1 College of Medicine, Wayne State University, Detroit, Michigan
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Cardiac chloromas are rare extramedullary tumors associated with acute myelogenous leukemia that can infiltrate cardiac tissues, disrupt normal function, and contribute to heart failure. Their diagnosis is challenging due to their rarity and variable clinical presentation. Imaging techniques such as echocardiography, MRI, CT, and PET/CT are necessary for detecting these masses and assessing their extent. Histopathologic analysis confirms the diagnosis by identifying leukemic markers within the tumor. Systemic chemotherapy remains the primary treatment, but prognosis remains poor due to the aggressive nature of acute myeloid leukemia and the complexity of managing cardiac involvement.
Categories
Case Summary
An infant presented with a 1-day history of lethargy, decreased oral intake, reduced urine output, respiratory distress, and diarrhea without emesis. There were no known contacts with individuals who were ill. An outpatient chest radiograph demonstrated cardiomegaly. Initial laboratory evaluation revealed normocytic anemia, thrombocytopenia, and leukocytosis with circulating blasts. The physical examination was notable for massive hepatosplenomegaly.
Image Findings
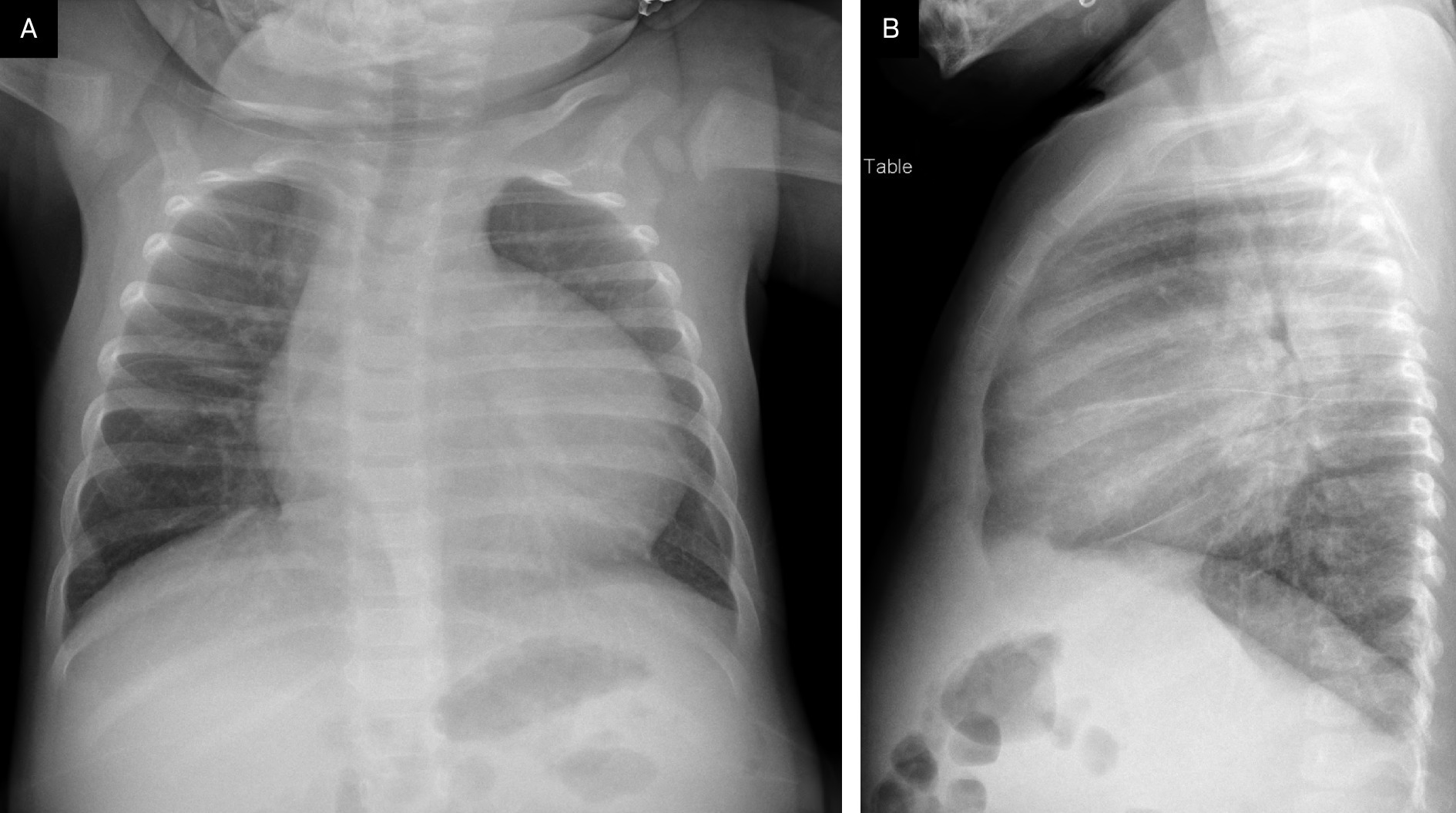
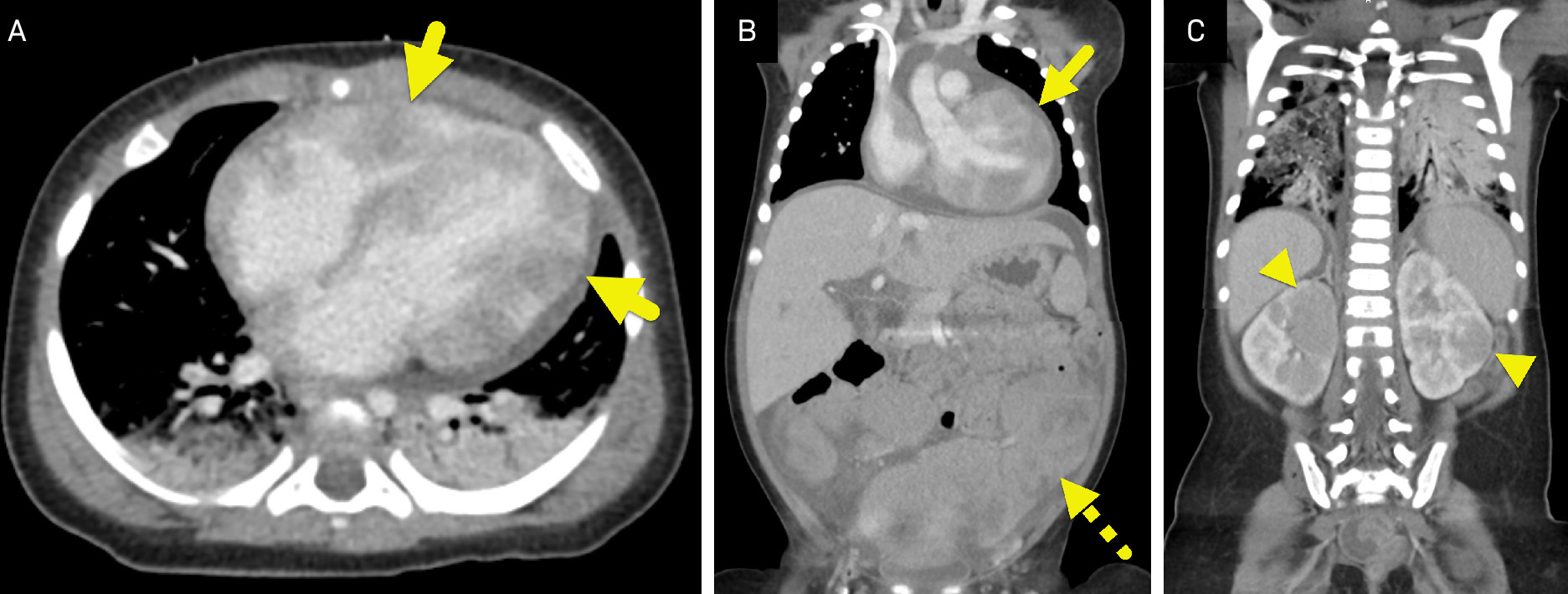
Initial chest radiograph (Figure 1) demonstrated marked cardiomegaly. Follow-up contrast-enhanced CT of the chest, abdomen, and pelvis (Figure 2), performed 2 days later, revealed multiple soft tissue masses consistent with chloromas involving the myocardium, mesentery, and kidneys.
Diagnosis
Acute myeloid leukemia (AML)-associated cardiac chloroma.
The differential diagnosis for a cardiac mass includes cardiac myxoma, cardiac sarcoma, and metastatic tumor to the heart.1
Discussion
Chloromas are rare extramedullary tumors composed of immature myeloid cells and are associated with AML. While chloromas can arise in various sites, including the soft tissues, lymph nodes, gastrointestinal and genitourinary systems, and central nervous system, cardiac involvement is particularly rare, occurring in only 2.5-9% of cases.2,3 Cardiac chloromas may involve the myocardium, pericardium, or endocardium, where they can disrupt normal cardiac function and contribute to heart failure.4
Chloromas develop when leukemic myeloid blasts migrate from the bone marrow to distant tissues, where they proliferate and form solid masses. While the exact mechanism remains unclear, several hypotheses have been proposed to explain myeloid blast migration. One theory suggests that leukemic cells adhere to endothelial surfaces, facilitating extravasation into surrounding tissues. Once outside the bone marrow, these cells may evade normal regulatory mechanisms, leading to uncontrolled proliferation in extramedullary sites.5
The clinical presentation of cardiac chloromas varies widely, with symptoms and severity depending on the tumor’s size, location within the heart, and extent of cardiac involvement. Smaller tumors may be asymptomatic or cause only mild palpitations, while larger tumors or those affecting the myocardium, pericardium, or endocardium can significantly impair cardiac function. Due to this variability, patients may present with a wide range of symptoms, including chest pain, dyspnea, palpitations, or more severe manifestations of heart failure.6
Imaging plays a crucial role in diagnosing cardiac chloromas. Echocardiography may reveal cardiomegaly or/and hypoechoic intracardiac masses, providing an initial assessment of cardiac involvement.7 Cardiac MRI offers detailed visualization of myocardial infiltration, typically demonstrating a hypointense or isointense mass on T1-weighted images and a hyperintense mass on T2-weighted images.6 The lesion typically enhances homogeneously following contrast administration. In addition to characterizing imaging features, cardiac MRI is also used to assess the tumor’s functional impact. CT and PET/CT are valuable for evaluating the extent of both cardiac and extracardiac involvement.6
Cardiac chloromas can present with nonspecific clinical and laboratory findings, making imaging and histopathologic evaluation critical for diagnosis. While an ECG may reveal arrhythmias or conduction abnormalities, and elevated cardiac biomarkers like troponins may suggest myocardial involvement, these findings lack specificity. Imaging techniques such as echocardiography, MRI, and CT are essential for identifying cardiac masses, but a biopsy remains the gold standard for definitive diagnosis through leukemic cell detection.8
Histopathologically, cardiac chloromas consist of immature myeloid cells demonstrating typical leukemic markers, including myeloperoxidase and CD45/34. Immunohistochemical staining is essential for confirming the diagnosis and distinguishing chloromas from other cardiac tumors, such as lymphomas or metastatic disease.4
The primary treatment for cardiac chloromas is systemic chemotherapy, which targets leukemic cells both in the heart and throughout the body. Standard regimens typically include cytarabine and anthracyclines, aimed at controlling the underlying AML.9 In some cases, localized radiation therapy may be considered to reduce tumor burden and alleviate symptoms.
Despite treatment, cardiac chloromas are associated with significant morbidity and mortality, largely due to complications such as heart failure and arrhythmias. The 5-year survival rate for affected patients is 31.9%, with higher survival rates observed in younger patients. However, prognosis remains poor, as these tumors represent a rare extramedullary manifestation of AML that is particularly challenging to manage, even with aggressive therapy.4
Conclusion
Cardiac chloromas are rare extramedullary tumors associated with AML that can infiltrate cardiac tissues, disrupt normal function, and contribute to heart failure. Their diagnosis is challenging due to their rarity and variable clinical presentation. Imaging techniques such as echocardiography, MRI, CT, and PET/CT are essential for detecting these masses and assessing their extent. Histopathologic analysis confirms the diagnosis by identifying leukemic markers within the tumor. Systemic chemotherapy remains the primary treatment, but prognosis remains poor due to the aggressive nature of AML and the complexity of managing cardiac involvement.
References
- Pino P, Moreo A, Lestuzzi C. Differential diagnosis of cardiac tumors: general consideration and echocardiographic approach. J Clin Ultrasound. 2022;50(8):1177-1193. doi:10.1002/jcu.23309.
- Singh A, Kumar P, Chandrashekhara S, Kumar A. Unravelling chloroma: review of imaging findings. Br J Radiol. 2017;90(1075):20160710. doi:10.1259/bjr.20160710.
- Zorn K, Cunningham A, Meyer A, Carlson K, Rao S. Pediatric myeloid sarcoma, more than just a chloroma: a review of clinical presentations, significance, and biology. Cancers. 2023;15(5):1443. doi:10.3390/cancers15051443.
- Mawad R, Wu D, Abkowitz J, Walter R. Myeloid sarcoma of the heart. Leuk Lymphoma. 2012;53(12):2511-2514. doi:10.3109/10428194.2012.685736.
- Stefanidakis M, Karjalainen K, Jaalouk D. Role of leukemia cell invadosome in extramedullary infiltration. Blood. 2009;114(14):3008-3017. doi:10.1182/blood-2008-04-148643.
- Bussani R, Castrichini M, Restivo L. Cardiac tumors: diagnosis, prognosis, and treatment. Curr Cardiol Rep. 2020;22(12):169. doi:10.1007/s11886-020-01420-z.
- Marcos-Alberca P, Ibáñez B, Rey M. Cardiac granulocytic sarcoma (chloroma): in vivo diagnosis with transesophageal echocardiography. J Am Soc Echocardiogr. 2004;17(9):1000-1002. doi:10.1016/j.echo.2004.04.030.
- Almond L, Charalampakis M, Ford S, Gourevitch D, Desai A. Myeloid sarcoma: presentation, diagnosis, and treatment. Clin Lymphoma Myeloma Leuk. 2017;17(5):263-267. doi:10.1016/j.clml.2017.02.027.
- Mignano J, Chan M, Rosenwald I, Kimmelstiel C, Wolfe L. Intracardiac chloroma. J Pediatr Hematol Oncol. 2009;31(12):977-979. doi:10.1097/MPH.0b013e3181b78951.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript, and no part of this article has been previously published elsewhere.
Citation
. Cardiac Chloroma. Applied Radiology. 2026. doi:10.37549/JPCR-25-0042.