Button Battery Ingestion
Journal of Pediatric Case Reports — Vol. 1 , Issue 3
Published: April 1, 2026
1 University of Arizona College of Medicine- Phoenix, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Button battery ingestion is an increasingly common cause of pediatric emergency department visits. Diagnosis is primarily made through radiographic evaluation, with anterior-posterior and lateral views distinguishing button batteries from other radiopaque foreign bodies. While most patients recover without complications, the caustic nature of modern lithium batteries necessitates careful evaluation and close follow-up to prevent potentially fatal outcomes. High-risk cases include children under 6 years of age, ingestion of batteries 20 mm or larger, and esophageal impaction, all of which require urgent intervention and monitoring.
Keywords
gastrointestinal, eophagus, trauma, ingestion
Categories
Case Summary
A toddler presented with 1 day of non-bilious vomiting. She was initially diagnosed with a viral illness, but her symptoms progressed to include persistent emesis, fever, and decreased oral intake. Due to these ongoing concerns, she was brought to the emergency department where a chest radiograph was obtained.
Imaging Findings
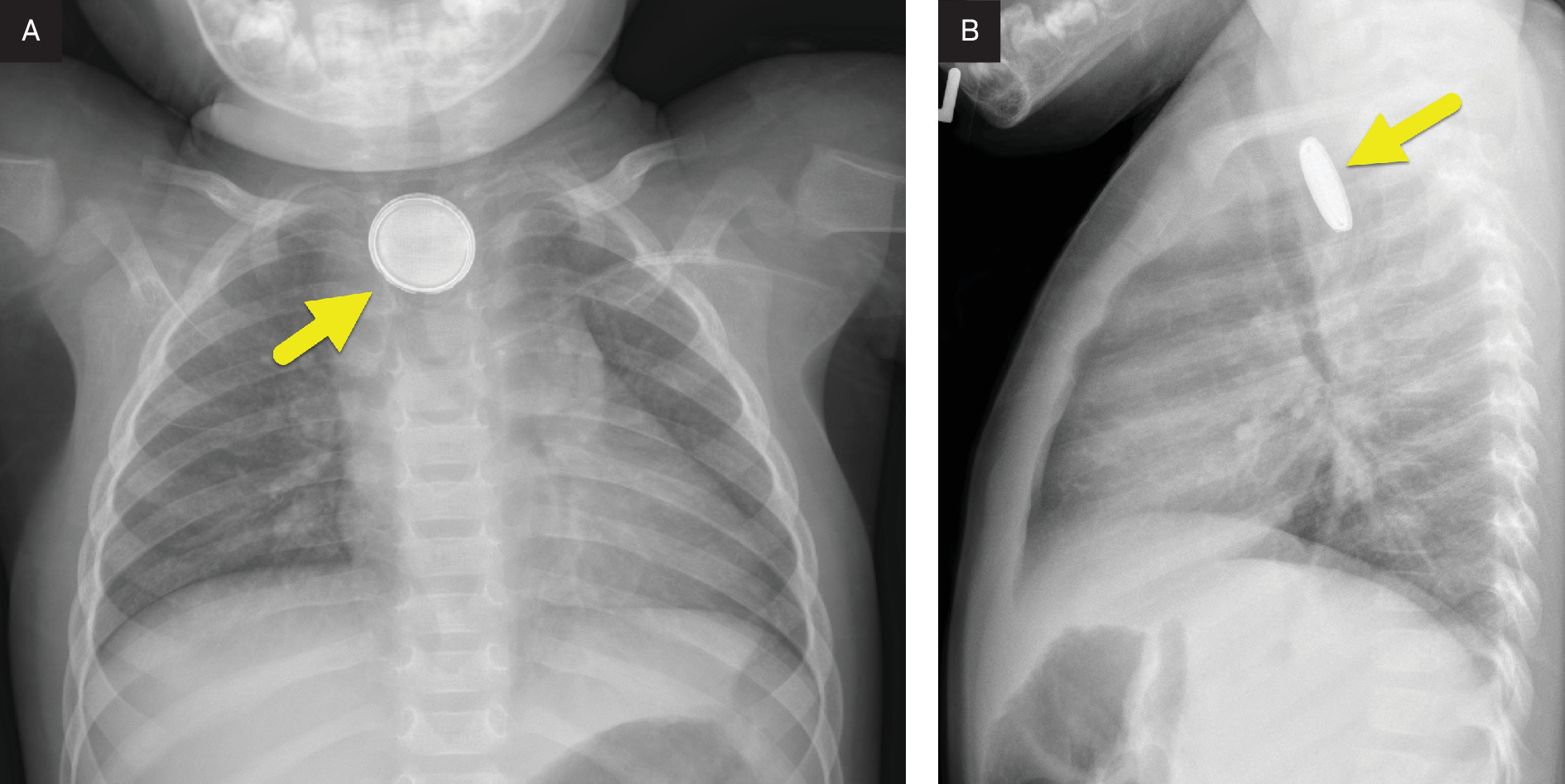
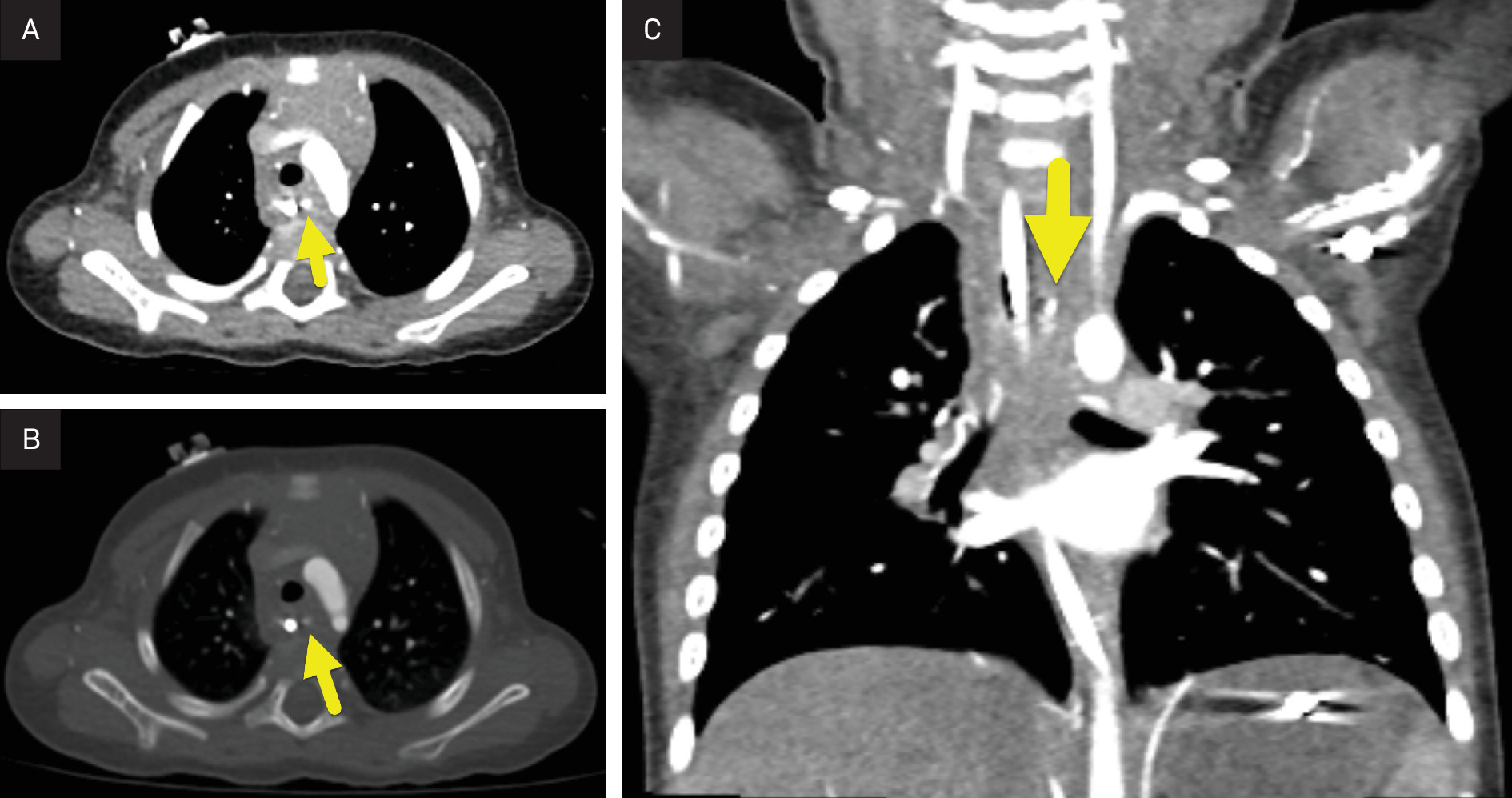
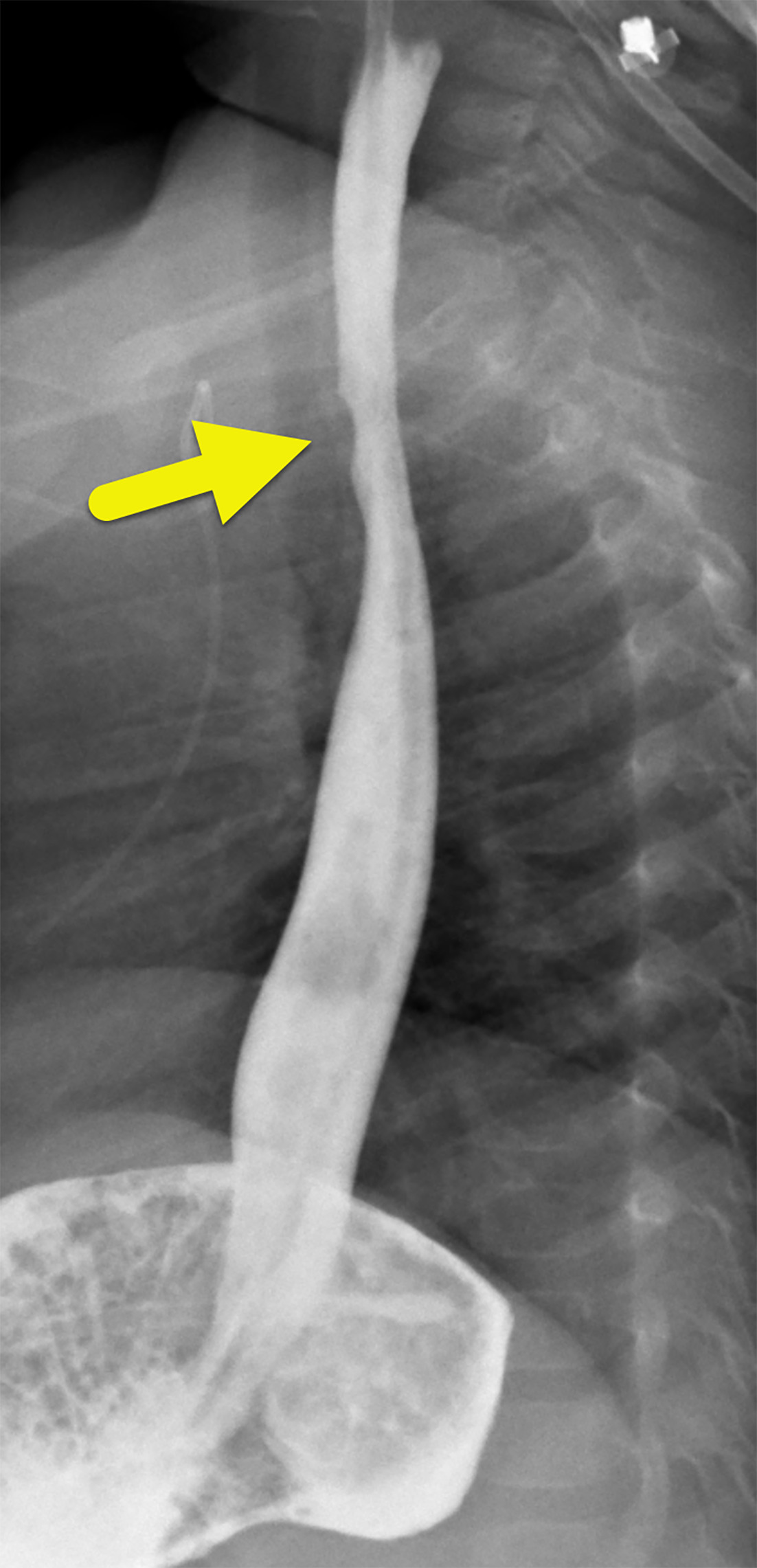
Chest radiograph (Figure 1) demonstrated a button battery lodged within the proximal esophagus at the level of the aortic arch. Following endoscopic removal, a chest CT (Figure 2) revealed residual battery fragments but no vascular injury. An esophagram (Figure 3) performed 2 weeks later showed mild irregularity of the proximal esophagus at the site of impaction.
Diagnosis
Button battery ingestion.
The imaging differential diagnosis includes button battery ingestion, coin ingestion, and magnet ingestion.
Discussion
Button battery ingestion is a medical emergency due to its potential for severe and life-threatening complications. When lodged in the esophagus, button batteries can generate a localized electrical current, leading to mucosal injury, liquefactive necrosis, and perforation within hours. Additionally, leakage of alkaline or lithium-containing substances can cause further tissue damage, increasing the risk of fistula formation, mediastinitis, and even fatal vascular injury. Given these serious consequences, rapid identification and removal are critical to prevent irreversible injury.
The prevalence of button battery ingestions has increased significantly in recent decades. In 1995, only 0.14% of emergency department visits for foreign body ingestions in children under 6 years old were attributed to batteries.1 By 2015, this number had risen to 8.4%, with 85.9% of identified batteries being button batteries.1 Two key factors have contributed to this trend: the larger diameters of modern button batteries, which increase the risk of esophageal impaction, and the conversion to lithium cells, which are more caustic to human tissues.2
In cases of witnessed button battery ingestion, patients often present with acute gastrointestinal symptoms, including vomiting, dysphagia, and abdominal pain, or with respiratory symptoms such as cough, stridor, or shortness of breath. In unwitnessed ingestions, symptoms may appear later, often manifesting as gastrointestinal hemorrhage or constitutional symptoms such as fever or weight loss.3
Given the severity of button battery ingestion, identifying patients at highest risk for complications is critical. The most vulnerable populations include children under 6 years of age and those who ingest lithium batteries larger than 20 mm in diameter.2,4 Once a battery becomes lodged, it can rapidly induce tissue damage, with the gastrointestinal tract being the most affected system. Complications range from ulceration (22.1%) and perforation (18.1%) to more severe injuries such as tracheoesophageal fistulas (14.6%), strictures or obstruction (13.7%), and tissue necrosis (4.9%)—the majority of which involve the esophagus. In the most severe cases, vascular involvement occurs in 6% of complications, as the battery erodes through the gastrointestinal wall into adjacent arteries or veins. This can result in catastrophic hemorrhage due to rapid vascular extravasation and exsanguination, making it one of the most feared and fatal consequences of button battery ingestion.4
Given the potential for life-threatening complications, rapid and accurate diagnosis of button battery ingestion is essential. The initial imaging evaluation includes anterior-posterior and lateral chest radiographs.3 On frontal radiographs, button batteries exhibit a “halo” or “double rim” sign, where the larger cathode portion forms the outer ring, and the radiopaque central circle represents both the cathode and anode. On lateral radiographs, this translates to a “step-off” sign, where the anode protrudes slightly from the cathode, producing a characteristic step-like appearance.
The radiographic appearance of button batteries can sometimes be mimicked by other radiopaque objects, such as stacked coins. Batteries smaller than 20 mm may not display the halo sign due to variations in battery morphology, but the step-off sign remains a reliable indicator for identifying button batteries of all sizes. Therefore, when observed, the step-off sign should raise strong suspicion for button battery ingestion.5
Serial CT or MRI is used to assess the extent of soft tissue injury following button battery removal and to monitor resolution.3,6 Both modalities may demonstrate soft tissue edema at the site of impaction, which can take weeks to resolve. MRI may also reveal blooming artifact, resulting from a combination of hydroxide ions generated during the initial caustic injury and hemosiderin deposition.6 Additionally, CT may detect residual metallic fragments from the battery surface.
When interpreting radiologic studies, it is particularly important to evaluate tissue at the anode contact site, as this location carries the highest risk of injury, especially in the esophagus. This occurs because the negative pole of the battery generates hydroxide ions, leading to localized corrosive tissue damage.3,4,6 In cases of button battery ingestion with suspected hemorrhage, CTA is used to assess the adjacent aorta.7 Key imaging findings of aortic injury include periaortic edema, aortic wall thickening, and pseudoaneurysm formation.
Most patients with button battery ingestion have a favorable prognosis, with a low overall complication rate of 0.165 %.4 However, when complications do occur, they can be life-threatening, particularly in cases of esophageal impaction. Impacted batteries require urgent endoscopic removal to prevent progressive tissue damage and fatal hemorrhage.2,4
Conclusion
Button battery ingestion is an increasingly common cause of pediatric emergency department visits. Diagnosis is primarily made through radiographic evaluation, with anterior-posterior and lateral views distinguishing button batteries from other radiopaque foreign bodies.
While most patients recover without complications, the caustic nature of modern lithium batteries necessitates careful evaluation and close follow-up to prevent potentially fatal outcomes. High-risk cases include children under 6 years of age, ingestion of batteries 20 mm or larger, and esophageal impaction, all of which require urgent intervention and monitoring.
References
- Orsagh-Yentis D, McAdams R, Roberts K, McKenzie L. Foreign-body ingestions of young children treated in US emergency departments: 1995-2015. Pediatrics. 2019;143(5). doi:10.1542/peds.2018-1988.
- Kramer R, Lerner D, Lin T. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN endoscopy committee. J Pediatr Gastroenterol Nutr. 2015;60(4):562-574. doi:10.1097/MPG.0000000000000729.
- Mubarak A, Benninga M, Broekaert I. Diagnosis, management, and prevention of button battery ingestion in childhood: a European society for paediatric gastroenterology hepatology and nutrition position paper. J Pediatr Gastroenterol Nutr. 2021;73(1):129-136. doi:10.1097/MPG.0000000000003048.
- Varga &, Kovács T, Saxena A. Analysis of complications after button battery ingestion in children. Pediatr Emerg Care. 2018;34(6):443-446. doi:10.1097/PEC.0000000000001413.
- Meyer T, Grunz J, Taeger J. Systematic analysis of button batteries’, euro coins’, and disk magnets’ radiographic characteristics and the implications for the differential diagnosis of round radiopaque foreign bodies in the esophagus. Int J Pediatr Otorhinolaryngol. 2020;132:109917. doi:10.1016/j.ijporl.2020.109917.
- Grey N, Malone L, Miller A. Magnetic resonance imaging findings following button battery ingestion. Pediatr Radiol. 2021;51(10):1856-1866. doi:10.1007/s00247-021-05085-w.
- Demiroren K. Management of gastrointestinal foreign bodies with brief review of the guidelines. Pediatr Gastroenterol Hepatol Nutr. 2023;26(1):1-14. doi:10.5223/pghn.2023.26.1.1.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Button Battery Ingestion. Journal of Pediatric Case Reports. 2026;1(3). doi:10.37549/JPCR-26-0088.