1 Idaho College of Osteopathic Medicine, Meridian, Idaho
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
Abstract
Duodenal atresia is a congenital malformation caused by a failure of intestinal recanalization. It is often diagnosed prenatally when a classic double bubble appearance of the dilated stomach and duodenum is identified. Once diagnosed, the definitive treatment for duodenal atresia is surgery.
Keywords
congenital, gastrointestinal track
Categories
Case Summary
A neonate presented to the emergency department with vomiting. The patient was afebrile, but irritable, with a soft abdomen. Subsequently, an abdominal radiographic was obtained.
Imaging Findings
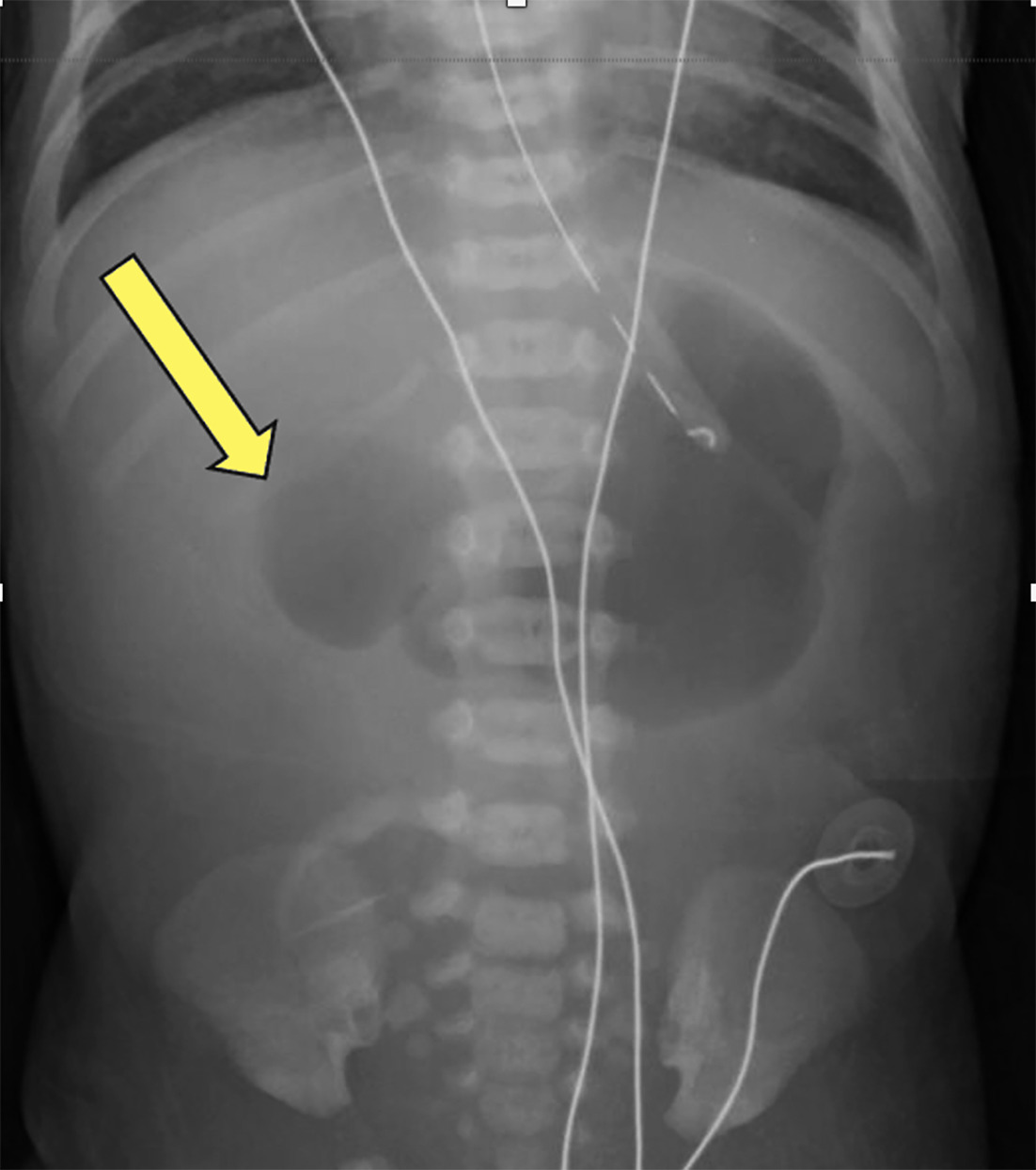
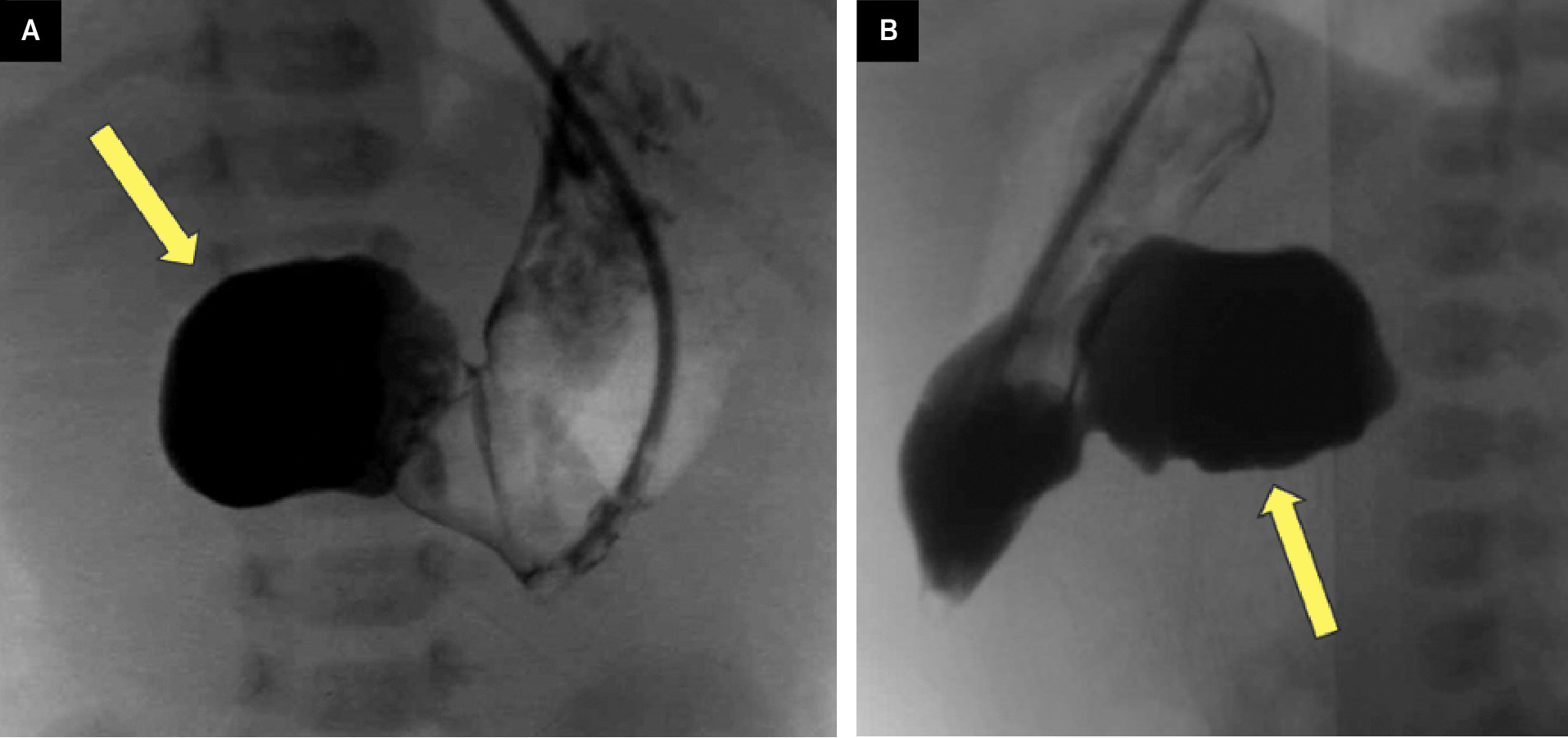
An abdominal radiograph (Figure 1) showed a dilated stomach and proximal duodenum (double bubble) with the absence of distal bowel gas. A subsequent upper gastrointestinal (UGI) study (Figure 2) was performed that confirmed the dilation of the stomach and proximal duodenum with no passage of contrast distally.
Diagnosis
Duodenal atresia.
Duodenal atresia results in a complete obstruction of the small intestine. Other conditions that cause a proximal small bowel obstruction in a neonate include intrinsic lesions such as duodenal stenosis and a duodenal web. Extrinsic causes of a proximal obstruction in a neonate include malrotation with midgut volvulus and annular pancreas. 1
Discussion
Duodenal atresia is a rare congenital abnormality affecting 2.5-10 per 100,000 live births. It is caused by a failure of the normal intestinal development. Normally, recanalization of the intestines occurs at 8-10 weeks of gestation. Failure of recanalization can result in an intestinal atresia or a web. 2 Duodenal atresia is the most common atresia, accounting for 25-49% of all intestinal atresias. 1 If not diagnosed in utero, patients present with bilious or non-bilious vomiting, which usually occurs after the first feeding. 3
It has been suggested that loss of function of fibroblast growth factor 10 (FGF10) is linked to duodenal atresia. 4 FGF10 regulates cell differentiation during fetal development and is associated with budding and branching interactions between the mesenchyme and epithelium in mice. 4 Loss of FGF10 function is also linked to other congenital anomalies such as pulmonary agenesis and esophageal atresia. 4
Duodenal atresia is associated with trisomy 21. One-third of patients with Trisomy 21 have been found to have duodenal atresia, making it the second most common associated congenital abnormality. Congenital heart disease is the most common anomaly with a frequency of 40-60%. 3
Overall, duodenal atresia and duodenal stenosis account for 35-40% of all intrinsic causes of congenital intestinal obstruction, happening in 1 in 6,000 live births. 1 Intestinal webs account for 5-15% of congenital causes of small bowel obstruction, 1 while annular pancreas occurs in 1 to 12,000-15,000 live births. 1 Of note, there is also no gender disparity within the broad umbrella of intestinal atresia.
Patients with duodenal atresia are typically diagnosed in utero. Pregnancies are complicated by polyhydramnios and premature delivery. In utero diagnosis is made via prenatal US showing polyhydramnios and a fluid-filled double bubble of the dilated stomach and proximal duodenum. A similar finding is present on fetal MRI. Once duodenal atresia is identified on prenatal imaging, one should look for other anomalies, including other intestinal atresia and other features of trisomy 21.
After birth, the diagnosis is typically made via abdominal radiograph. Initial radiographs may appear normal, before the neonate has swallowed enough air to distend the stomach and duodenum. However, after several hours, an air-filled double bubble is seen. Importantly, most patients with duodenal atresia have no distal bowel gas. If distal bowel gas is present, other causes should be considered. These causes can be intrinsic such as a duodenal web or annular pancreas or malrotation with midgut volvulus. Rarely, distal bowel gas is present in neonates with duodenal atresia. In these instances, air can pass distally via a biliary or pancreatic ductal anomaly.
If the diagnosis is in question, an UGI series can be performed. The UGI will show a blind-ending duodenum. This can be accentuated by placing a nasogastric tube into the stomach and injecting contrast. Nasogastric injection increases gastric pressure and can uncover a tight stenosis. Delayed radiographs are also helpful to identify contrast in distal bowel loops.
Definitive treatment for duodenal atresia is surgery. Patients are hydrated with intravenous fluids, and any electrolyte imbalances are corrected before surgery is performed. 7 Laparoscopic duodenoduodenostomy is the preferred approach. Open surgery is reserved for patients who are not candidates for laparoscopic repair. The survival rate for children with duodenal atresia or stenosis is 90-95%. However, associated anomalies, when present, may have a significant impact on survival.
Conclusion
Duodenal atresia is a congenital malformation caused by a failure of intestinal recanalization. It is often diagnosed prenatally when a classic double-bubble appearance of the dilated stomach and duodenum is identified. Once diagnosed, the definitive treatment for duodenal atresia is surgery.
References
- Patterson K, Cruz S, Nwomeh B, Diefenbach K. Congenital duodenal obstruction - advances in diagnosis, surgical management, and associated controversies. Semin Pediatr Surg. 2022;31(1):151140. doi:10.1016/j.sempedsurg.2022.151140.
- St. Peter S, Little D, Barsness K. Should we be concerned about jejunoileal atresia during repair of duodenal atresia?. J Laparoendosc& Adv Surg Tech. 2010;20(9):773-775. doi:10.1089/lap.2010.0173.
- Bethell G, Long A, Knight M, Hall N. The impact of trisomy 21 on epidemiology, management, and outcomes of congenital duodenal obstruction: a population-based study. Pediatr Surg Int. 2020;36(4):477-483. doi:10.1007/s00383-020-04628-w.
- Teague W, Jones M, Hawkey L. FGF10 and the mystery of duodenal atresia in humans. Front Genet. 2018;9. doi:10.3389/fgene.2018.00530.
- Millar A, Cox S, Gosche J, Lakhoo K. Intestinal Atresia and Stenosis. 2020. doi:10.1007/978-3-030-41724-6_63.
- Sigmon D, Eovaldi B, Cohen H. StatPearls. 2022.
- Kandasamy D, Sharma R, Gupta A. Bowel imaging in children: part 1. Indian J Pediatr. 2019;86(9):805-816. doi:10.1007/s12098-019-02877-9.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Duodenal Atresia. Applied Radiology. 2025. doi:10.37549/JPCR-25-0016.