Embolization of Intercostal Artery Pseudoaneurysm Secondary to Active Tuberculosis
Applied Radiology — Vol. 55 , Issue 4
Published: May 1, 2026
1 Department of Radiology, SUNY Downstate Medical Center, Kings County Hospital Center, Brooklyn, New York
* Corresponding author: Mousa Payinkay (mousa.payinkay@downstate.edu)
Abstract
We present a novel case of embolization for a patient presenting with chronic episodes of hemoptysis, found to have a pseudoaneurysm arising from a branch of the L5 intercostal artery secondary to active tuberculosis (TB). The expectant management for pseudoaneurysm in this location would be radiological intervention for identifying and embolizing the pseudoaneurysm. This case is unique given its atypical location and several feeder branches, making the treatment approach more challenging. In addition, a concomitant pseudoaneurysm with active TB predisposes the patient to multiple etiologies for hemoptysis that make management further complicated. Ultimately, the patient was treated with acute coil embolization of the pseudoaneurysm and placed on a prolonged course of the RIPE (Rifampin, Isoniazid, Pyrazinamide, and Ethambutol) regimen for active TB, resulting in resolving hemoptysis and overall clinical improvement. The patient’s case and the details of our intervention with relevant imaging are discussed throughout the report, as well as a brief overview of management for hemoptysis secondary to pseudoaneurysms.
Keywords
hemoptysis, RIPE, pseudoaneurysm, tuberculosis, embolization
Categories
Case Summary
A middle-aged adult presented with a 2-month history of fever, chills, and night sweats, along with a recent episode of hemoptysis consisting of 150 mL of bright red blood. The patient experienced one episode of hemoptysis 2 months prior but did not seek medical attention. The physical exam was significant for rhonchi breath sounds, with multiple episodes of small volume (<10 mL) hemoptysis in the setting of hemodynamic stability. Labs were significant for anemia, lactic acidosis, elevated liver function tests, and electrolyte abnormalities.
Imaging Findings
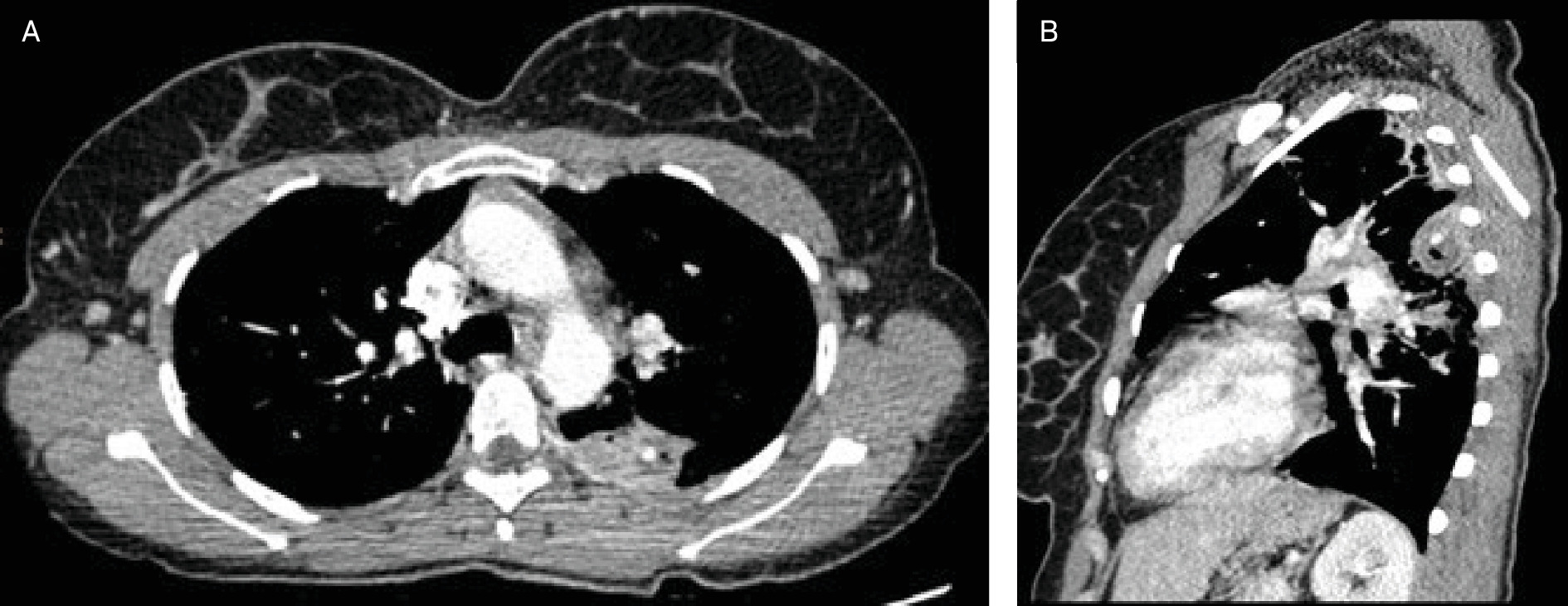
Chest radiography revealed prominent patchy airspace opacities and right apical and basilar airspace opacities in the left upper lobe, raising concerns for multifocal pneumonia. Subsequent chest CTA revealed a small (<1 cm) cavitary lesion in the right upper lobe and a 2 cm × 1.7 cm × 2.2 cm cavitating consolidative mass in the apical segment of the left lower lobe (Figure 1). The lesion contained high attenuation fluid, along with a discrete, 4 mm, rounded high-attenuation focus matching the attenuation of the arterial vasculature, raising concern for a pseudoaneurysm (PSA) (Figure 2).

The patient had a positive QuantiFERON and PCR test showing pan-sensitive mycobacterial tuberculosis (TB). Acid-fast Bacillus (ABF) smear was negative 3 times, indicating the patient was not actively contagious. The patient was placed on a RIPE regimen with pyridoxine 50 mg daily, tranexamic acid nebulizers Q8, and underwent urgent interventional radiology (IR) embolization.
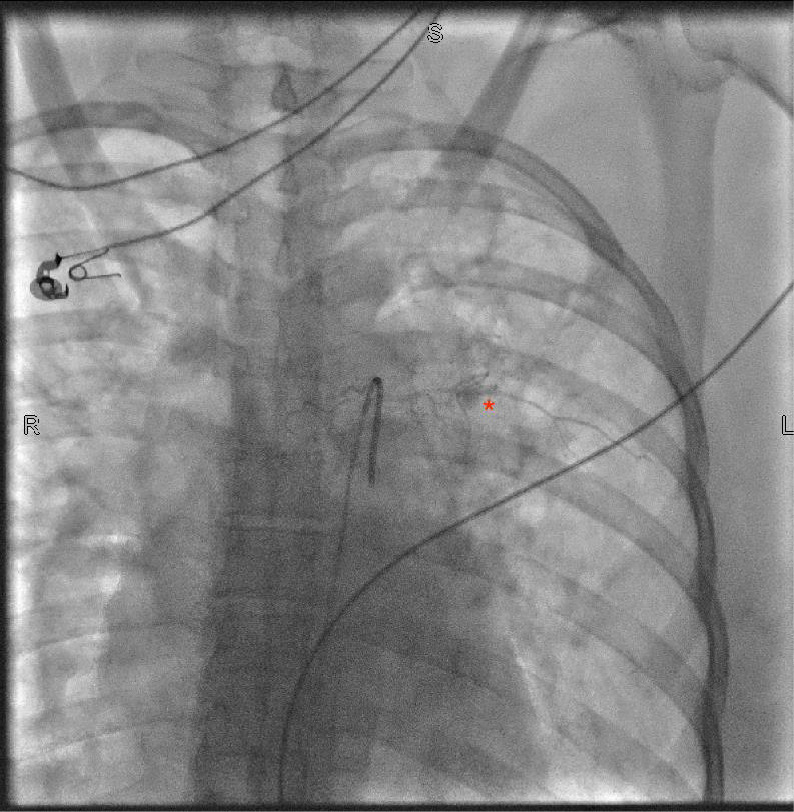
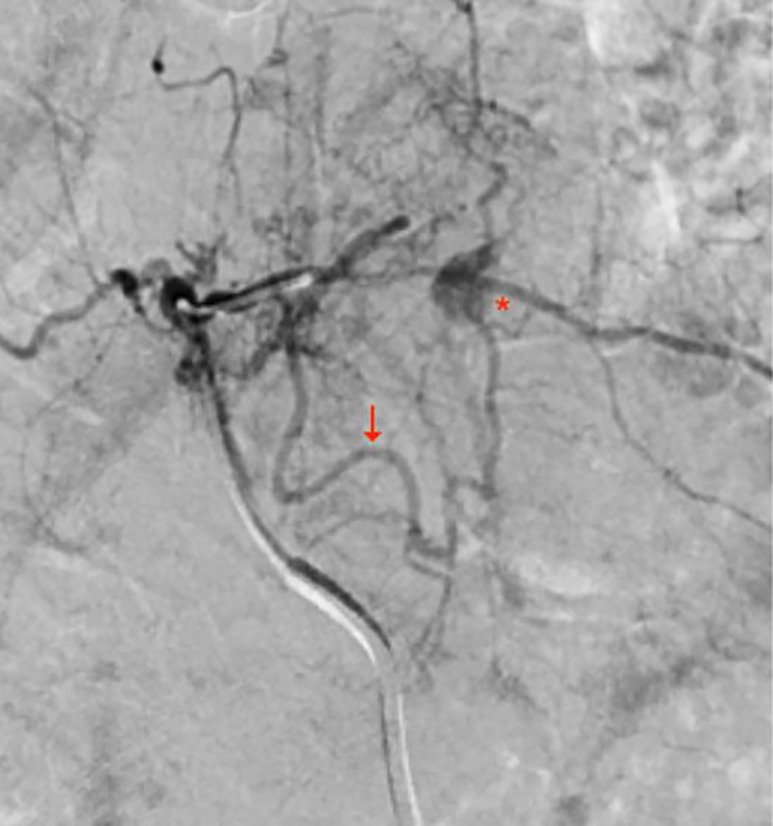
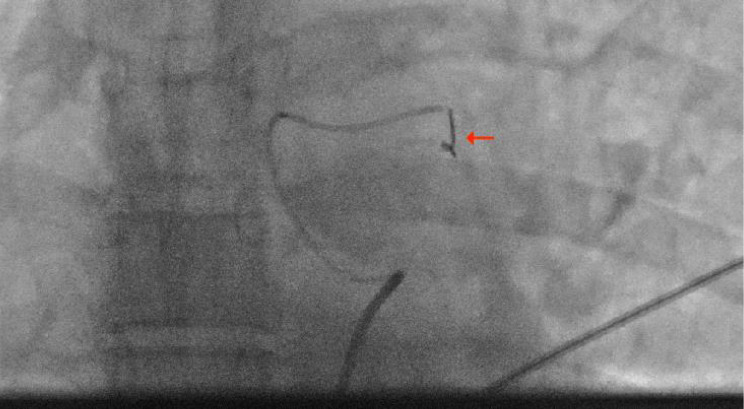
The patient underwent urgent arterial embolization utilizing a right femoral arterial approach. Arch aortogram was performed with subsequent bronchial artery angiograms. While attempting to identify the bronchial artery, the left T5 intercostal artery was opacified and inadvertently demonstrated a possible pseudoaneurysm (Figure 3). A digital roadmap image allowed for successful coaxial catheterization of the intercostal artery using a microcatheter. Hand injection identified the pseudoaneurysm and arteriogram identified a prominent feeder branch from the left intercostal artery that provided direct supply to the pseudoaneurysm (Figure 4) . The feeder branch was super-selectively coil embolized with a 2 mm x 1 cm Ruby microcoil (Figure 5) . Post-embolization angiograms showed delayed but persistent filling of the pseudoaneurysm with smaller caliber collateral branches from the intercostal artery. After unsuccessful attempts at selectively catheterizing the other feeder branches, it was decided against embolizing the proximal T5 intercostal artery.
Diagnosis
Intercostal PSA secondary to active TB.
Differential diagnoses include Rasmussen Aneurysm, septic emboli, and vasculitis.
Discussion
Pulmonary TB remains a significant global health concern as its incidence continues to rise despite efforts to reduce transmission rates. The current incidence rate in the United States is 2.9 per 100,000, which marks an increase compared with previous years.1 Massive hemoptysis, a life-threatening complication of TB, occurs in about 8% of infected individuals.2 While no clear consensus exists on the definition of massive hemoptysis, the condition is generally diagnosed when a patient has expectorated from > 100 mL of blood in 24 hours.
In TB infections, hemoptysis typically arises from the rupture of friable small vessels secondary to inflammation, PSA of the intercostal arteries, or the development of a Rasmussen’s aneurysm, a distinct pulmonary artery PSA within or adjacent to a tuberculous cavity.2-5 While the rate of PSA is rare, it carries a mortality rate of over 38%.3 Any of these vascular complications can progress to massive hemoptysis, and IR is frequently called on to intervene. There are no clear guidelines regarding embolization of PSAs; unique pitfalls may affect clinical outcomes even in cases of technical success. Roughly 90% of patients with hemoptysis experience bleeding resulting from the high-pressure bronchial circulation, with the other 10% experiencing bleeds from the aorta or nonbronchial circulation and the low-pressure pulmonary artery system.6
Most cases of life-threatening hemoptysis arise from the high-pressure systemic circulation; therefore, embolization strategies typically first target the bronchial arteries. However, non-bronchial systemic arteries (NBSAs)—including variable collateral supply from the intercostal, internal mammary, phrenic, or subclavian branches—are frequently overlooked sources of bleeding and represent major contributors to early rebleeding, particularly in the setting of chronic inflammatory or pleural disease.6 Pre-procedure multidetector CTA is essential for identifying enlarged bronchial arteries and ectopic NBSA feeders, allowing for accurate procedural planning and selective catheterization.6 In addition, the anatomic location of parenchymal cavitation can help predict the responsible systemic feeder, as posteriorly located cavitary disease often correlates with involvement of the corresponding intercostal artery.6
Bronchial artery embolization is typically performed using particles ≥300‐355 µm, with larger particles favored in the presence of arteriovenous shunting and careful attention paid to avoidance of spinal arterial branches.6 Embolization of NBSAs frequently requires super-selective catheter positioning and, when the risk of non-target embolization is high, the use of controlled embolic agents such as coils.7 Hemoptysis stemming from pulmonary arterial lesions (eg, Rasmussen PSA) requires targeted pulmonary artery embolization, often combined with systemic treatment. With respect to intercostal artery PSAs, there remains no clear consensus regarding optimal embolic agent selection. Successful reports in the literature have used microcoils with or without glue, alcohol, and/or Gelfoam.4,5,7-10 In our case, we utilized microcoils to reduce the risk of nontarget embolization. Of note, severe cases warrant consideration of thoracotomy.
A potential complication of intercostal artery embolization is spinal cord injury. The artery of Adamkiewicz, which supplies the anterior spinal artery of the thoracic and lumbar spinal cord segments, should be carefully sought and avoided to prevent infarction and the development of long-term neurological complications. Radicular branches from the proximal intercostal arteries should also be avoided for similar reasons. Therefore, selective embolization should be employed. Bleeding sources close to the radicular orifices are typically treated with coils to limit inadvertent embolization.7,10
Numerous collateral pathways supplying intercostal artery PSAs may represent a source of treatment failure and, when identified, should ideally be embolized.4,9 As demonstrated in our case, the PSA was supplied by multiple feeder branches, with post-embolization angiography showing delayed yet persistent filling.9 Another contributor to treatment failure is the coagulopathy that can accompany massive hemoptysis, such that technically successful embolization may not immediately translate into clinical hemostasis, resulting in persistent postprocedural bleeding.6 In our case, we were able to acutely stabilize and improve the patient’s hemoptysis. The condition progressively resolved over several weeks with medical management, including an anti-tuberculous regimen. This emphasizes the importance of a multidisciplinary approach and longitudinal care in complex cases.
Conclusion
In cases of hemoptysis, IR is frequently called upon to intervene and prevent rapid patient deterioration. Preprocedural CTA is vital for diagnosis and mapping. While the bronchial arteries are common culprits, recognition of nonbronchial sources is crucial to increasing the chance of technical success and positive patient outcomes. Medical management also plays a key role throughout the patient’s stay, highlighting the importance of taking a multidisciplinary approach to complex cases. Our coil embolization is one of only a few reported in the literature, with no consensus for the best embolic to use in these cases. Our success in this study warrants further research into how to best embolize and manage rare yet life-threatening PSAs.
References
- Reported tuberculosis in the United States, 2023. 2024.
- Seedat U, Seedat F. Post-primary pulmonary TB haemoptysis - when there is more than meets the eye. Respir Med Case Rep. 2018;25:96-99. doi:10.1016/j.rmcr.2018.07.006.
- Mikanović M, Markelić I, Boras Z. Pseudoaneurysm as an etiological cause of hemoptysis in extensive tuberculosis. Thorac Res Pract. 2023;24(2):113-116. doi:10.5152/ThoracResPract.2023.22012.
- Sharma M, Singhal M, Kamble R. Intercostal artery pseudoaneurysm in pulmonary tuberculosis - a rare cause of hemoptysis: a case report with review of the literature. Lung India. 2019;36(1):63-65. doi:10.4103/lungindia.lungindia_87_18.
- Chatterjee K, Colaco B, Colaco C, Hellman M, Meena N. Rasmussen’s aneurysm: a forgotten scourge. Respir Med Case Rep. 2015;16:74-76. doi:10.1016/j.rmcr.2015.08.003.
- Khalil A, Parrot A, Nedelcu C. Severe hemoptysis of pulmonary arterial origin. Chest. 2008;133(1):212-219. doi:10.1378/chest.07-1159.
- Chemelli A, Thauerer M, Wiedermann F. Transcatheter arterial embolization for the management of iatrogenic and blunt traumatic intercostal artery injuries. J Vasc Surg. 2009;49(6):1505-1513. doi:10.1016/j.jvs.2009.02.001.
- Fenwick A, Omotoso P, Ferguson D. Endovascular management of unruptured intercostal artery aneurysms. CVIR Endovasc. 2019;2(1):2. doi:10.1186/s42155-018-0048-7.
- Martin-Champetier A, Di Bisceglie M, Ravaud S, Soussan J, Habert P. Successful embolization of a rasmussen aneurysm perfused by an intercostal artery using ethylene-vinyl alcohol copolymer. J Vasc Interv Radiol. 2023;34(6):1098-1100. doi:10.1016/j.jvir.2023.01.025.
- Ozoilo K, Stein M. Paraplegia complicating embolization for bleeding intercostal artery in penetrating trauma. Injury Extra. 2013;44(8):70-73. doi:10.1016/j.injury.2013.05.015.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Embolization of Intercostal Artery Pseudoaneurysm Secondary to Active Tuberculosis. Applied Radiology. 2026;55(4). doi:10.37549/AR-D-25-0086.