1 University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, North Carolina
2 Department of Radiology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina
3 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
4 Department of Radiology, Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Congenital chylothorax should be considered in neonates with symptoms and imaging consistent with pleural effusion, but analysis of the pleural effusion is necessary to confirm chylothorax. Lymphangiogram can identify a leak or highlight a structural lymphatic anomaly and is useful in guiding therapy. However, this case adds to the recent evidence in the literature that lymphangiography alone can resolve a lymphatic leak. Further research should be done on the efficacy of therapeutic lymphangiography to further elucidate its role in congenital chylothorax management.
Keywords
lymphatic, congenital
Categories
Case Summary
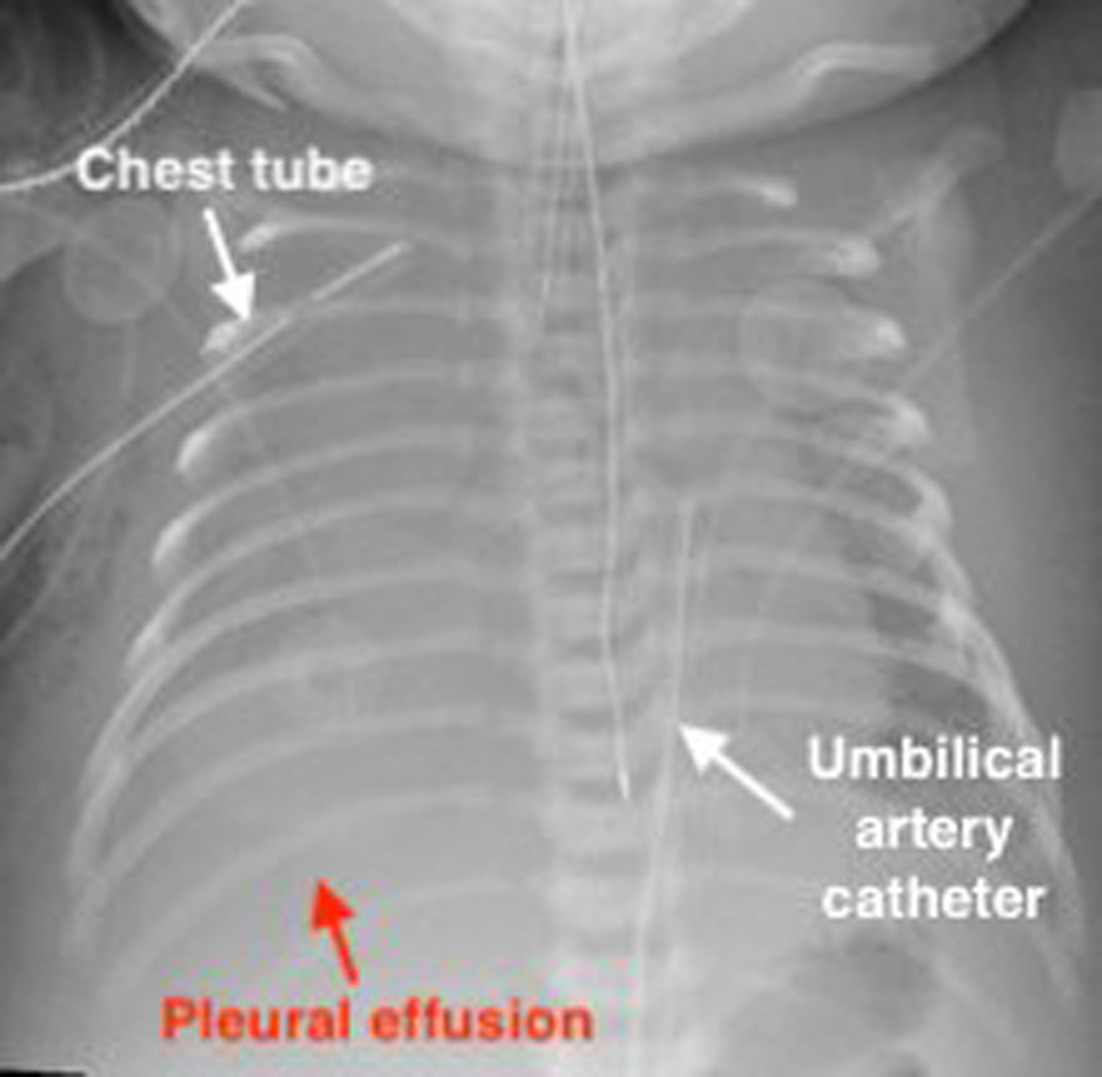
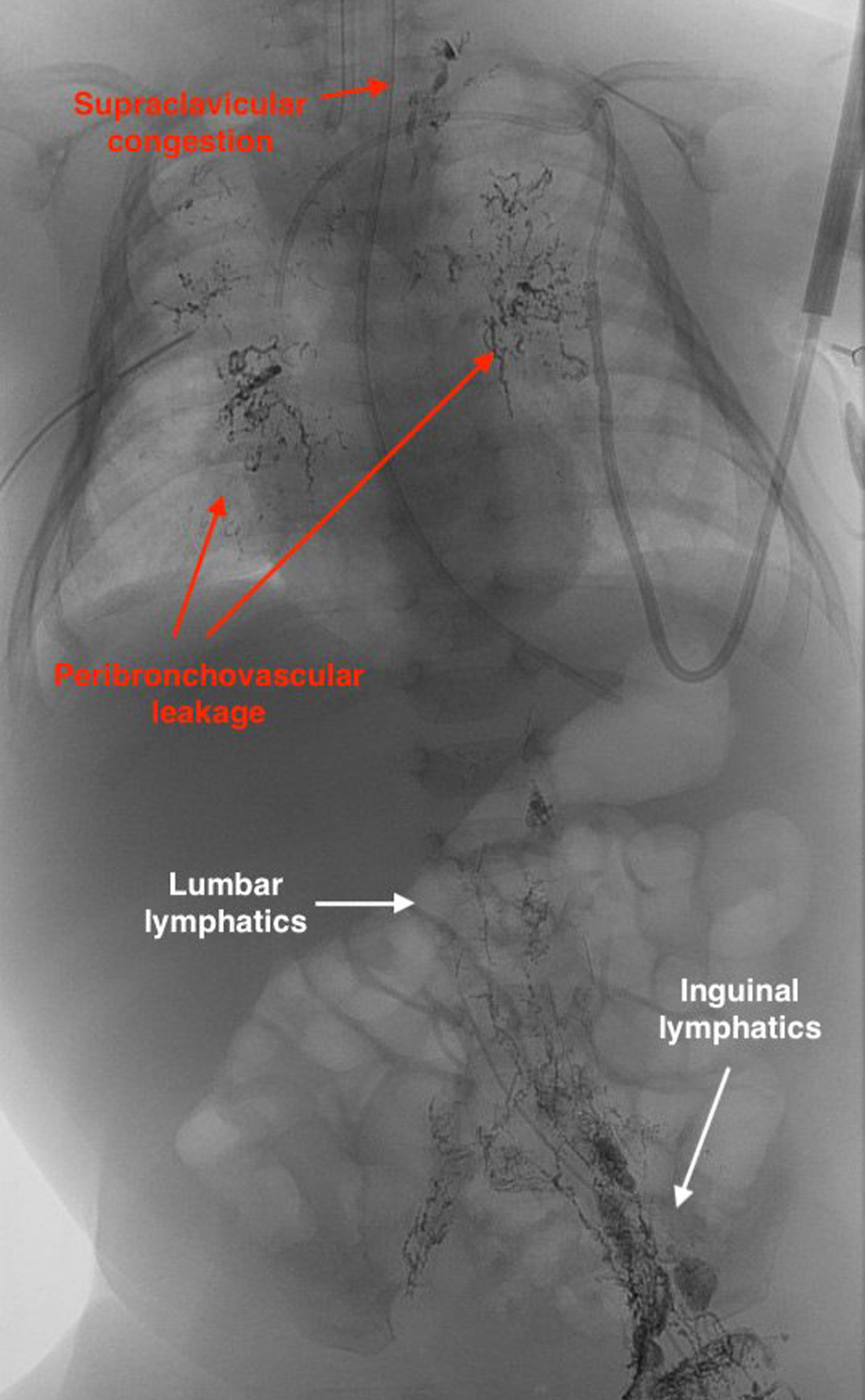
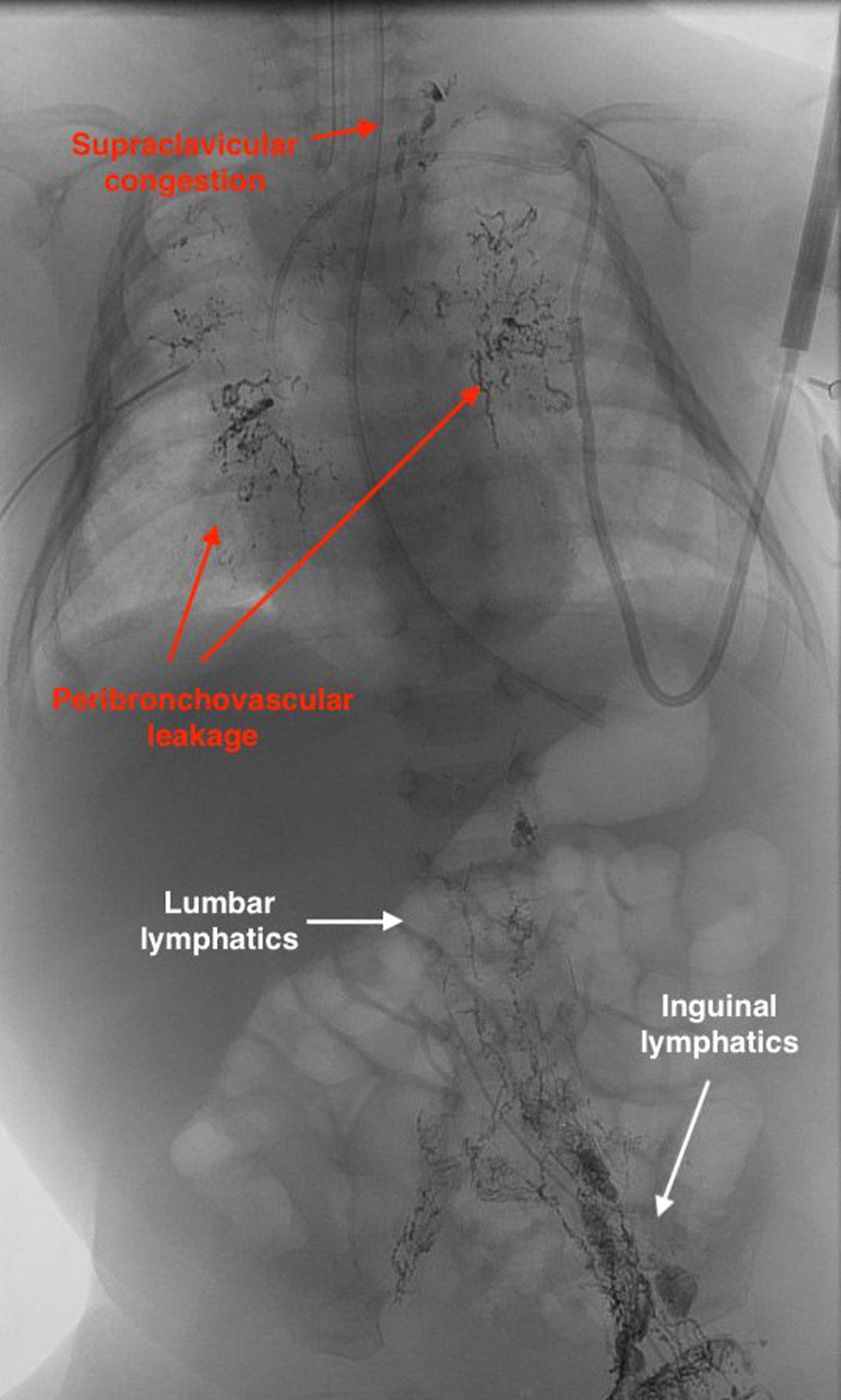
An infant with horseshoe kidney and hydrops fetalis was born at 37 weeks’ gestation and required intubation and chest compressions at birth. Chest x-ray confirmed the presence of a pleural effusion. A right chest tube was placed and drained a chylous effusion with a triglyceride level of 165 mg/dL and a lymphocyte count of 88%. Total parenteral nutrition therapy was initiated, and chest tube output increased with each feeding. Sirolimus therapy failed to improve the effusion. At 44 days of age, intranodal lymphangiography was performed with an access in the left inguinal lymph node using 0.9 mL oily contrast (Lipiodol, Guerbet, Princeton, New Jersey) and revealed contrast leaking into the bilateral peribronchovascular lymphatic channels consistent with a lymphatic channel anomaly. Following lymphangiography, serial chest x-rays did not demonstrate reaccumulation of pleural effusion. The patient’s chest tube was removed 4 days later, and the infant was weaned off diuretic medication. Genetic testing was performed, but no genetic mutations associated with congenital chylothorax were identified.
Imaging Findings
Chest x-ray performed at 41 days old revealed opacities primarily in the right lung, consistent with right-sided pleural effusion (Figure 1). Intranodal lymphangiography done at 44 days of age revealed normal iliac and lumbar lymphatics, cisterna chyli, and thoracic duct. Congestion was found at the left supraclavicular lymphatic channel with no contrast passage into the subclavian vein as well as reflux of contrast into the peribronchovascular lymphatics bilaterally. These findings are consistent with a central conducting lymphatic anomaly (CCLA) and chylothorax due to leakage of chyle into the pleural spaces (Figure 2). Chest x-ray performed 60 days after lymphangiography revealed normal pleural spaces and resolution of chylothorax (Figure 3).
Diagnosis
Chylothorax caused by CCLA.
Discussion
Chylothorax is a collection of lymphatic fluid in the pleural spaces and is the most common cause of congenital pleural effusion in neonates. Congenital chylothorax may present with lung hypoplasia and pulmonary hypertension, complicating cardiorespiratory function as well as the development of hydrops fetalis. Malnutrition and immune compromise can also manifest because of protein and cell leakage into the pleural space. 1,2 Postnatal development may be more insidious, with gradual worsening of dyspnea, cough, and chest discomfort. 2 Spontaneous regression of congenital chylothorax has been reported in 22% of cases, while severe conditions associated with hydrops may lead to high morbidity and mortality. 1 Prenatally, US can diagnose pleural effusion while chest imaging is used postnatally. 1,2 Thoracentesis or chest tube placement can extract the pleural fluid for analysis and identification of the effusion. Chylous effusion is milky white, and fluid analysis reveals triglyceride levels > 110 mg/dL, a pleural fluid to serum cholesterol ratio of <1.0, and evidence of chylomicrons. 2
Chylothorax can be caused by traumatic or iatrogenic injury of the thoracic duct, be a complication of malignancies such as lymphoma, and be associated with genetic syndromes and other congenital causes. 2 CCLA is defined by abnormalities in the thoracic duct that impede lymphatic flow into the subclavian vein, resulting in retrograde reflux and leakage of lymphatic fluid into the pleural space. 3 The causes of CCLA are poorly understood, though some genetic conditions like the RASopathies have been associated with congenital chylothorax. 2,4 Genetic syndromes are suspected when multiple embryological defects exist such as in this case of horseshoe kidney and CCLA, but no characteristic genetic mutations were identified in this patient.
Treatment of chylothorax often relies on conservative management. Octreotide reduces lymphatic flow via vasoconstriction and reduced fat absorption and has been shown to be effective in 47% of cases. 1,5 Nutritional management consists of a fat-free diet with medium-chain triglyceride supplementation (MCT) because long-chain triglycerides (LCTs) are absorbed into the lymphatic system while MCTs get directly absorbed into the systemic circulation. Increasing the ratio of MCT to LCT therefore reduces the amount of lymph available for leakage into the pleural space and gives time for the leak to spontaneously close. 1,2 Sirolimus has also been shown to be effective in treating various lymphatic malformations and one case of CCLA specifically, though its role in chylothorax management is not clearly defined. 6,7 Cases refractory to these interventions may require surgery or lymphatic interventions such as thoracic duct embolization. 8 In this patient, chylothorax returned when LCTs were reintroduced and sirolimus was not shown to mitigate the effusion.
Lymphangiography is commonly performed to visualize the lymphatic system to determine the etiology of the effusion and guide treatment. A contrast agent, such as Lipiodol, is injected into an inguinal lymph node and imaged via fluoroscopy, tracking the passage of Lipiodol through the thoracic duct and into the left subclavian vein. 8 While lymphangiography is most often done for visualization prior to a therapeutic procedure, several cases of resolution of chylothorax after lymphangiography alone have been reported. 9 Similarly, lymphangiography alone has been found to resolve other lymphatic leaks such as chylous ascites, where, similarly to chylothorax, lymphatic fluid leaks into the abdominal cavity. 10
In congenital chylothorax specifically, one case report describes resolution of congenital chylothorax after lymphangiography in 2 cases of RASopathies in an 8-year-old with cardiofaciocutaneous syndrome and a 2-month-old patient with Noonan syndrome. 4 The case presented here represents additional evidence of lymphangiography resolving congenital chylothorax and supports therapeutic lymphangiography as a potential treatment modality for medically refractory congenital chylothorax.
Conclusion
Congenital chylothorax should be considered in neonates with symptoms and imaging consistent with pleural effusion, but analysis of the pleural effusion is necessary to confirm chylothorax. Lymphangiogram can identify a leak or highlight a structural lymphatic anomaly and is useful in guiding therapy. However, this case adds to the recent evidence in the literature that lymphangiography alone can resolve a lymphatic leak. Further research should be done on the efficacy of therapeutic lymphangiography to further elucidate its role in congenital chylothorax management.
References
- De Angelis L, Bellini T, Witte M. Congenital chylothorax: current evidence-based prenatal and post-natal diagnosis and management. Lymphology. 2019;52(3):108-125.
- Tutor J. Chylothorax in infants and children. Pediatrics. 2014;133(4):722-733. doi:10.1542/peds.2013-2072.
- Trenor C, Chaudry G. Complex lymphatic anomalies. Semin Pediatr Surg. 2014;23(4):186-190. doi:10.1053/j.sempedsurg.2014.07.006.
- Kinota N, Kodama H, Moriyama T. Lymphangiography as a treatment for refractory congenital chylothorax due to RASopathies: a report of two cases. Interv Radiol (Higashimatsuyama). 2022;7(1):17-20. doi:10.22575/interventionalradiology.2021-0014.
- Bellini C, Cabano R, De Angelis L. Octreotide for congenital and acquired chylothorax in newborns: a systematic review. J Paediatr Child Health. 2018;54(8):840-847. doi:10.1111/jpc.13889.
- McCormick A, Rosenberg S, Trier K, Balest A. A case of a central conducting lymphatic anomaly responsive to sirolimus. Pediatrics. 2016;137(1). doi:10.1542/peds.2015-2694.
- Adams D, Trenor C, Hammill A. Efficacy and safety of sirolimus in the treatment of complicated vascular anomalies. Pediatrics. 2016;137(2). doi:10.1542/peds.2015-3257.
- Itkin M, Nadolski G. Modern techniques of lymphangiography and interventions: current status and future development. Cardiovasc Intervent Radiol. 2018;41(3):366-376. doi:10.1007/s00270-017-1863-2.
- Kim P, Tsauo J, Shin J. Lymphatic interventions for chylothorax: a systematic review and meta-analysis. J Vasc Interv Radiol. 2018;29(2):194-202. doi:10.1016/j.jvir.2017.10.006.
- Bhardwaj R, Vaziri H, Gautam A. Chylous ascites: a review of pathogenesis. Diagnosis and Treatment J Clin Transl Hepatol. 2018;6(1):105-113. doi:10.14218/JCTH.2017.00035.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Congenital Chylothorax. Applied Radiology. 2025. doi:10.37549/JPCR-25-0014.