Brachiocephalic Artery Compression Syndrome
Applied Radiology
Published: December 24, 2025
1 University of Arizona College of Medicine Phoenix, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children's Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Brachiocephalic artery compression syndrome occurs when the brachiocephalic artery takes an anomalous course, causing anterior compression of the trachea at the thoracic inlet. It is a syndrome of childhood due to the smaller size of the thoracic inlet. Affected patients most commonly present with stridor, recurrent respiratory tract infections, and severe respiratory distress. Other signs and symptoms include a croup-like “barking” cough, episodic apnea, difficulty feeding, and failure to thrive. CT with intravenous contrast is the preferred imaging modality and will often reveal tracheal compression at the level of the brachiocephalic artery. Treatment is centered on supportive care in patients with mild-to-moderate symptoms and aortopexy or brachiocephalic artery reimplantation in severe cases.
Keywords
vascular, compression syndrome, upper extremity
Categories
Case Summary
An adolescent male with a remote history of tracheoesophageal fistula and esophageal atresia and repair presents with dyspnea on exertion, exercise intolerance, and intermittent wheezing.
Imaging Findings
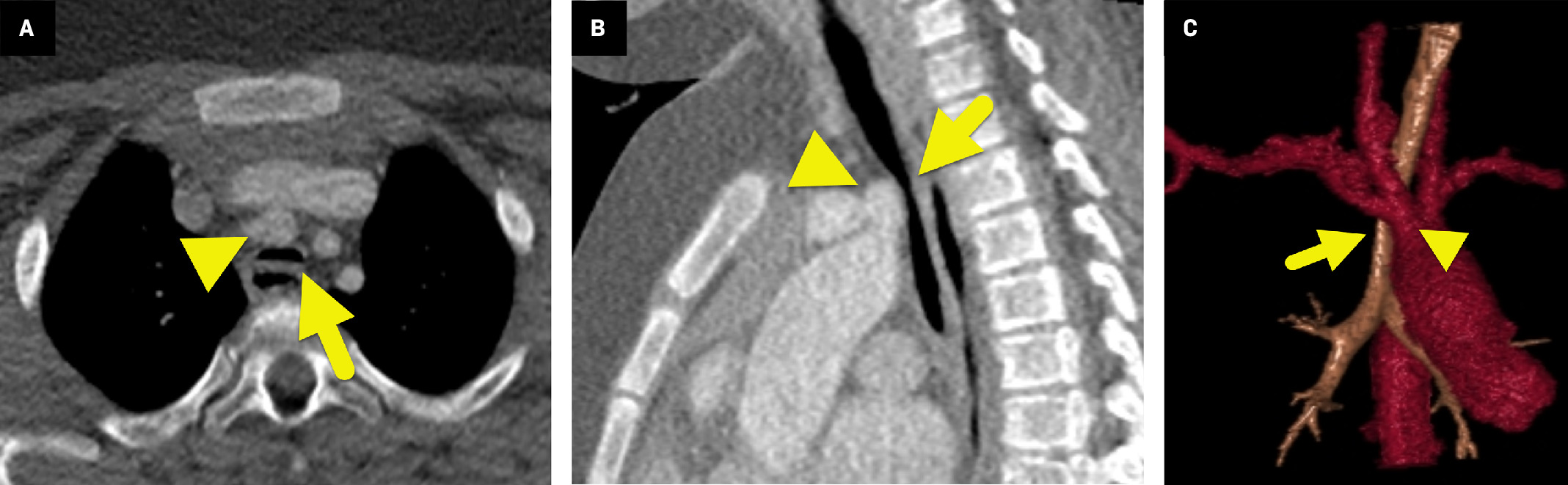
Contrast-enhanced chest CT (Figure 1) shows severe narrowing of the trachea as the brachiocephalic artery passes anteriorly into the right.
Diagnosis
Brachiocephalic (innominate) artery compression syndrome.
The differential diagnosis includes right aortic arch, double aortic arch, aberrant origin of the right subclavian artery, and pulmonary artery sling.
Discussion
Brachiocephalic artery compression syndrome is the most common vascular compression syndrome. It most often occurs when the brachiocephalic artery takes an anomalous course, originating on the left side of the trachea and crossing the anterior aspect of the airway at the level of the thoracic inlet. The course of the vessel and the related mediastinal crowding cause focal tracheal narrowing.
Affected patients are typically younger than 2 years of age. Stridor is the most common presenting symptom, though symptoms can vary depending on the child’s age and the degree of tracheal compression. While infants may have trouble feeding, vomiting, and failure to thrive, younger children may have stridor and a “croup-like barking” cough, 1 and older children may have a persistent nonproductive cough. More severe symptoms include apnea and recurrent tracheobronchitis or bronchopneumonia. However, many children (up to 30%) with mild-to-moderate tracheal narrowing are asymptomatic. 2 It is not known why some children with an anomalous course of the brachiocephalic artery have symptoms and others do not. However, brachiocephalic artery compression syndrome is thought to occur more frequently in patients with a “crowded” mediastinum, such as patients with congenital heart disease. 3 The syndrome is associated with esophageal atresia as well as severe gastroesophageal reflux. 1
Patients presenting with stridor will often initially receive chest or airway radiographs. These studies may show anterior lateral tracheal compression, deviation, and hyperinflation of the lungs. 2 Typically, the diagnosis is made via CT with intravenous contrast. However, the diagnosis can also be made via MRI (with or without intravenous contrast). Axial images show anteroposterior narrowing of the trachea where the brachiocephalic artery crosses the trachea. 4 Sagittal views may show the compression of the trachea at the same level. Bronchoscopy is considered the gold standard for diagnosis and may demonstrate an area of pulsatile compression upon the trachea that, when levered anteriorly, results in a decrease in the strength of the right radial pulse.
Most patients with brachiocephalic artery compression syndrome are treated with supportive care. Symptoms typically resolve after 2-3 years of age as the cartilaginous rings of the trachea become more rigid and less compressible, the thoracic inlet becomes wider and less crowded, and the aortic arch grows, causing the brachiocephalic artery to move away from the trachea. Patients with moderate symptoms may be treated with oxygen, steroids, and antibiotics as needed, particularly in the setting of upper respiratory infections. 5 Children who do not respond to medical therapy and have episodes of apnea, recurrent pneumonia, or tracheobronchitis are candidates for surgery. Patients with severe symptoms may be treated with aortopexy or reimplantation of the brachiocephalic artery to a more proximal site on the aorta. Relief of symptoms after surgery occurs in up to 90% of cases. The rate of complications ranges from 0% to 25% with more recent reports suggesting a rate around 2%. 6
Conclusion
Brachiocephalic artery compression syndrome occurs when the brachiocephalic artery takes an anomalous course, causing anterior compression of the trachea at the thoracic inlet. It is a syndrome of childhood due to the smaller size of the thoracic inlet. Affected patients most commonly present with stridor, recurrent respiratory tract infections, and severe respiratory distress. Other signs and symptoms include a croup-like “barking” cough, episodic apnea, difficulty feeding, and failure to thrive. CT with intravenous contrast is the preferred imaging modality and will often reveal tracheal compression at the level of the brachiocephalic artery. Treatment is centered on supportive care in patients with mild-to-moderate symptoms and aortopexy or brachiocephalic artery reimplantation in severe cases.
References
- Malik T, Bruce I, Kaushik V. The role of magnetic resonance imaging in the assessment of suspected extrinsic tracheobronchial compression due to vascular anomalies. Arch Dis Child. 2006;91(1):52-55. doi:10.1136/adc.2004.070250.
- Sachdev M, Joshi R, Kaul S, Kohli V. Innominate artery compression of trachea. Indian J Pediatr. 2007;74(8):768-769. doi:10.1007/s12098-007-0136-5.
- Lee E, Greenberg S, Boiselle P. Multidetector computed tomography of pediatric large airway diseases: state-of-the-art. Radiol Clin North Am. 2011;49(5):869-893. doi:10.1016/j.rcl.2011.06.006.
- Hegde S, Greenberg B. Newborn respiratory distress: airway abnormalities. Semin Ultrasound CT MR. 2015;36(2):138-145. doi:10.1053/j.sult.2015.01.005.
- Friedman E, Kennedy A, Neitzschman H. Innominate artery compression of the trachea: an unusual cause of apnea in a 12-year-old boy. South Med J. 2003;96(11):1161-1164. doi:10.1097/01.SMJ.0000072420.60411.9F.
- McKiernan M, Lee M. In: StatPearls [Internet].
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript, and no part of this article has been previously published elsewhere.
Citation
. Brachiocephalic Artery Compression Syndrome. Applied Radiology. 2025. doi:10.37549/JPCR-25-0068.