1 University of Arizona College of Medicine, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Mercy Children’s Hospital, Kansas City, Missouri
4 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Croup often is diagnosed by clinical history and physical examination. A radiograph of the airway confirms the symmetric subglottic narrowing of the trachea creating the steeple sign. Patients are treated based on the severity of their symptoms. This care ranges from supportive management at home to inpatient hospitalization with supplemental oxygen.
Keywords
airway, infection
Categories
Case Summary
A toddler presented to the emergency room with a barky cough and stridor. On physical examination, there was tachycardia, stridor at rest, and retractions with respiration. Pulse oximetry identified oxygen saturation levels as low as 87%.
Imaging Findings
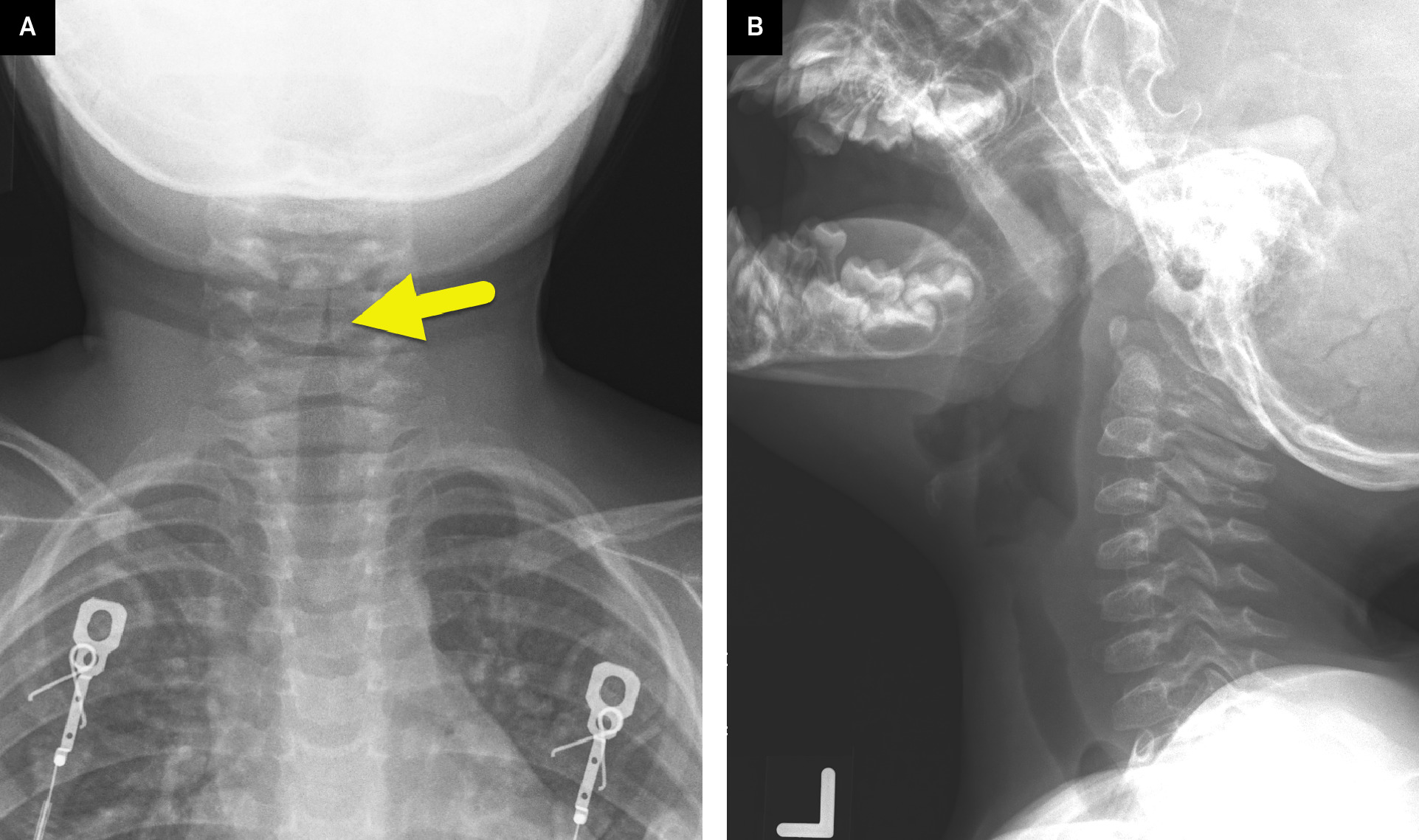
Radiograph of the airway (Figure 1) showed symmetric narrowing of the subglottic airway and moderate ballooning of the pharynx.
Diagnosis
Croup.
The differential diagnosis for the clinical features of croup includes bacterial tracheitis, subglottic hemangioma, tracheal and esophageal foreign bodies, angioneurotic edema, and congenital subglottic stenosis. 1
Discussion
Laryngotracheobronchitis, commonly referred to as croup, is an acute viral upper respiratory infection typically caused by the parainfluenza virus. Croup is defined by inflamed airway mucosa that may cause respiratory distress. The condition predominantly affects the pediatric population with involvement of the larynx and trachea and large bronchi. 2
About 15% of children below age 4 will contract croup at least once, while 1.7-6.4% of children experience recurrent croup. 3 Croup commonly manifests as a runny nose, pharyngitis, and fever during the initial phase. As the illness progresses, an increase in subglottic inflammation and swelling occurs, accompanied by a seal-like or barking cough. These symptoms are exacerbated at night. 4 Young patients experience a state of respiratory distress as an increase in mucus production and heightened inflammatory immune response causes the airway to narrow. 2
Croup is primarily caused by the parainfluenza virus. However, other viruses such as the influenza viruses, adenovirus, respiratory syncytial virus, or SARS-CoV-2 (COVID) can cause similar symptoms. The implicated viruses explain the illness’s predilection for occurring during the fall and winter months. Viral croup affects children ages 6 months to 6 years old.
Bacterial tracheitis differs from croup. However, patients may first become infected with a croup-causing virus. A secondary bacterial infection may then occur, causing more severe symptoms. Staphylococcus aureus, Streptococcus pneumoniae, and Streptococcus pyogenes are the most common pathogens associated with bacterial tracheitis. Patients with bacterial tracheitis are typically older than those with croup, with infection most common in those 5-10 years of age.
Diagnosis of croup heavily relies on the stereotypical triad of cough, inspiratory stridor, and hoarseness. 5 Despite the sound, the “croupy” cough is not a major threat to the child’s health status, but rather serves as a clinical signifier in determining the differential diagnosis. 4 The mild form of croup presents with fever, runny nose, and pharyngitis. In the most severe stage of infection, breathing becomes more taxing, leading to inspiratory stridor caused by air forcefully passing through narrowed airways during inspiration and expiration. The clinical presentation, along with imaging, solidifies the diagnosis, rather than any laboratory findings.
In patients with croup, airway and chest radiography are usually all that are necessary. The anteroposterior airway radiograph shows symmetric subglottic narrowing of the airway. 6 This appearance of the airway is described as the steeple sign due to the appearance of the airway mimicking a church’s steeple. This serves as a classic diagnostic finding for croup with a 93% sensitivity and 92% specificity. 7 The steeple appearance of the airway in patients with croup differs from the normal subglottic shouldering of the airway, which has an appearance more like a cupola. On the frontal radiography, the subglottic swelling changes the shape to a steeple. The lateral radiograph may show ballooning of the pharynx due to the upper airway obstruction and ill-definition of the larynx and subglottic trachea. Bacterial tracheitis appears differently on lateral radiograph with irregularity of the subglottic airway. A chest radiograph is often performed at the same time as airway radiographs to help exclude other causes of respiratory distress such as pneumonia.
Croup is a self-limited infection. Patients with mild symptoms are treated with supportive therapy. The nighttime symptoms can be relieved with warm wet air (achieved by turning on the shower in a closed bathroom) or colder dry air. Those with more severe symptoms, including respiratory distress, are treated with nebulized epinephrine and steroids. Most patients do well with a single treatment. Those with more severe disease may require hospitalization, oxygen support, and additional epinephrine treatments.
Conclusion
Croup often is diagnosed by clinical history and physical examination. Radiograph of the airway confirms the symmetric subglottic narrowing of the trachea creating the steeple sign. Patients are treated based on the severity of their symptoms. This care ranges from supportive management at home to inpatient hospitalization with supplemental oxygen.
References
- Gaillard F, Kearns C, Murphy A. Croup. Reference article. Radiopaedia.org. doi:10.53347/rID-1185.
- Moraa I, Sturman N, McGuire T, van Driel M. Heliox for croup in children. Cochrane Database Syst Rev. 2021;8(8). doi:10.1002/14651858.CD006822.pub6.
- Sowa L, Stillwell P, Houin P. Prophylactic inhaled corticosteroids for the management of recurrent croup. Int J Pediatr Otorhinolaryngol. 2023;170:111600. doi:10.1016/j.ijporl.2023.111600.
- Baiu I, Melendez E. Croup. JAMA. 2019;321(16):1642. doi:10.1001/jama.2019.2013.
- Burton L, Lofgren D, Silberman M. StatPearls [Internet]. 2024.
- Roebuck D, Murray C, McLaren C. Imaging of airway obstruction in children. Front Pediatr. 2020;8. doi:10.3389/fped.2020.579032.
- Yang W, Hsu Y, Chen C. Initial radiographic tracheal ratio in predicting clinical outcomes in croup in children. Sci Rep. 2019;9(1). doi:10.1038/s41598-019-54140-y.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Croup. Applied Radiology. 2025. doi:10.37549/JPCR-25-0030.