Contained Abdominal Aortic Rupture
Applied Radiology
Published: April 1, 2026
1 Creighton University School of Medicine – Phoenix Regional Campus, Phoenix, Arizona
2 Phoenix Children’s Hospital, Phoenix, Arizona
Categories
Case Summary
A previously healthy child presented to the emergency department with suspected abdominal aortic injury from a lap belt after a head-on motor-vehicle collision. The physical exam showed an extensive lower-abdominal seatbelt sign with bilateral lower extremity abrasions and ecchymosis across the abdomen, as well as extreme swelling in the lower thoracic and upper lumbar area. The patient was hemodynamically stable and had a Glasgow Coma Scale score of 15 upon initial assessment.
Image Findings
Computed tomography (CT) of the abdomen and pelvis revealed abdominal aortic irregularity consistent with a contained aortic rupture, with intraluminal thrombus formation at the L2-L3 level and a retroperitoneal hematoma (Figure 1). Multiple fractures of the L2 vertebra, including a distraction fracture extending to the posterior elements, were also identified.
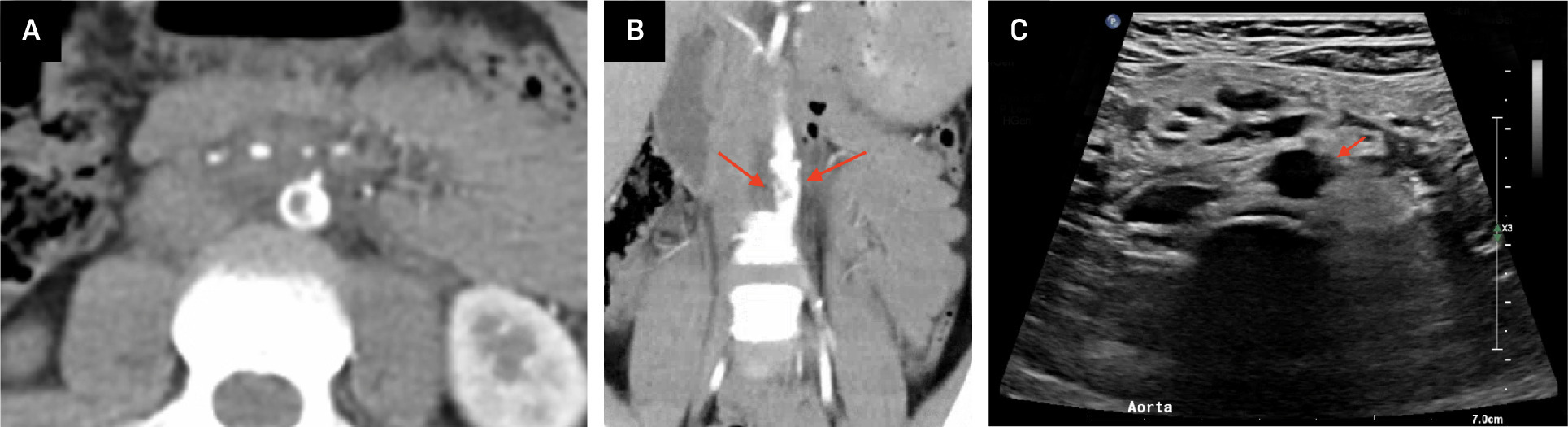
There was significant irregularity in the wall of the distal aorta above the bifurcation over a length of 2.4 cm, consistent with intimal injury. In addition to a 6 × 7 mm-sized filling defect in the aorta just above the aortic bifurcation, the aortic wall was thickened and accompanied by mild surrounding fat stranding. This aortic wall irregularity involved the origin of the inferior mesenteric artery, although the artery appeared patent. A dorsal hematoma at the level of the fracture contributed to increased stenosis at the L2 level.
Diagnosis
Contained abdominal aortic rupture at the L2 level, with associated L2 distraction fracture and a fracture through the left and right articular pillars on L2.
Discussion
Abdominal aortic injuries are very rare in the pediatric population; they typically occur in motor-vehicle crashes and result in significant morbidity and mortality.1,2 Owing to incorrect positioning of seat belts, their higher head-to-body ratio, and underdeveloped iliac crests, children are particularly susceptible to these often fatal injuries.3
Since aortic ruptures are rare in the pediatric population, treatment guidelines for them are not as well established for children as they are for adults. Owing to the diverse clinical presentation and correlated lesions, defining appropriate management for this population is challenging.3
The first successful management of aortic injury with an intravascular stent graft was performed in 2006.2 Intimal dissections that cause vascular symptoms and occlusion require additional investigation or intervention, whereas those without occlusion may be treated nonsurgically.4 In this case, endovascular stent graft placement was necessary to treat the primary aortic injury as well as to stabilize the aorta in preparation for subsequent spinal and bowel repair surgeries.
Endovascular stents are now the standard of care in the repair of posttraumatic vascular injuries.5 Candidates for arterial stent grafting consist of patients who are hemodynamically stable, have few associated injuries, and have high Glasgow coma scores.6 Endovascular stent grafting is also useful in minimizing contamination where there is a risk for bowel injury, as well as for when the patient’s aorta is expected to increase in diameter over time.4 The procedure also allows for repair of arterial vasculature located away from the injury, where nearby fractures and bleeding may hinder access.7
Long-term follow-up data for endovascular stent grafts in children is lacking, and this patient will likely require site stent graft dilation as the aorta increases in diameter.7 In addition, stent grafts are not designed for pediatric use, so extra consideration should be given to the size and profile of the stent to help prevent further injury and to excessive shortening following dilatation as the aorta increases in diameter.7,8
In this case of contained aortic rupture, observational management was considered but ultimately dismissed owing to the need for aortic stabilization prior to spinal fixation and for abdominal manipulation and prone positioning during surgery. Open repair was rendered suboptimal given the possibility of delayed bowel injury and increased lactate, making the risk of performing a fresh aortic graft placement too high. Ultimately, stent grafting was chosen to achieve stabilization and allow for the potential need for future stent dilation, without removing the option for future aorto-bifemoral or aorto-biiliac graft to manage demand ischemia.
After a multidisciplinary review and discussion, a 10 × 39 mm stent was placed (Figure 2), successfully treating the aortic irregularity, with no evidence of ongoing aortic leak. The patient subsequently underwent an L1-L2 spinal fusion with segmental instrumentation and an open reduction with evacuation of an epidural hematoma. The patient also underwent laparoscopic repair for various serosal injuries, including a right hemicolectomy. The aortic stent graft lessened the risk of further aortic injury throughout these operations. An arterial Doppler showed no evidence of arterial thrombus. At the 3-week follow-up, the patient clinically had returned to her preprocedural baseline without complaint. A follow-up CTA at 5 months demonstrated a stable stent graft within the abdominal aorta with no evidence of aneurysm, significant stenosis, or occlusion (Figure 3). There was occlusion of the origin of the inferior mesenteric artery, with arterial flow compensated for by collateral vessels.


Conclusion
Few cases of contained abdominal aortic ruptures in children have been reported, leaving gaps in criteria for determining the best approach to treatment of these injuries in this population. This report demonstrates a case of contained abdominal aortic rupture being successfully treated with an endovascular stent graft for immediate stabilization of the aorta and allowing for subsequent spinal and laparoscopic abdominal surgeries.
References
- Anderson S, Day M, Chen M. Traumatic aortic injuries in the pediatric population. J Pediatr Surg. 2008;43(6):1077-1081. doi:10.1016/j.jpedsurg.2008.02.030.
- Aidinian G, Karnaze M, Russo E, Mukherjee D. Endograft repair of traumatic aortic transection in a 10-year-old--a case report. Vasc Endovascular Surg. 2006;40(3):239-242. doi:10.1177/153857440604000310.
- Sadaghianloo N, Jean-Baptiste E, Breaud J. Blunt abdominal aortic trauma in paediatric patients. Injury. 2014;45(1):183-191. doi:10.1016/j.injury.2012.10.033.
- Takach T, Anstadt M, Moore H. Pediatric aortic disruption. Tex Heart Inst J. 2005;32(1):16-20.
- Krzyston H, Kumari D. Stent grafting for traumatic arterial injuries.
- Reuben B, Whitten M, Sarfati M, Kraiss L. Increasing use of endovascular therapy in acute arterial injuries: analysis of the National Trauma Data Bank. J Vasc Surg. 2007;46(6):1222-1226. doi:10.1016/j.jvs.2007.08.023.
- Branco B, Naik-Mathuria B, Montero-Baker M. Increasing use of endovascular therapy in pediatric arterial trauma. J Vasc Surg. 2017;66(4):1175-1183. doi:10.1016/j.jvs.2017.04.072.
- Nordmeyer J, Kramer P, Berger F, Schubert S. Successful exclusion of an aortic aneurysm with a novel PTFE-tube covered cobalt-chromium stent in a pediatric patient with native coarctation of the aorta. Catheter Cardiovasc Interv. 2018;92(5):930-934. doi:10.1002/ccd.27647.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Contained Abdominal Aortic Rupture. Applied Radiology. 2026. doi:10.37549/AR-D-25-0097.