Bronchopulmonary Sequestration in a Fetus
Applied Radiology
Published: December 24, 2025
1 California Health Sciences University College of Osteopathic Medicine, Clovis, California
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Bronchopulmonary sequestration (BPS) is a rare congenital lung malformation characterized by its systemic arterial supply and lack of connection to the bronchial tree. There are 2 types of sequestration: intralobar and extralobar. Intralobar sequestrations are more common. Patients with this type of BPS typically present with recurrent pulmonary infection. Chest radiography is usually the initial imaging examination, followed by CT. CT is used to diagnose the aberrant venous and arterial anatomy and eliminate other disease entities. Treatment is surgical.
Keywords
fetal, congenital, pulmonary, fetal MRI
Categories
Case Summary
A fetal MRI was performed at 25 weeks’ gestational age to evaluate a congenital lung lesion identified on screening US.
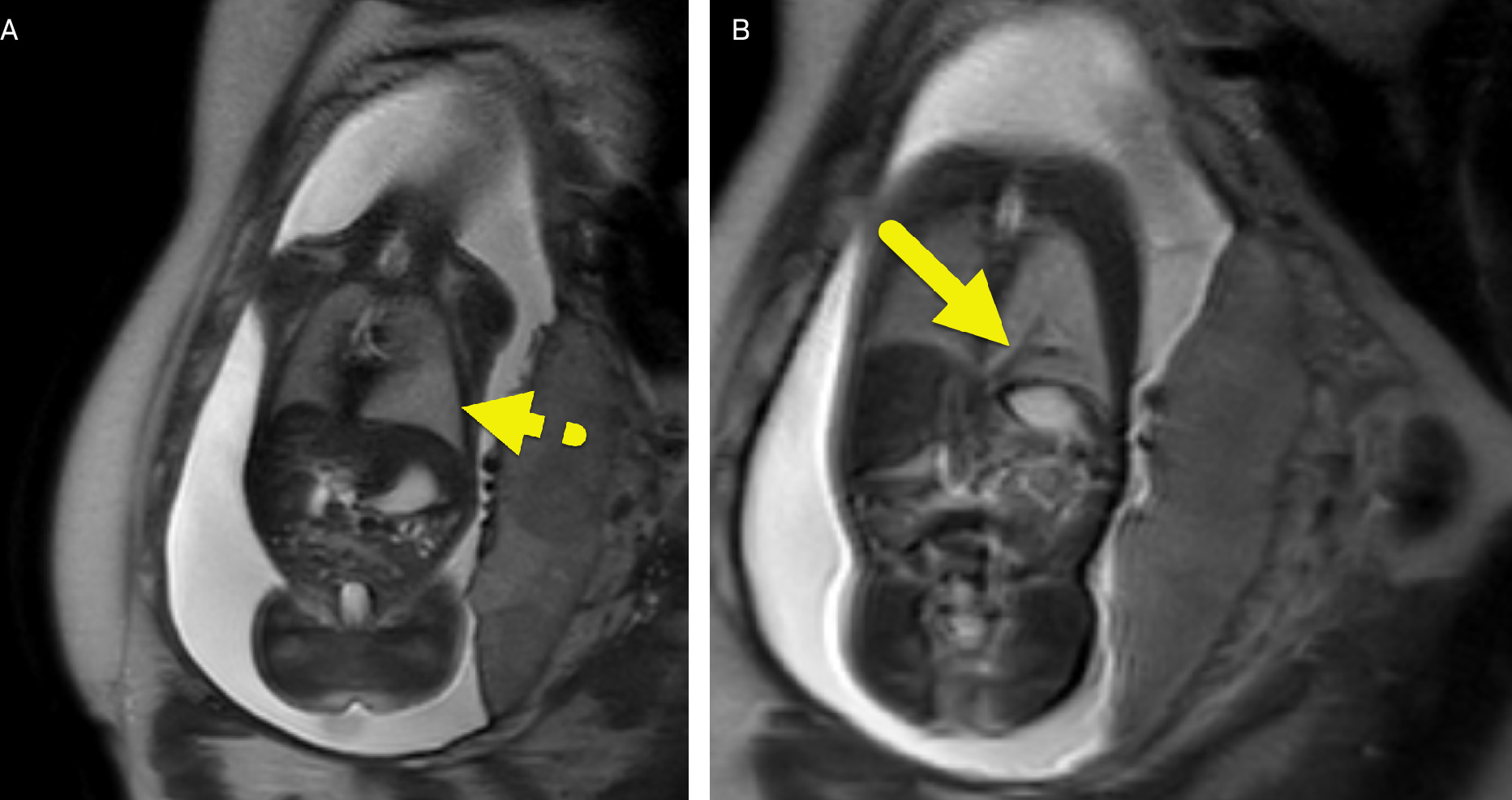
Imaging Findings
Fetal MRI (Figure 1) showed a T2-hyperintense mass-like region of the left lower lung supplied by a vessel arising from the aorta. After birth, a contrast-enhanced CT (Figure 2) was performed, showing an enhancing soft-tissue mass in the left lower lung. A large artery was visible arising from the aorta and supplying the mass. Venous drainage extended from the mass and joined with the main portal vein.

Diagnosis
Bronchopulmonary sequestration (BPS).
The differential diagnosis based on fetal imaging includes congenital pulmonary airway malformation, bronchogenic cysts, congenital lobar emphysema, and congenital diaphragmatic hernia. 1
Discussion
BPS exists as a spectrum of anomalies that are generally defined as nonfunctional lung tissue that does not communicate with the tracheobronchial tree and derives its arterial blood supply from the systemic vasculature. This condition represents roughly 0.15-6.4% of all congenital pulmonary malformations and is classified as either intralobar or extralobar.
Intralobar sequestrations (ILS) are more common and account for 75% of all BPS. 2,3 In this type of sequestration, the sequestration is located within the lung, sharing the visceral pleura with normal lung. The arterial supply is from anomalous systemic arteries often from the descending aorta (72%). However, other arterial supply from the abdominal aorta, celiac axis, splenic artery, or intercostals has been reported. 4 Venous drainage of an ILS occurs via the ipsilateral inferior pulmonary vein (95%). Patients with ILS present later in life and often have symptoms of recurrent infections in the same portion of the lung. 5
Of all sequestrations, the extralobar type occurs in 15-25% and usually presents in infants <6 months of age. Extralobar sequestration (ELS) is more common in males (4:1), left-sided (65%), and associated with numerous congenital anomalies (65%). These associations include diaphragmatic hernia, cystic adenomatoid malformation, bronchogenic cysts, pectus excavatum, pericardial cysts, and enteric duplications 6 that are differentiated from an ILS by the presence of a separate pleural covering separating the sequestered lung from the adjacent normal lung. 3 Arterial supply is often from the thoracic aorta (46%). 6 However, blood supply may be from the abdominal aorta, pulmonary artery, intercostal artery, left gastric, and subclavian artery. Anomalous venous drainage pathway is usually systemic, flowing to the right atrium. The most common venous drainage is into the azygos vein, hemiazygos vein, or inferior vena cava. However, in a minority of cases, drainage can go into the portal vein or pulmonary vein. While all ILS are intrathoracic, ELS can be intrathoracic or extrathoracic. Extrathoracic sequestrations are less common and account for only 10% of ELS. Patients with ELS may first present on prenatal imaging with a visible mass. After birth, symptoms depend on the size of the sequestration, mass effect, and associated anomalies. 5
Chest radiography can show a focal airspace opacity, a focal lucent lesion, or both. In larger lesions, prominent features such as a mediastinal shift or abnormal lung development could be seen. 7 CT is the main imaging modality used to assess congenital lung lesions because of its ability to accurately depict the lung parenchyma and the abnormal systemic arterial supply. 8
Surgical resection has been the gold standard for therapy. In the late 1990s, video-assisted thoracoscopy (VATS) and catheter embolization were introduced as minimally invasive alternatives. 9 A lobectomy is preferred for most BPS, while a wedge resection is favored for smaller lesions situated away from the pulmonary hilum. Resections can either be performed through an open thoracotomy or VATS, with VATS being more widely accepted due to the lesser degree of invasiveness. In infants, endovascular occlusion of the supplying arteries can be performed as a presurgical option or as primary therapy to decrease or eliminate blood flow to the sequestered tissue. 5,10 The outcome for children with sequestration is generally very good but may depend on associated anomalies.
Conclusion
BPS is a rare congenital lung malformation characterized by its systemic arterial supply and lack of connection to the bronchial tree. There are 2 types of sequestration: intralobar and extralobar. ILS are more common. Patients with this type of BPS typically present with recurrent pulmonary infection. Chest radiography is usually the initial imaging examination, followed by CT. CT is used to diagnose the aberrant venous and arterial anatomy and eliminate other disease entities. Treatment is surgical.
References
- Ko S, Ng S, Lee T. Noninvasive imaging of bronchopulmonary sequestration. AJR Am J Roentgenol. 2000;175(4):1005-1012. doi:10.2214/ajr.175.4.1751005.
- Ou J, Lei X, Fu Z. Pulmonary sequestration in children: a clinical analysis of 48 cases. Int J Clin Exp Med. 2014;7(5):1355-1365.
- Abbey P, Das C, Pangtey G. Imaging in bronchopulmonary sequestration. J Med Imaging Radiat Oncol. 2009;53(1):22-31. doi:10.1111/j.1754-9485.2009.02033.x.
- Prasad R, Garg R, Verma S. Intralobar sequestration of lung. Lung India. 2009;26(4):159-161. doi:10.4103/0970-2113.56357.
- Zobel M, Gologorsky R, Lee H, Vu L. Congenital lung lesions. Semin Pediatr Surg. 2019;28(4):150821. doi:10.1053/j.sempedsurg.2019.07.004.
- Brown E, Marr C, Farmer D. Extralobar pulmonary sequestration: the importance of intraoperative vigilance. J Pediatr Surg Case Rep. 2013;1(4):74-76. doi:10.1016/j.epsc.2013.02.015.
- Menashe S, Iyer R, Parisi M, Otto R, Stanescu A. Pediatric chest radiographs: common and less common errors. AJR Am J Roentgenol. 2016;207(4):903-911. doi:10.2214/AJR.16.16449.
- Gabelloni M, Faggioni L, Accogli S, Aringhieri G, Neri E. Pulmonary sequestration: what the radiologist should know. Clin Imaging. 2021;73:61-72. doi:10.1016/j.clinimag.2020.11.040.
- Roman S, Millet C, Mekheal N, Mekheal E, Manickam R. Endovascular embolization of pulmonary sequestration presenting with hemoptysis: a promising alternative to surgery. Cureus. 2021;13(8). doi:10.7759/cureus.17399.
- Zhang N, Zeng Q, Chen C, Yu J, Zhang X. Distribution, diagnosis, and treatment of pulmonary sequestration: report of 208 cases. J Pediatr Surg. 2019;54(7):1286-1292. doi:10.1016/j.jpedsurg.2018.08.054.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Bronchopulmonary Sequestration in a Fetus. Applied Radiology. 2025. doi:10.37549/JPCR-25-0047.