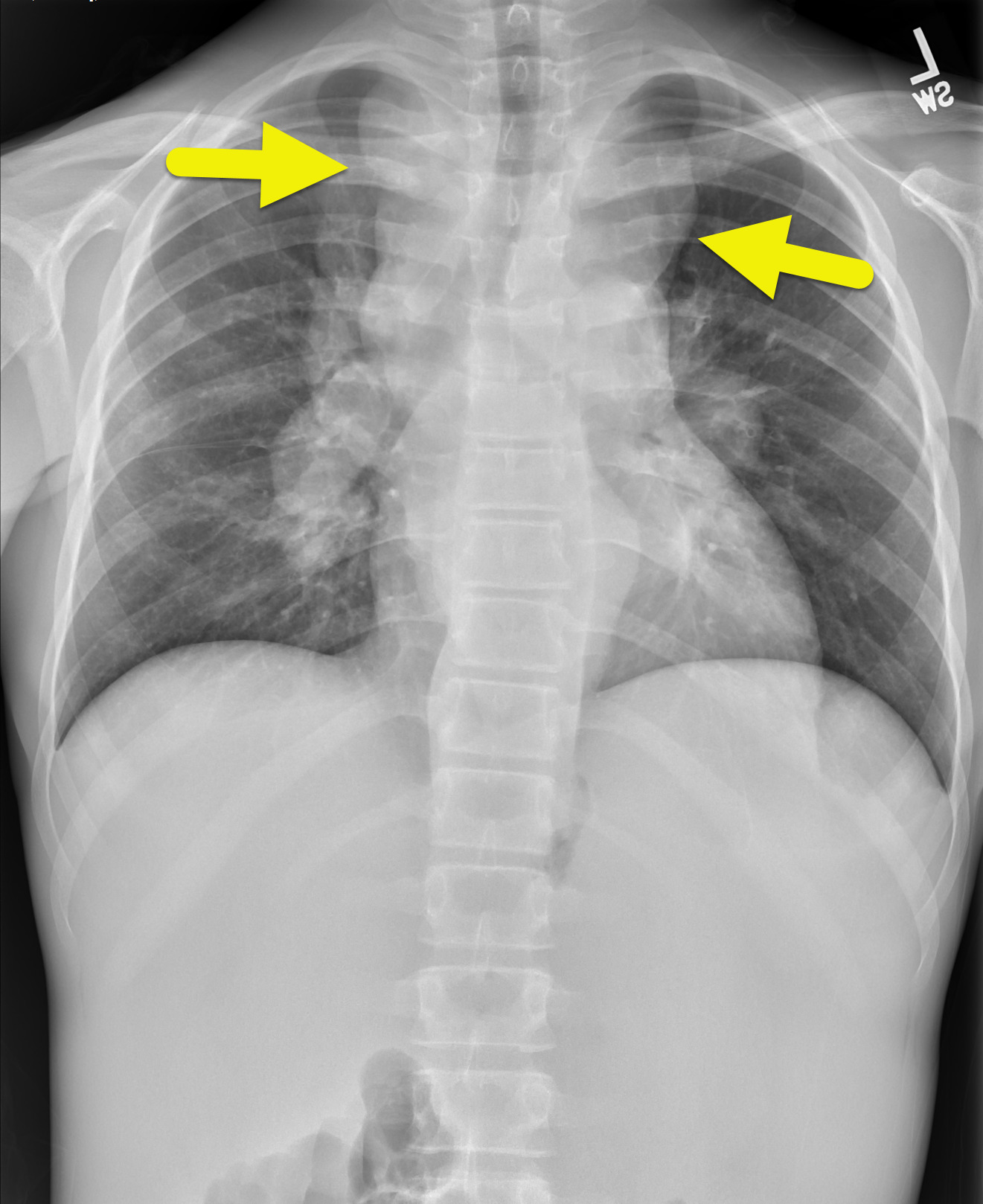
Radiography is the initial diagnostic tool utilized for anterior mediastinal masses (Figure 1). Radiographs can be used to detect abnormal or soft tissue masses, by displacement of the lung from structures such as the aorta and heart borders, or the absence of normal thoracic anatomic borders. 1
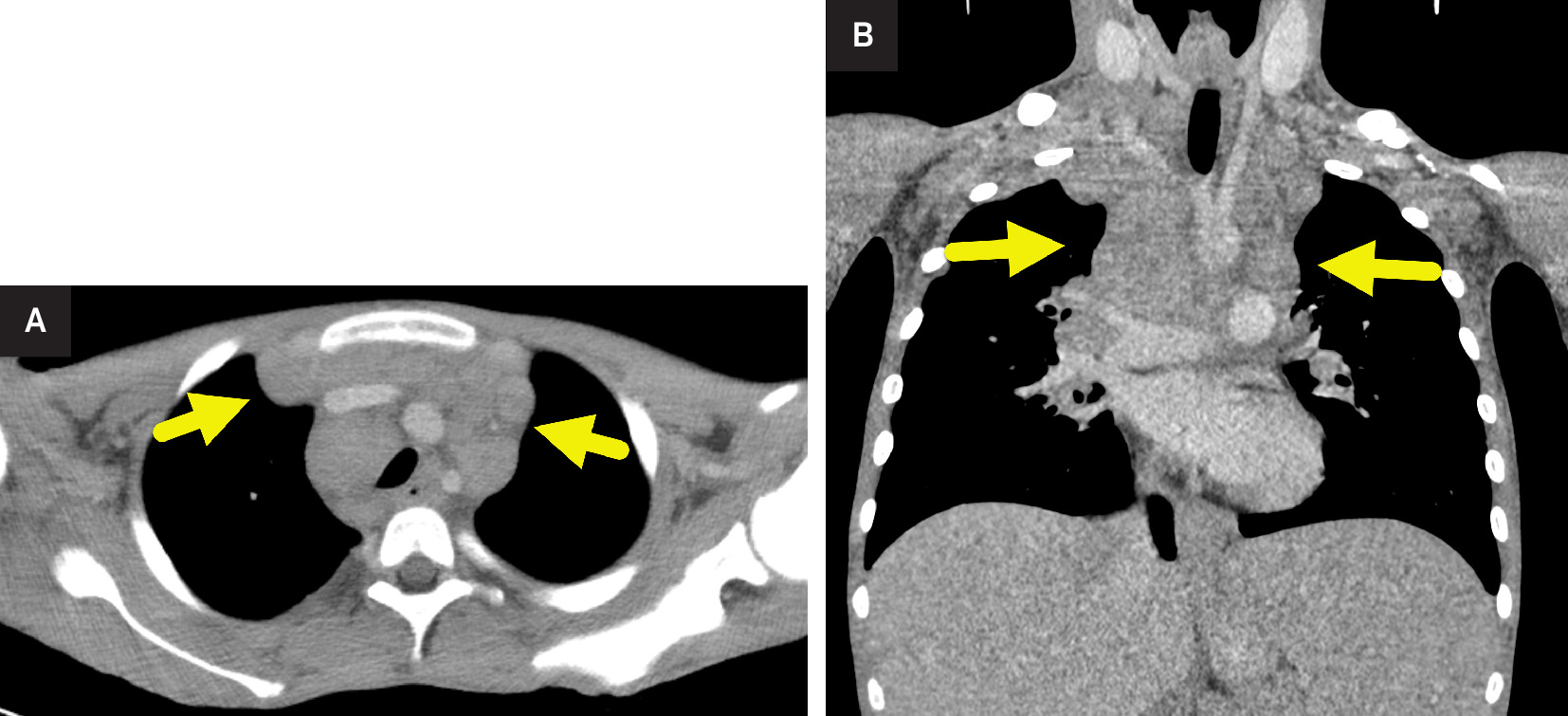
CT is the preferred modality for diagnosis and determination of the extent of disease in children with suspected lymphoma (Figure 2). Patients with mediastinal LBL often present with a pericardial effusion along with cervical or abdominal lymphadenopathy and splenomegaly. Extranodal sites, including skin and bone, are often affected. However, head and neck involvement is uncommon. The nodal masses are often large and invasive and may have evidence of hemorrhage, necrosis, or cystic degeneration. MRI may show T1 and T2 hyperintensity and no significant contrast enhancement. 4
Like LBL, HL can also present with lymphadenopathy and pleural effusion. HL can be differentiated by its irregular contour and surface lobulations. Lack of vascular invasion and extranodal involvement (~1-4% of the time) are rare. Thus, nodal masses are largely located above the diaphragm and confined to the neck and mediastinum. 5 On CT, the nodal mass is not generally as large and aggressive as LBL. On MRI, T1W images are isointense to muscle. 6,7
PMBCL shares some features of LBL and HL with the presence of pericardial effusion and irregular contour on CT but can be differentiated by the presence of vascular involvement in 20-30% of patients and usually confined to the abdomen, including kidneys, ovaries, and liver when present. 5 PMBCL typically presents as well defined with significant enhancement due to the high vascularity of the tumor on CT and with intermediate to low signal intensity on T1W MRI images due to the solidity and cellular density of the tumor. 6,8
Teratomas typically present on CT with fat, fluid, and calcified components. Thymomas commonly present as a component of paraneoplastic syndromes such as myasthenia gravis and hypogammaglobulinemia and demonstrate sharp margins and enhancement on CT. 3
PET-CT is also used to differentiate between benign and malignant mediastinal masses by quantifying the amount of metabolic activity. HL and NHL exhibit varying levels of radiotracer uptake, while thymomas tend to show lower overall uptake. PET-CT can also help identify the most metabolically active areas of a mass to target in a biopsy. In malignant masses, it can be used to help stage the cancer and also can be used to assess treatment response following diagnosis. 9
Once a mass is identified, a biopsy is used when the clinical picture and imaging need confirmation. Whenever possible, an image-guided percutaneous biopsy is preferred for histologic examination as endoscopic and open surgical procedures are more invasive, have higher complication rates, and are more costly. 10,11 Thus, image-guided percutaneous approaches have become the initial procedure of choice. This approach minimizes invasiveness and has been shown in several studies to have higher diagnostic accuracy and lower cost. 7,12,13 In addition to the minimal invasiveness, image-guided biopsy also benefits from visualization of the needle tip and normal structures surrounding the mass, resulting in lower rates of complications. 14 Studies using the percutaneous, image-guided approach have also demonstrated decreased procedure time and improved diagnostic yield rates. 10 If a percutaneous approach is deemed to be unsuitable or nondiagnostic, thoracoscopy, mediastinoscopy, and mediastinotomy may be performed to acquire tissue for pathologic evaluation. Endoscopic transbronchial or transesophageal procedures can also be performed but are reserved for selected occasions when other approaches are unsuccessful or not feasible. 10,11 These surgical methods are not usually the initial diagnostic approach due to the higher rate of major complications. 14
Conclusion
Lymphomas of the anterior mediastinum are more prevalent in the pediatric population compared with the adult population, necessitating the need for accurate differential diagnostic strategies. LBL, HL, and PMBCL are commonly diagnosed malignancies of the mediastinum. The masses are imaged to identify distinguishing features to determine an initial diagnosis, with a biopsy used to confirm the diagnosis. Minimally invasive, image-guided biopsy is preferred. If nondiagnostic, surgical approaches can be used to obtain a histologic sample.
References
- Carter B, Okumura M, Detterbeck F, Marom E. Approaching the patient with an anterior mediastinal mass: a guide for radiologists. J Thorac Oncol. 2014;9(9 suppl 2):S110-8. doi:10.1097/JTO.0000000000000295.
- Almeida P, Heller D. Statpearls. 2024.
- Verma S, Kalra K, Rastogi S, Sidhu H. Clinical approach to childhood mediastinal tumors and management. Mediastinum. 2020;4. doi:10.21037/med-19-82.
- Dvorak P, Hoffmann P, Kocova E, Habal P, Nova M. CT-guided biopsy of the mediastinal masses. Can anatomical relationships predict complications?. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2019;163(3):220-226. doi:10.5507/bp.2018.058.
- Wang Y, Chen M, Ni C. Case report: primary mediastinal large b-cell lymphoma invasion of extranodal thyroid tissue mimicking tuberculosis and confounded by similar ultrasonic appearance. Front Oncol. 2022;12:879295. doi:10.3389/fonc.2022.879295.
- Ong C, Teo L. Imaging of anterior mediastinal tumours. Cancer Imaging. 2012;12(3):506-515. doi:10.1102/1470-7330.2012.0039.
- Burgard C, Stahl R, de Figueiredo G. Percutaneous ct fluoroscopy-guided core needle biopsy of mediastinal masses: technical outcome and complications of 155 procedures during a 10-year period. Diagnostics (Basel). 2021;11(5). doi:10.3390/diagnostics11050781.
- Silva T, Ferreira C, Leite G, de Menezes Pontes J, Antunes H. Oral manifestations of lymphoma: a systematic review. Ecancermedicalscience. 2016;10. doi:10.3332/ecancer.2016.665.
- Reddy R. Comparative role of MDCT and FDG-PET/CT in the diagnostic evaluation of mediastinal mass lesions: an institutional experience. World J Nucl Med. 2022;21(3):200-209. doi:10.1055/s-0042-1751032.
- Iguchi T, Hiraki T, Matsui Y. CT fluoroscopy-guided core needle biopsy of anterior mediastinal masses. Diagn Interv Imaging. 2018;99(2):91-97. doi:10.1016/j.diii.2017.10.007.
- Mallick S, Jain S, Ramteke P. Pediatric mediastinal lymphoma. Mediastinum. 2020;4. doi:10.21037/med-20-37.
- Navin P, Eickstaedt N, Atwell T. Safety and efficacy of percutaneous image-guided mediastinal mass core-needle biopsy. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1100-1108. doi:10.1016/j.mayocpiqo.2021.09.006.
- Sklair-Levy M, Polliack A, Shaham D. CT-guided core-needle biopsy in the diagnosis of mediastinal lymphoma. Eur Radiol. 2000;10(5):714-718. doi:10.1007/s003300050991.
- Nakazono T, Yamaguchi K, Egashira R. MRI findings and differential diagnosis of anterior mediastinal solid tumors. Magn Reson Med Sci. 2023;22(4):415-433. doi:10.2463/mrms.rev.2021-0098.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Anterior Mediastinal Mass. Applied Radiology. 2025;1(1):1-4. doi:10.37549/JPCR-25-0012.