1 College of Medicine, University of Central Florida, Orlando, Florida
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, University of College of Medicine, Cincinnati, Ohio
4 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Discitis is an intervertebral disc infection in young children most caused by S. aureus or K. kingae. Symptomatic patients most commonly present with back pain, refusal to walk or crawl, loss of lumbar lordosis, and inability to flex the lower back. The first-line diagnostic tool is MRI, which demonstrates a shortened, inflamed disc. Treatment generally consists of bed rest in combination with IV and oral empiric antibiotic therapy over the course of several weeks.
Keywords
spine, infection, children
Categories
Case Summary
A teenager with a history of chronic granulomatous disease and bone marrow transplantation presented with low back pain that progressed over the course of several weeks. The patient’s pain worsened during flexion and extension of the back.
Imaging Findings
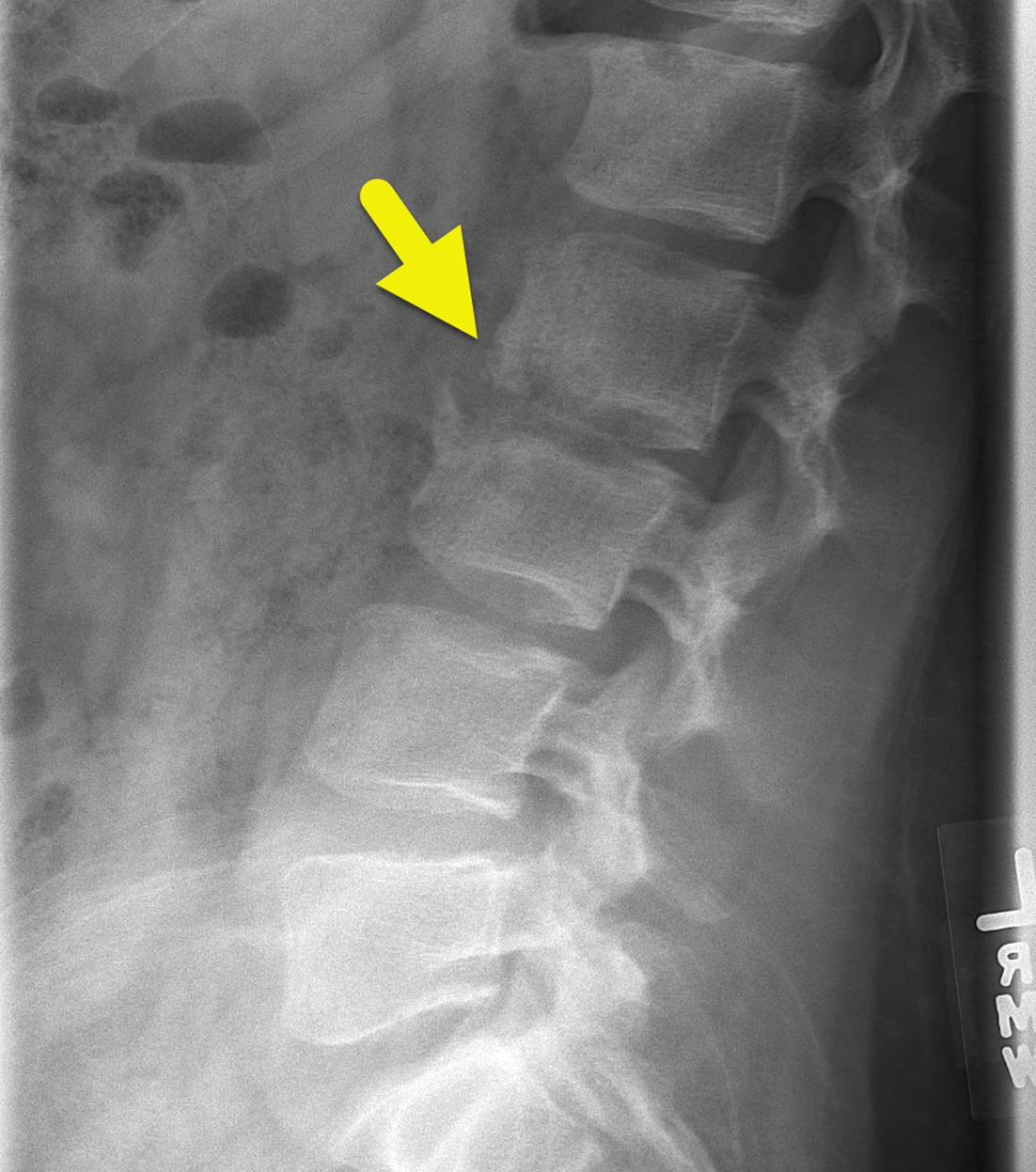
Radiographs of the lumbar spine (Figure 1) showed narrowing of the anterior aspect of the L2/L3 disc with destructive changes at the facing anterior corners of the L2 and L3 vertebral bodies.
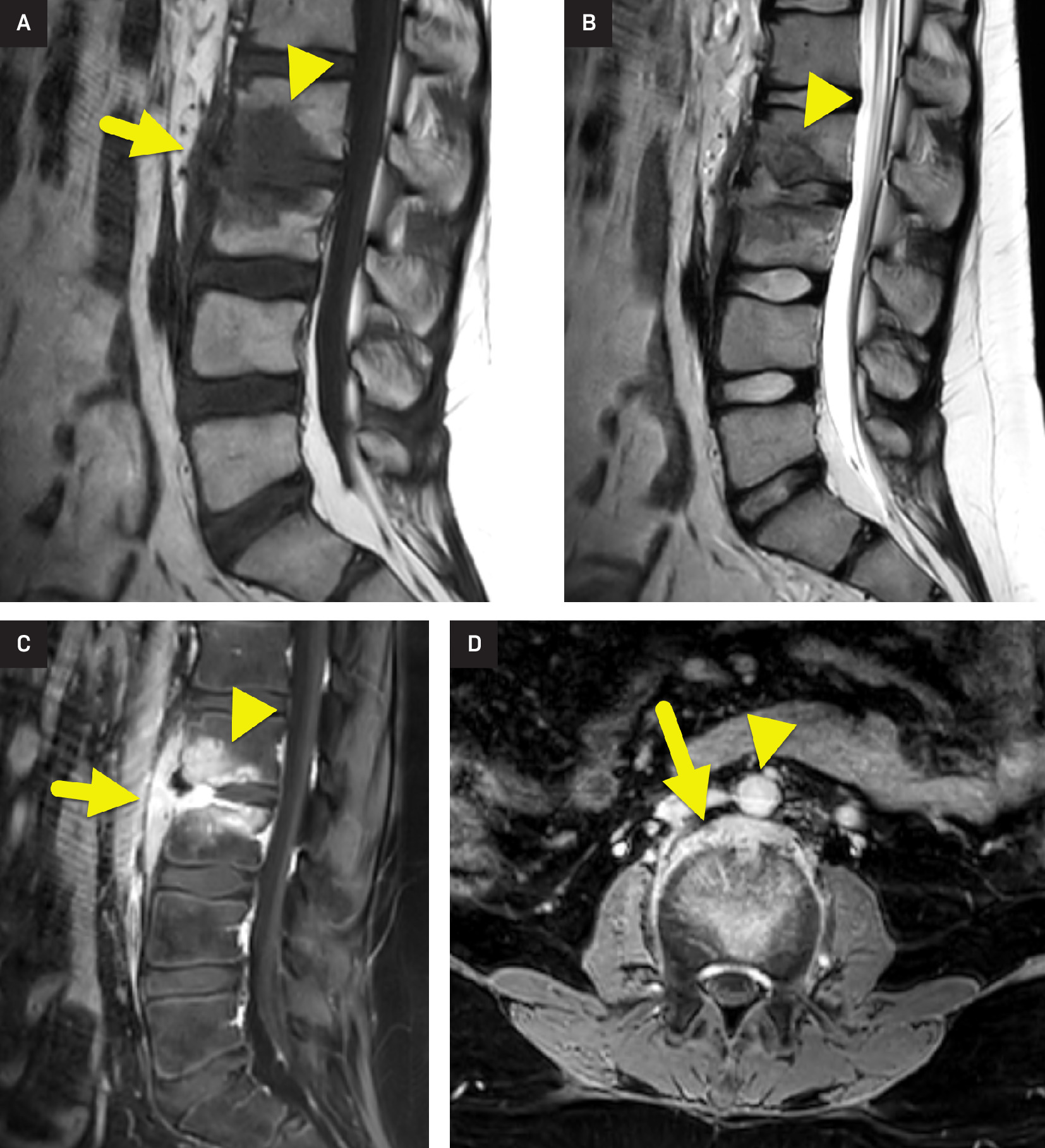
Further evaluation with MRI of the spine (Figure 2) demonstrated end plate erosion, a narrowed L2-L3 disc space, and abnormal adjacent bone marrow signal. Edema and enhancement were also found within the prevertebral soft tissues at the L2-L3 level, resulting in elevation of the abdominal aorta. After administration of contrast, there was enhancement of the L2 and L3 vertebral bodies and the L2-L3 disc.
Diagnosis
L2-L3 discitis/osteomyelitis.
The differential diagnosis for low back pain in children or adolescents includes spondylosis, spondylolisthesis, disc herniation, and inflammatory arthritis.
Discussion
Discitis refers to an infection of the intervertebral disc space. It typically affects the lumbar spine and most frequently occurs in children under the age of 5 years. 1 Studies indicate that the infection begins as microabscesses in the vertebral body near the end plate. 2,3 Then, due to the increased vascularity of the intervertebral space in young children, the infection spreads to the disc upon rupture of the abscesses. 4,5
The presentation of discitis most commonly includes the refusal to walk or crawl, inability to flex the lower back, loss of lumbar lordosis, and back pain. 6,7 Notably, patients with discitis do not typically present with a fever. 1 Lab results demonstrate an elevated erythrocyte sedimentation rate and platelet count in >90% of cases. However, for unknown reasons, the white blood cell count and C-reactive protein levels are typically within normal ranges. 8 Blood cultures of patients with discitis are also almost always sterile, and disc biopsy cultures grow bacteria in only approximately 60% of cases. 2,9 Because these observations do not clearly represent an infectious cause, it may be challenging for physicians to discover the true origin of the patient’s symptoms.
Staphylococcus aureus is the pathogen most frequently found to grow on vertebral disc cultures of patients with discitis. 4,10,11 Kingella kingae is also thought to be a common cause and is likely to be the source of infection in patients whose disc cultures come back negative as it is difficult to grow on typical culture media. In support of this theory, one study found that the K. kingae RTX toxin gene was discovered in the oropharynx of a significantly larger percentage of children with confirmed discitis compared with those without. 8
Although a biopsy of the disc space may identify an infectious organism, this is not necessary for the diagnosis of discitis. Biopsies are not typically recommended due to the risks associated with the procedure as well as the high frequency of false-negative results. 7 Vertebral imaging is generally the preferred diagnostic tool as it is non-invasive and highly accurate.
Plain radiographs of a patient with discitis will demonstrate intervertebral disc space narrowing. In more advanced cases of the disease, destruction of the neighboring vertebral end plates and disc herniation into the vertebral body may also be observed. 1,7 However, abnormalities may not be seen at all on plain radiographs during the first 2 weeks following the onset of the illness. The observation of a normal spine during this time may lead the physician to believe that nothing is wrong. A bone scan may be used as it can localize inflammation within the spine earlier. The findings on a bone scan, however, lack specificity and cannot differentiate discitis from other pathologies. 10
MRI is the imaging modality of choice in the diagnosis of discitis as it demonstrates high sensitivity and specificity compared with other techniques. Additionally, in contrast to plain radiographs, MRI can detect changes from the onset of the illness, reducing diagnostic delay and allowing appropriate treatment to begin as soon as possible. 6 Typical MR findings include decreased disc height, disc hypointensity on T1-weighted images, and disc hyperintensity on T2-weighted images. 11 In cases where the vertebral bodies have been significantly affected by the infection, the end plates will appear irregular and blurred. Later in the disease process, the end plates and vertebrae may become bright on T2-weighted images. 3
Due to limited data, there is not yet a standardized treatment regimen for discitis, and recommendations regarding the route and duration of antibiotic therapy vary. However, data suggest that treating the child with intravenous antibiotics prior to oral therapy is associated with an earlier response and fewer relapses than treatment with oral antibiotics or analgesia alone. 2,11 Therefore, most researchers agree that antibiotics should initially be administered intravenously for several days (up to 2 weeks). Then, when signs of improvement are present, the patient may be transitioned to oral antibiotics for 2 additional weeks. Antibiotic therapy should be directed against S. aureus and K. kingae. Bed rest with immobilization, throughout the course of antibiotic treatment, is recommended to assist with pain control. 11
The prognosis of appropriately managed discitis in children is generally good. Approximately 80% of patients in one retrospective study reported unrestricted mobility and the absence of pain more than 10 years following treatment. 10 The other 20% of cases reported relatively mild pain for which pain relievers were not required. Despite most patients denying any lasting symptoms, nearly all patients showed persistent radiographic abnormalities. These include narrowing of the intervertebral disc space (100%), fibrous ankylosis (60%), and vertebral fusion (40%).
Conclusion
Discitis is an intervertebral disc infection in young children mostly caused by S. aureus or K. kingae. Symptomatic patients most commonly present with back pain, refusal to walk or crawl, loss of lumbar lordosis, and inability to flex the lower back. The first-line diagnostic tool is MRI, which demonstrates a shortened, inflamed disc. Treatment generally consists of bed rest in combination with intravenous and oral empiric antibiotic therapy over the course of several weeks.
References
- Fernandez M, Carrol C, Baker C. Discitis and vertebral osteomyelitis in children: an 18-year review. Pediatrics. 2000;105(6):1299-1304. doi:10.1542/peds.105.6.1299.
- Ring D, Johnston C, Wenger D. Pyogenic infectious spondylitis in children: the convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop. 1995;15(5):652-660. doi:10.1097/01241398-199509000-00021.
- Tyagi R. Spinal infections in children: a review. J Orthop. 2016;13(4):254-258. doi:10.1016/j.jor.2016.06.005.
- Rossi A. Pediatric spinal infection and inflammation. Neuroimaging Clin N Am. 2015;25(2):173-191. doi:10.1016/j.nic.2015.01.001.
- Tay B, Deckey J, Hu S. Spinal infections. J Am Acad Orthop Surg. 2002;10(3):188-197. doi:10.5435/00124635-200205000-00005.
- Brown R, Hussain M, McHugh K, Novelli V, Jones D. Discitis in young children. J Bone Joint Surg Br. 2001;83(1):106-111. doi:10.1302/0301-620x.83b1.10865.
- Karabouta Z, Bisbinas I, Davidson A, Goldsworthy L. Discitis in toddlers: a case series and review. Acta Paediatr. 2005;94(10):1516-1518. doi:10.1111/j.1651-2227.2005.tb01832.x.
- Ceroni D, Belaieff W, Kanavaki A. Possible association of Kingella kingae with infantile spondylodiscitis. Pediatr Infect Dis J. 2013;32(11):1296-1298. doi:10.1097/INF.0b013e3182a6df50.
- Dayer R, Alzahrani M, Saran N. Spinal infections in children: a multicentre retrospective study. Bone Joint J. 2018;100-B(4):542-548. doi:10.1302/0301-620X.100B4.BJJ-2017-1080.R1.
- Kayser R, Mahlfeld K, Greulich M, Grasshoff H. Spondylodiscitis in childhood: results of a long-term study. Spine. 2005;30(3):318-323. doi:10.1097/01.brs.0000152097.57891.98.
- Principi N, Esposito S. Infectious discitis and spondylodiscitis in children. Int J Mol Sci. 2016;17(4). doi:10.3390/ijms17040539.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Discitis. Applied Radiology. 2025. doi:10.37549/JPCR-25-0013.