Cerebral Palsy and Hip Dysplasia
Applied Radiology
Published: December 24, 2025
1 Virginia Tech Carilion School of Medicine, Roanoke, Virginia
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Cerebral palsy is the most common physical disability in children and can result in long-term musculoskeletal complications due to asymmetrical muscular forces across joints. One of the most significant orthopedic sequelae is hip dysplasia, which can severely impair mobility and quality of life for both patients and caregivers. Routine screening with anteroposterior pelvic radiographs should begin at age 2 in children with a Gross Motor Function Classification System level of II or higher, with additional surveillance guided by functional level and rate of progression.
Preventive strategies for hip displacement include physical therapy, antispasticity medications, and postural support. Surgical intervention is typically indicated when the migration percentage reaches 40-60%, with the best outcomes achieved when performed prior to complete dislocation.
Keywords
syndrome, complications, hip
Categories
Case Summary
A young child with a history of Niemann-Pick disease and spastic quadriplegic cerebral palsy presented for routine screening hip radiograph.
Imaging Findings
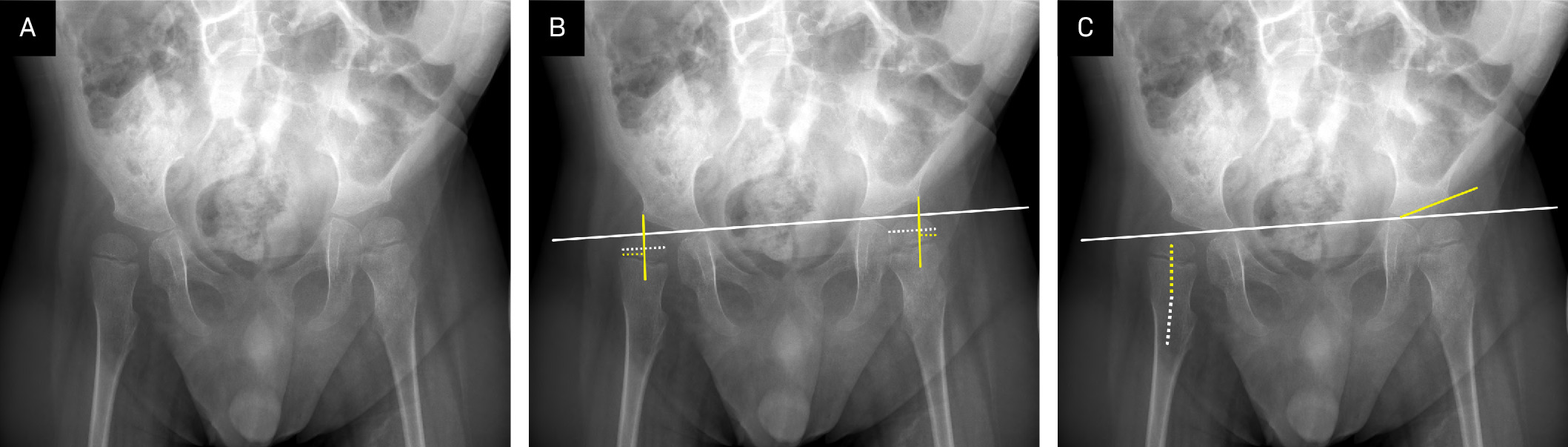
Anteroposterior pelvic radiographs (Figures 1, 2) obtained 2 years apart demonstrate progressive hip displacement. Both hips show a coxa valga configuration. Over time, the degree of lateral migration of the femoral heads increases, ultimately progressing to Frank dislocation of the right hip on the follow-up radiograph.

Diagnosis
Cerebral palsy with neuromuscular hip dislocation.
The differential diagnosis for pediatric neuromuscular hip dislocation includes other diseases that can cause spasticity in infants, including spina bifida or spinal cord injury, stroke, hereditary spastic paraplegias, or less commonly Charcot-Marie-Tooth disease.
Discussion
Cerebral palsy is the most common physical disability in children, affecting 1 in 323 live births. 1 Although the etiology is multifactorial and incompletely understood, many cases are linked to perinatal brain injury. Prematurity is among the strongest risk factors; infants born before 28 weeks’ gestation have a 50-fold increased risk compared with those born at term. Other prenatal risks include maternal systemic inflammation, multiple gestation, pre-eclampsia with fetal growth restriction, fetal thyroid dysfunction, and maternal factors such as obesity, alcohol exposure, and intrauterine infection. Perinatal stroke is an underlying cause in approximately 50% of patients with cerebral palsy cases. In these instances, stroke may be associated with congenital heart disease, meningitis, placental thrombosis, or hypertensive disorders of pregnancy. Additional risk factors include genetic predisposition and lower socioeconomic status. 2 Finally, in approximately 8% of cases, cerebral palsy is acquired postnatally, most often following traumatic brain injury or infection. 1
Cerebral palsy is diagnosed based on a combination of clinical and neurologic findings, with the defining feature being a permanent, nonprogressive disorder of motor function. 1 It is further classified into 4 clinical subtypes: spastic, dyskinetic, ataxic, and mixed. Functional severity is commonly evaluated using the Gross Motor Function Classification System (GMFCS), which categorizes motor abilities across 5 levels (Table 1). 1
| Level | Description |
|---|---|
| I | Walks without restrictions. May have limitations in advanced gross motor skills such as running, balance, coordination, or speed. |
| II | Walks without assistive devices. Some limitations in walking outdoors and in the community. May use handheld mobility devices for safety and climb stairs with a railing. May use wheeled mobility for long distances. |
| III | Walks with assistive mobility devices. May use handheld devices, manual or self-propelled wheelchairs, and powered mobility outside the home. |
| IV | Self-mobility with limitations. May walk short distances with physical assistance but primarily relies on wheeled mobility. Requires 1-2 people to assist with transfers. |
| V | Severely limited self-mobility. Limited ability to maintain antigravity head and trunk postures and control arm and leg movements. Uses a wheelchair in all settings. |
Although neuroimaging is not independently diagnostic, certain lesion patterns have been associated with the timing of injury and the severity or subtype of cerebral palsy. 2 Injuries sustained in the early third trimester or in preterm infants are more commonly associated with white matter injury. In contrast, injuries occurring later in the third trimester are more often linked to gray matter involvement. Lesions involving the thalamus and basal ganglia are frequently seen in patients with spastic quadriplegia. In a study by Rana et al, periventricular leukomalacia was present in 60% of patients with spastic diplegia, while cortical atrophy was observed more commonly in children with quadriplegic cerebral palsy. 4
Cerebral palsy can lead to secondary anatomic abnormalities due to chronic asymmetrical muscle forces across joints. One of the most significant of these is hip dysplasia, which affects approximately 15-35% of individuals with cerebral palsy. 5,6 Hip dysplasia in this population results from muscular imbalance: hypertonic hip adductors and flexors overpower relatively weak abductors and extensors, causing progressive lateral displacement of the femoral head. This displacement typically occurs in a posterosuperior direction due to spasticity of the adductor and iliopsoas muscles, leading to subluxation and, if left untreated, eventual dislocation. 3
Early detection and intervention are essential to prevent irreversible joint damage. Untreated hip displacement can lead to chronic pain, reduced mobility, degenerative joint changes, pressure ulcers, and significant challenges with perineal hygiene—all of which contribute to a decreased quality of life for patients and caregivers. 5,6
Routine screening is essential for the prevention of hip dysplasia in children with cerebral palsy as most patients remain asymptomatic until dislocation occurs. Anteroposterior pelvic radiographs are recommended beginning at 2 years of age for children with a GMFCS level of II or higher. 7 Follow-up imaging is performed every 6-12 months, depending on the GMFCS level and the rate of progression. Surveillance continues until age 10 for children with GMFCS level II and through skeletal maturity for those with GMFCS level III or higher. If imaging is needed in infants younger than 6 months based on signs, symptoms, and/or physical examination, US is the preferred modality as it allows dynamic assessment of hip stability. 7,8
Anteroposterior pelvic radiographs allow for key measurements used to assess hip development and detect early signs of dysplasia. Many of these measurements rely on specific reference lines drawn on the radiograph. The Hilgenreiner line is a horizontal line connecting the triradiate cartilage of each hip. The Perkin line is drawn perpendicular to the Hilgenreiner line, starting at the lateral acetabular margin. Hip displacement is quantified using the proximal femoral migration percentage, which represents the proportion of the proximal femoral epiphysis located lateral to the Perkin line, expressed as a percentage of the total epiphyseal width. 6 Acetabular dysplasia is assessed using the acetabular index, defined as the angle between the Hilgenreiner line and a line drawn from the lateral edge of the triradiate cartilage to the lateral margin of the acetabulum. Coxa valga is evaluated using the neck-shaft angle, which should be measured with the femur positioned in 30-40° of internal rotation. A neck-shaft angle >150° is considered elevated in newborns. 7,9 Details on how to perform these measurements are provided in Figure 1.
In addition to routine physical therapy, early intervention can help prevent the progression of hip dysplasia. Management strategies vary depending on the severity and may be either conservative or surgical. Spasticity can be addressed with targeted botulinum toxin injections or systemic medications such as baclofen or diazepam. 10 In select cases, selective dorsal rhizotomy—a neurosurgical procedure involving sectioning of specific sensory nerve rootlets—may be considered to reduce spasticity. 11 Surgical treatment for hip subluxation is typically considered when the proximal femoral migration percentage reaches between 40% and 60%. The decision to operate is also influenced by the rate of progression, with more rapid migration necessitating earlier and more aggressive intervention. 5 The procedures that may be performed include muscle/tendon lengthening, femoral osteotomies such as a varus derotational osteotomy and pelvic osteotomies. The best outcomes are achieved before the hip is dislocated.
Conclusion
Cerebral palsy is the most common physical disability in children and can result in long-term musculoskeletal complications due to the asymmetrical muscular forces across joints. One of the most significant orthopedic sequelae is hip dysplasia, which can severely impair mobility and quality of life for both patients and caregivers. Routine screening with anteroposterior pelvic radiographs should begin at age 2 in children with a GMFCS level of II or higher, with additional surveillance guided by functional level and rate of progression.
Preventive strategies for hip displacement include physical therapy, antispasticity medications, and postural support. Surgical intervention is typically indicated when the migration percentage reaches 40-60%, with the best outcomes achieved when performed prior to complete dislocation.
References
- Vitrikas K, Dalton H, Breish D. Cerebral palsy: an overview. Am Fam Physician. 2020;101(4):213-220.
- Korzeniewski S, Slaughter J, Lenski M, Haak P, Paneth N. The complex aetiology of cerebral palsy. Nat Rev Neurol. 2018;14(9):528-543. doi:10.1038/s41582-018-0043-6.
- Palisano R, Rosenbaum P, Walter S. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214-223. doi:10.1111/j.1469-8749.1997.tb07414.x.
- Rana K, Narwal V, Chauhan L. Structural and perfusion abnormalities of brain on MRI and technetium-99m-ECD SPECT in children with cerebral palsy: a comparative study. J Child Neurol. 2016;31(5):589-592. doi:10.1177/0883073815604224.
- Milks K, Whitaker A, Ruess L. Radiographic hip screening for children with cerebral palsy: an imaging and reporting update. Pediatr Radiol. 2022;52(1):12-21. doi:10.1007/s00247-021-05197-3.
- Okuno K, Kitai Y, Shibata T, Arai H. Risk factors for hip dislocation in dyskinetic cerebral palsy. J Orthop Surg. 2021;29(1):23094990211001196. doi:10.1177/23094990211001196.
- O’Donnell M, Mayson T, Miller S. Hip surveillance care pathway American Academy for Cerebral Palsy and Developmental Medicine (AACPDM).
- Aroojis A, Mantri N, Johari A. Hip displacement in cerebral palsy: the role of surveillance. Indian J Orthop. 2020;55(1):5-19. doi:10.1007/s43465-020-00162-y.
- Schroeder K, Heydemann J, Beauvais D. Musculoskeletal imaging in cerebral palsy. Phys Med Rehabil Clin N Am. 2020;31(1):39-56. doi:10.1016/j.pmr.2019.09.001.
- Pérez-de la Cruz S. Childhood cerebral palsy and the use of positioning systems to control body posture: current practices. Parálisis cerebral infantil y el uso de sistemas de posicionamiento para el control postural: estado actual del arte. Neurologia. 2017;32(9):610-615. doi:10.1016/j.nrl.2015.05.008.
- Munger M, Aldahondo N, Krach L, Novacheck T, Schwartz M. Long-term outcomes after selective dorsal rhizotomy: a retrospective matched cohort study. Dev Med Child Neurol. 2017;59(11):1196-1203. doi:10.1111/dmcn.13500.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Cerebral Palsy and Hip Dysplasia. Applied Radiology. 2025. doi:10.37549/JPCR-25-0038.