Aortic Stenosis
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -3
Published: September 1, 2025
1 Midwestern University Chicago College of Osteopathic Medicine, Downers Grove, Illinois
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Cardiology, Le Bonheur Hospital, Memphis, Tennessee
4 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pediatric Aortic Stenosis (AS) should be suspected in children with fatigue, dizziness, cyanosis, and chest pain. AS can be associated with other congenital heart conditions. Echocardiogram is the first-line imaging study. Up to 40% of patients require intervention, generally involving repair and/or replacement of the aortic valve.
Keywords
congenital heart defect
Categories
Case Summary
A teenage boy presented with chest pain and shortness of breath during exercise. His physical exam was notable for normal vital signs, but a II/VI systolic ejection murmur was present at the right upper sternal border.
Imaging Findings
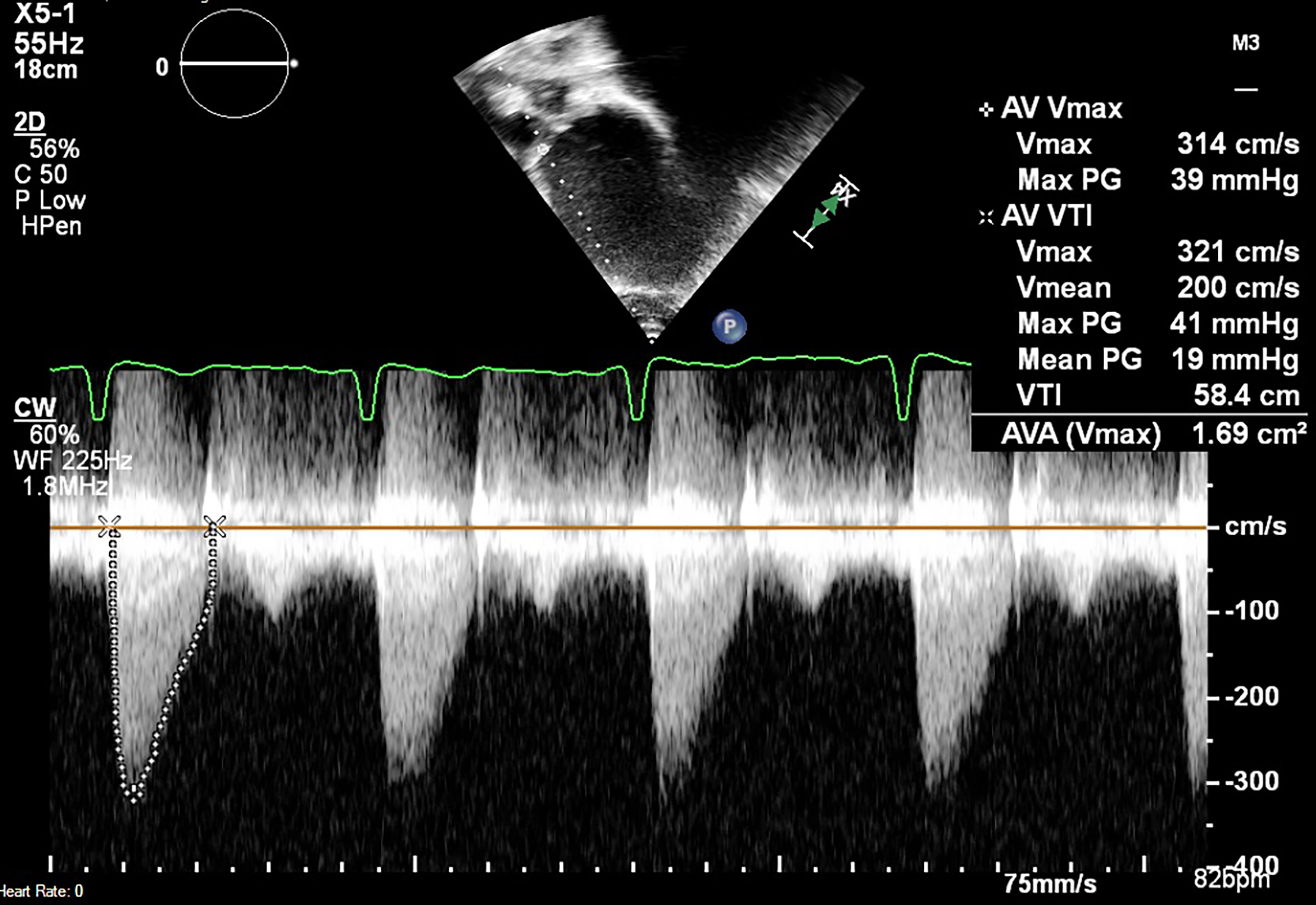
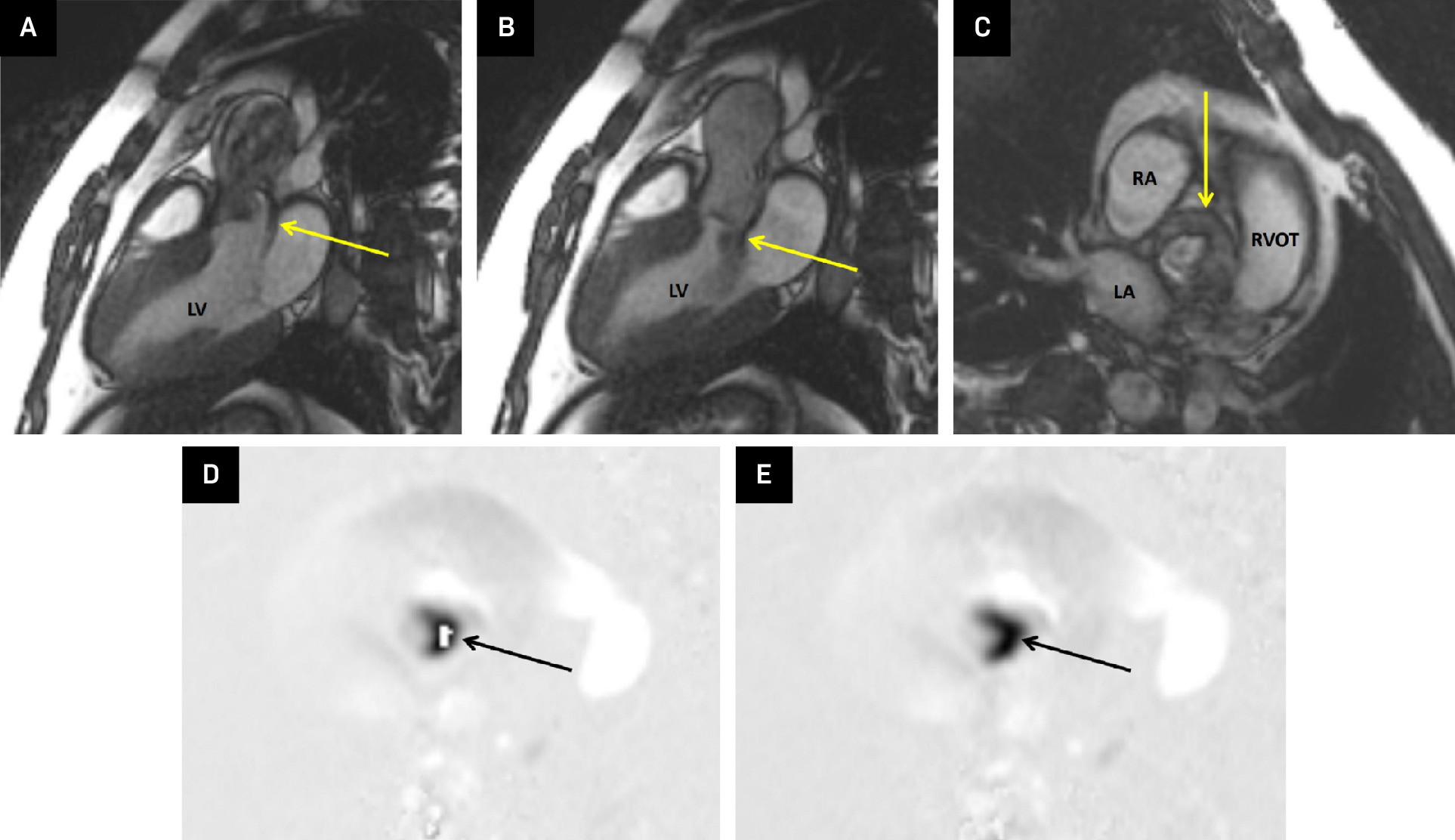
Transthoracic echocardiogram (Figure 1) showed a bicuspid aortic valve with stenosis and normal left ventricular systolic function. Cardiac MRI confirmed the presence of a bicuspid aortic valve with moderate aortic stenosis (Figure 2) and moderate insufficiency. There was mild left ventricular chamber dilation and normal systolic function.
Diagnosis
Aortic stenosis.
The differential diagnosis is primarily hypertrophic obstructive cardiomyopathy.
Discussion
In pediatric patients, aortic valve stenosis (AS) is a congenital heart defect that creates left ventricular outflow tract obstruction. 1 In neonates, this obstruction leads to an increase in afterload after birth as the low-resistance placental circulation is removed. The loss of the placental circulation, along with the closure of the ductus arteriosus, leads to a drop in systemic cardiac output and the subsequent development of congestive heart failure. 1
AS is more common in males and accounts for about 3-6% of congenital heart defects. Affected patients present with fatigue, dizziness, cyanosis, and chest pain. Approximately 15-20% of children with AS have associated congenital heart diseases such as ventricular septal defects and coarctation of the aorta. 2 Several congenital etiologies can cause AS. While supravalvular and subvalvular stenosis can occur in conditions such as Williams syndrome, true valvular stenosis is the most common cause of AS. 3 Of the valvular etiologies, 60% of cases are due to a congenital bicuspid aortic valve. While less common, rheumatic heart disease can cause an acquired AS. When affected in rheumatic heart disease, the aortic valve can become thickened, with shortened cusps and fused commissures. 3
Transthoracic echocardiography is the preferred imaging modality to assess patients with known or suspected AS. The focus of the echocardiogram is to assess the extent of left ventricular hypertrophy and the ejection fraction during systole. 3 When assessing a bicuspid aortic valve, it is important to identify systolic “doming” of the valve leaflets. When this occurs, the leaflets take a concave shape in respect to the orifice due to restricted excursion. 4 Other important findings include an abnormal number and division of valve commissures and cusp fusion, which may give a false appearance of a tricuspid valve. 4 In assessing the severity of the stenosis, Doppler flow can be used to estimate the degree of stenosis through measurement of the jet velocity and mean gradient. A jet velocity of 2.6-2.9 m/second and mean gradient of <30 mm Hg is indicative of mild AS. Moderate AS is shown with a jet velocity of 3.0-4.0 m/second and a mean gradient of 30-50 mm Hg. Anything greater than this is considered severe AS. 5 While chest radiographs and CT scans can be used to assess the extent of calcification in the aortic valve leaflets, this is a rare finding in the pediatric population and more commonly utilized in adult-onset AS. 3
Cardiac MRI allows for more detailed dynamic assessment of the left ventricle and aortic valve via improved soft-tissue definition. On cardiac MRI, the radiologist or cardiologist should look for increased left ventricular wall thickness (>12 mm), increased left ventricular mass, and post-stenotic dilatation of the ascending aorta distal to the stenotic valve. 3
Cardiac catheterization is the gold standard modality used to assess and potentially treat AS in children. During this procedure, the cardiac interventionalist can directly measure pressures across the aortic valve. However, in most instances, cardiac catheterization is only used when there are discrepancies between echocardiogram, when the noninvasive imaging has shown to be inconclusive, or balloon angioplasty is indicated to treat AS. 6
Currently, there are 2 major interventions indicated for children with AS: balloon aortic valvuloplasty and surgical repair. 7 In a large follow-up study with patients aged 1 month to 23 years, 10- and 20-year freedom from reintervention was 54% and 27%, respectively. Groups at greatest risk of restenosis are those aged 3 months or younger and those with an immediate post-valvuloplasty mean gradient of >30 mm Hg. 8
Surgical options include aortic repair, where fibrous excess is removed, or valve replacement for patients with an uncorrectable valve. Those with a bicuspid aortic valve with significant dysfunction and dilation >4.5 cm will likely need a valve replacement. 1 The 10-year freedom from reintervention for patients who underwent a surgical valvuloplasty was about 73%. 9 While the surgical option provides a higher rate of freedom from reintervention, it is associated with greater morbidity and an extended hospital stay compared with balloon valvuloplasty. 1
Conclusion
Pediatric AS should be suspected in children with fatigue, dizziness, cyanosis, and chest pain. AS can be associated with other congenital heart conditions. Echocardiogram is the first-line imaging study. Up to 40% of patients require intervention, generally involving repair and/or replacement of the aortic valve.
References
- Singh G. Congenital aortic valve stenosis. Children (Basel). 2019;6(5). doi:10.3390/children6050069.
- Sievers H, Stierle U, Mohamed S. Toward individualized management of the ascending aorta in bicuspid aortic valve surgery: the role of valve phenotype in 1362 patients. J Thorac Cardiovasc Surg. 2014;148(5):2072-2080. doi:10.1016/j.jtcvs.2014.04.007.
- Sorrentino S, Yap J, Weerakkody Y. Aortic valve stenosis. Reference article, Radiopaedia.org.
- Weerakkody Y, Yap J, Rogalskyi V. Bicuspid aortic valve. Reference article, Radiopaedia.org.
- Graham T, Driscoll D, Gersony W. Task force 2: congenital heart disease. J Am Coll Cardiol. 2005;45(8):1326-1333. doi:10.1016/j.jacc.2005.02.009.
- Brito J, Raposo L, Teles R. Invasive assessment of aortic stenosis in contemporary practice. Front Cardiovasc Med. 2022;9. doi:10.3389/fcvm.2022.1007139.
- Jone P, Haak A, Petri N. Echocardiography-fluoroscopy fusion imaging for guidance of congenital and structural heart disease interventions. JACC Cardiovasc Imaging. 2019;12(7 pt 1):1279-1282. doi:10.1016/j.jcmg.2018.11.010.
- Brown D, Dipilato A, Chong E, Lock J, McElhinney D. Aortic valve reinterventions after balloon aortic valvuloplasty for congenital aortic stenosis intermediate and late follow-up. J Am Coll Cardiol. 2010;56(21):1740-1749. doi:10.1016/j.jacc.2010.06.040.
- Carrel T, Kadner A. Long-term clinical and imaging follow-up after reinforced pulmonary autograft ross procedure. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2016;19(1):59-62. doi:10.1053/j.pcsu.2015.11.005.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Aortic Stenosis. Applied Radiology. 2025;1(1):1-3. doi:10.37549/JPCR-25-0002.