Arthrogryposis Multiplex Congenita
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 1, 2026
1 University of Arizona College of Medicine, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Arthrogryposis multiplex congenita (AMC) is a multietiologic congenital syndrome resulting from decreased fetal movement and defined by joint contractures involving 2 or more body regions. The 6 major etiologic categories include neuropathic abnormalities, muscle abnormalities, connective tissue abnormalities, uterine space limitations, intrauterine vascular compromise, and maternal disease. Prenatal US most commonly detects joint contractures during the second or third trimester, although first-trimester findings such as increased nuchal translucency or congenital anomalies may suggest the diagnosis earlier. In cases where fetal movement is not assessed, diagnosis may be delayed until birth. Careful attention to imaging findings is essential when evaluating any pregnancy in which decreased fetal movement is reported or AMC is suspected.
Keywords
musculoskeletal, syndrome, congenital
Categories
Clinical Summary
A G5P2 woman presented for level 2 US at 25 weeks of gestation after club foot was identified on level 1 US.
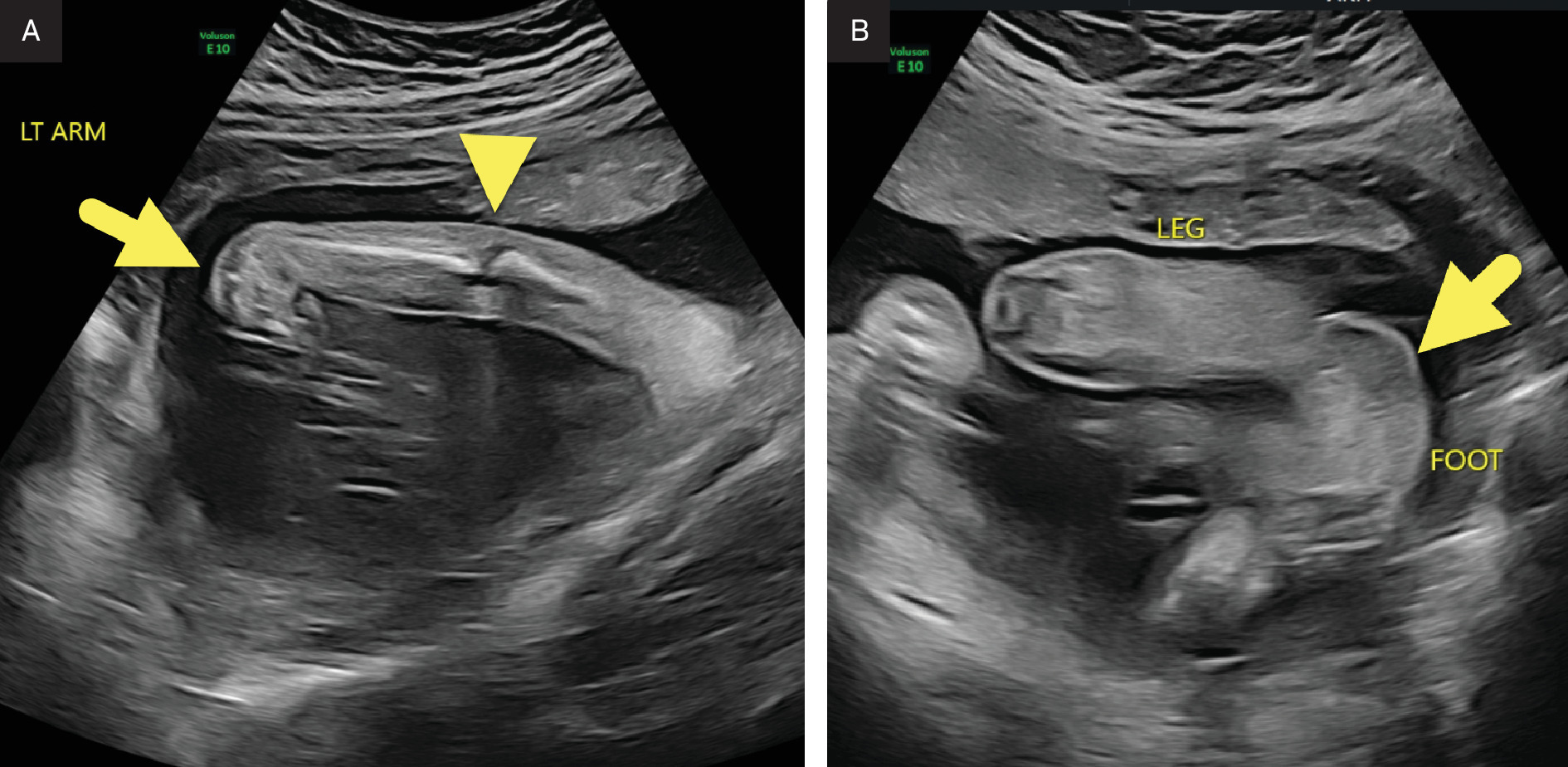
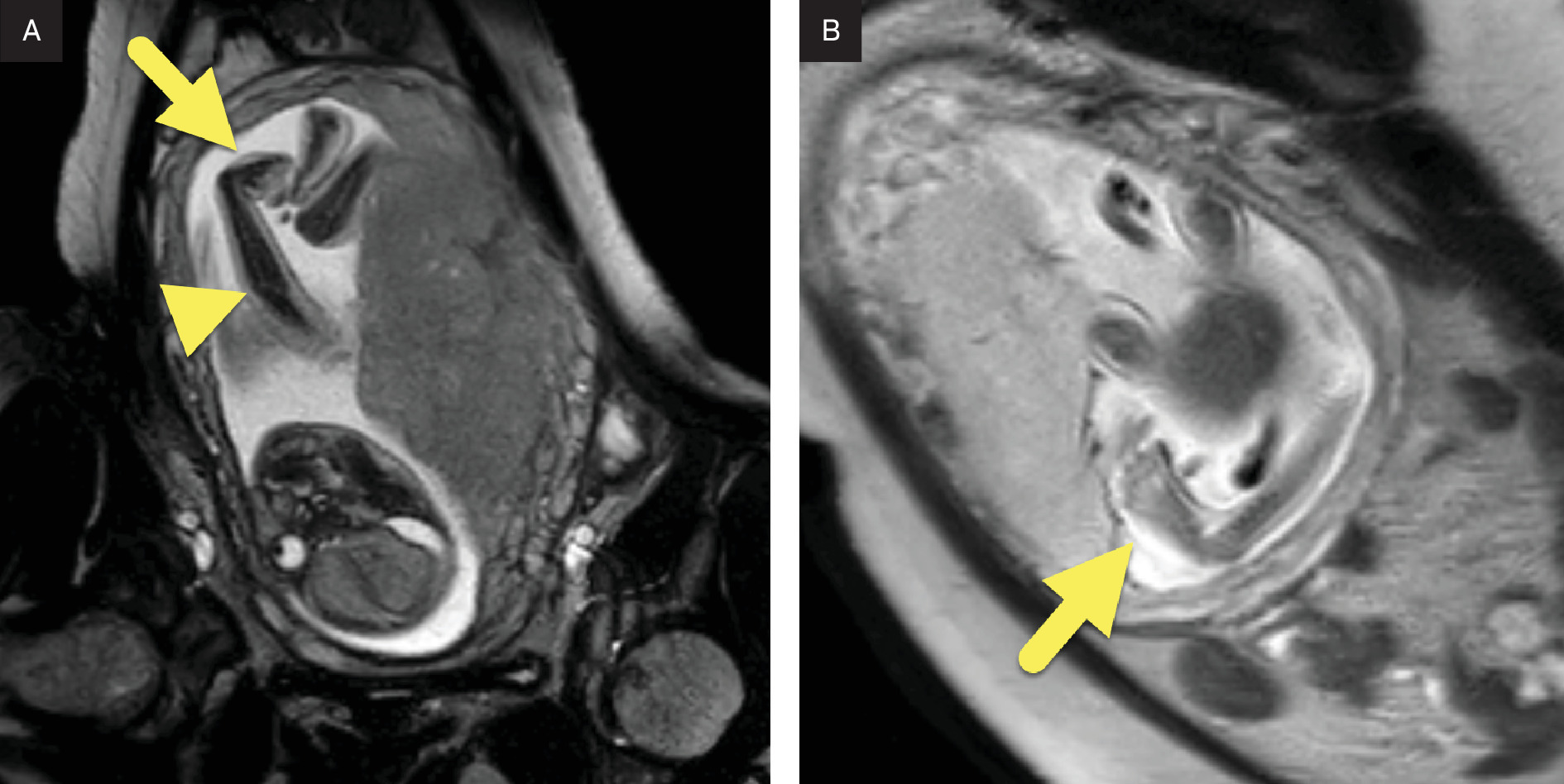
Imaging Findings
Fetal US (Figure 1) and MRI (Figure 2) showed fixed extension of the elbows and flexion of the wrists. Bilateral clubfoot was also present.
Diagnosis
Arthrogryposis multiplex congenita (AMC) is an umbrella term encompassing a wide range of congenital conditions characterized by multiple joint contractures.
The differential diagnosis is broad and includes distal arthrogryposis, congenital bony fusions, contractural arachnodactyly, multiple pterygium syndrome, and other disorders that affect both the limbs and additional organ systems.
Discussion
AMC is a congenital syndrome defined as a group of conditions characterized by joint contractures involving 2 or more body regions.1 The unifying mechanism across all forms of AMC is decreased fetal movement (fetal akinesia).2 When movement is restricted early in gestation, the resulting contractures are typically more severe.3 The causes of fetal akinesia are diverse and often multifactorial. However, they can generally be grouped into 6 major categories: neuropathic abnormalities, muscle abnormalities, connective tissue abnormalities, uterine space limitations, intrauterine vascular compromise, and maternal disease.2
The 6 etiologic categories of AMC encompass a wide range of underlying abnormalities. Neuropathic causes involve both the central and peripheral nervous systems and include cerebellar hypoplasia, spinal muscular atrophy (SMA), and other anterior horn cell diseases.2,4 Muscle-related causes include maternal antibody translocation in myasthenia gravis, congenital muscular dystrophies, and mitochondrial disorders.2,4 Connective tissue abnormalities may result from normal tissue forming at inappropriate attachment sites or from intrinsic connective tissue defects such as dystrophic dysplasia.2 Space limitations within the uterus, as seen with oligohydramnios, fibroids, uterine growths, or multiple gestations, can also contribute to the development of AMC.2,4 Intrauterine vascular compromise leads to decreased blood flow, which can damage fetal nerves and muscles and result in akinesia.2 Maternal factors, including infections, trauma, and exposure to teratogenic medications, have also been implicated.2,5,6 Notably, many chromosomal deletion and duplication syndromes have been associated with AMC,5 and more than 400 specific conditions and over 400 genes have been linked to its development.5,7
Individuals with AMC have restricted joint motion that may be accompanied by varying degrees of muscle weakness. These musculoskeletal abnormalities result from reduced fetal movement, which leads to fixed joint positions and muscle imbalance. In addition to limb contractures, spinal deformities such as scoliosis or kyphosis may be present at birth or develop later in childhood or adolescence. Other organ systems, including the central nervous system (CNS), respiratory, gastrointestinal, and genitourinary systems, may also be affected. Cognitive impairment can occur when the CNS is involved, but sensation is typically preserved. The overall impact on function depends on the degree of musculoskeletal and systemic involvement, with outcomes ranging from mild limitations in mobility to severe lifelong disability.1
The clinical presentation of AMC is highly variable, reflecting the diversity of underlying causes. The most common subtype, amyoplasia, accounts for approximately one-third of cases and represents the classic form of AMC. Amyoplasia is characterized by underdevelopment of skeletal muscle and replacement of muscle tissue with fibrofatty tissue. Affected patients typically demonstrate symmetric flexion of the wrists, extension of the elbows, internal rotation of the shoulders, and severe lower-extremity contractures. Additional findings may include decreased muscle bulk, body weight below the 10th percentile, shortened limbs, and dimpling over affected joints. Other presentations may involve only the limbs, primarily the distal limbs, or combinations of limb and systemic involvement, including neuromuscular disorders with associated cognitive or nervous system abnormalities.5
US is the primary tool for prenatal diagnosis of AMC.5 Findings are most often detected in the second or third trimester, typically following maternal reports of reduced fetal movement. At this stage, US can readily identify most types of arthrogryposes. The most common contracture observed is clubfoot, although additional findings may include internal rotation or adduction of the shoulders, abnormal flexion or extension of the elbows, ulnar deviation of the wrists, hip dislocation, and clenched hands.8 Earlier diagnosis is also possible, as fetal movement can be visualized by US as early as 8 weeks of gestation.8 In the first trimester, secondary findings such as increased nuchal translucency, cystic hygroma, or a hypoplastic mandible should prompt further evaluation.
In the late second and third trimesters, fetal MRI complements US by identifying potential CNS causes of AMC, including cortical atrophy, lissencephaly, spinal cord atrophy, and cerebellar or pontine hypoplasia.9 Additional prenatal MRI findings may include hypoplastic lungs, muscular atrophy, growth restriction, craniofacial abnormalities, scoliosis, a short umbilical cord, and abnormal amniotic fluid volume.8 After birth, radiographs can help identify joint dislocations, ankylosis, bony disproportion, scoliosis, or fusions. Postnatal MRI and US can further evaluate the CNS and musculature to characterize the extent and underlying cause of abnormalities.5
The prognosis of AMC varies widely and depends on the underlying etiology and the severity of contractures. Progressive neuromuscular disorders such as SMA are associated with poorer outcomes compared with contractures resulting from reversible mechanical factors such as oligohydramnios. Children with mild contractures may achieve normal development after appropriate treatment, whereas those with severe, fixed deformities often require lifelong therapy and may experience limited functional independence.2
Conclusion
AMC is a multietiologic congenital syndrome resulting from decreased fetal movement and defined by joint contractures involving 2 or more body regions. The 6 major etiologic categories include neuropathic abnormalities, muscle abnormalities, connective tissue abnormalities, uterine space limitations, intrauterine vascular compromise, and maternal disease. Prenatal US most commonly detects joint contractures during the second or third trimester, although first-trimester findings such as increased nuchal translucency or congenital anomalies may suggest the diagnosis earlier. In cases where fetal movement is not assessed, diagnosis may be delayed until birth. Careful attention to imaging findings is essential when evaluating any pregnancy in which decreased fetal movement is reported or AMC is suspected.
References
- Dahan-Oliel N, Cachecho S, Barnes D. International multidisciplinary collaboration toward an annotated definition of arthrogryposis multiplex congenita. Am J Med Genet C Semin Med Genet. 2019;181(3):288-299. doi:10.1002/ajmg.c.31721.
- Kiefer J, Hall J. Gene ontology analysis of arthrogryposis (multiple congenital contractures). Am J Med Genet C Semin Med Genet. 2019;181(3):310-326. doi:10.1002/ajmg.c.31733.
- Hall J. Arthrogryposis multiplex congenita: etiology, genetics, classification, diagnostic approach, and general aspects. J Pediatr Orthop B. 1997;6(3):159-166.
- Moessinger A. Fetal akinesia deformation sequence: an animal model. Pediatrics. 1983;72(6):857-863.
- Gordon N. Arthrogryposis multiplex congenita. Brain Dev. 1998;20(7):507-511. doi:10.1016/s0387-7604(98)00037-0.
- Hall J. Arthrogryposis (multiple congenital contractures): diagnostic approach to etiology, classification, genetics, and general principles. Eur J Med Genet. 2014;57(8):464-472. doi:10.1016/j.ejmg.2014.03.008.
- van der Linden V, Filho E, Lins O. Congenital zika syndrome with arthrogryposis: retrospective case series study. BMJ. 2016;354. doi:10.1136/bmj.i3899.
- Skaria P, Dahl A, Ahmed A. Arthrogryposis multiplex congenita in utero: radiologic and pathologic findings. J Matern Fetal Neonatal Med. 2019;32(3):502-511. doi:10.1080/14767058.2017.1381683.
- Fedrizzi E, Botteon G, Inverno M. Neurogenic arthrogryposis multiplex congenita: clinical and MRI findings. Pediatr Neurol. 1993;9(5):343-348. doi:10.1016/0887-8994(93)90102-i.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Arthrogryposis Multiplex Congenita. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0078.