Esophageal Atresia and Tracheoesophageal Fistula
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -3
Published: November 1, 2025
1 College of Osteopathic Medicine, Rocky Vista University, Parker, Colorado
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, The University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
As a result of successful surgical repairs, esophageal atresia changed from a fatal to a livable condition. However, the residual effects of the anomaly may lead to a lifetime of complications related to the underlying deformity. The condition is often diagnosed via prenatal US, which shows a dilated, fluid-filled proximal esophagus, a small or absent stomach bubble, and polyhydramnios. Imaging plays a significant role in the diagnosis and management of this complex congenital anomaly.
Keywords
gastrointestinal track, congenital, esophageal
Categories
Case Summary
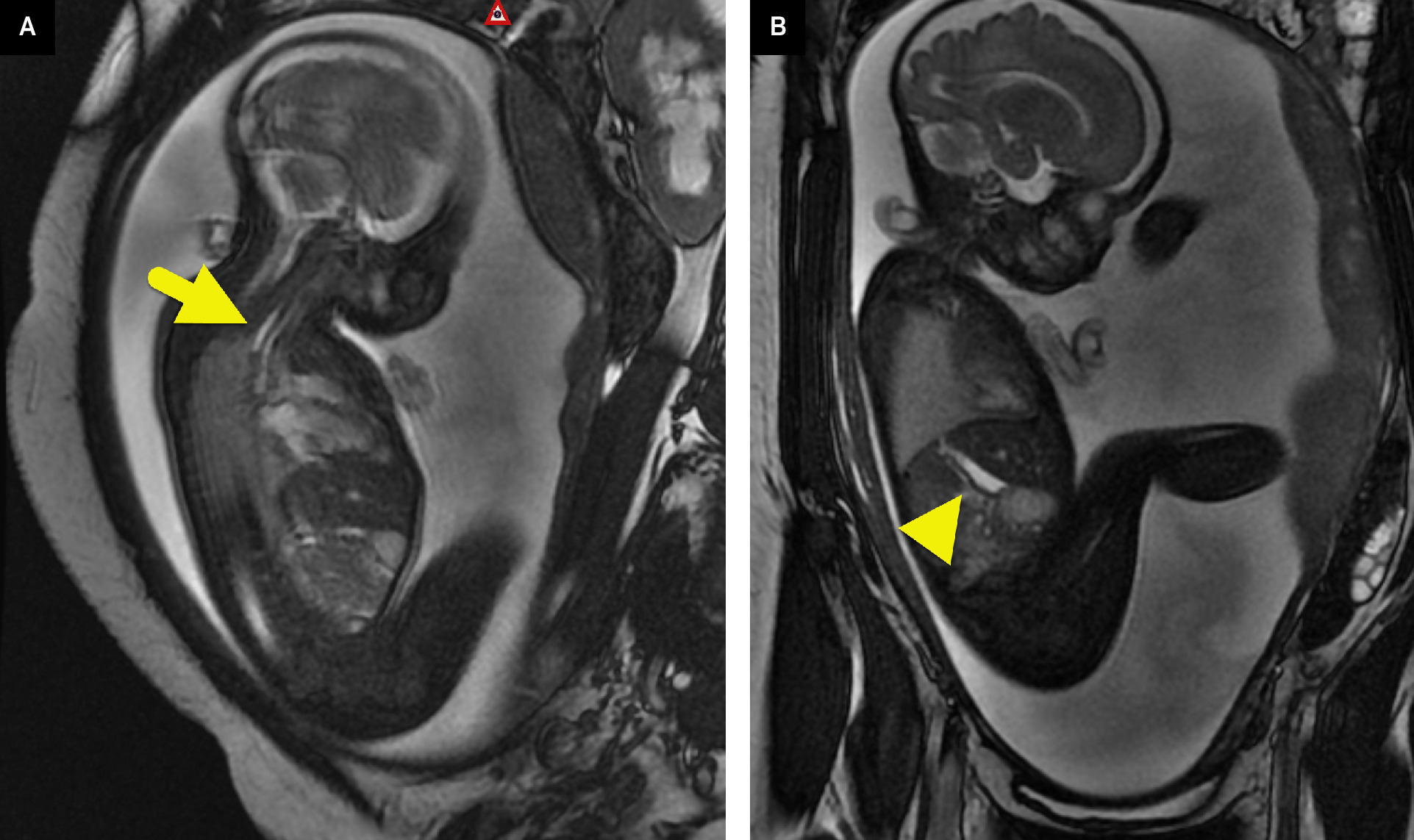
A fetal MRI was performed at 30 weeks’ gestation due to polyhydramnios and prenatal US findings of a small stomach.
Imaging Findings
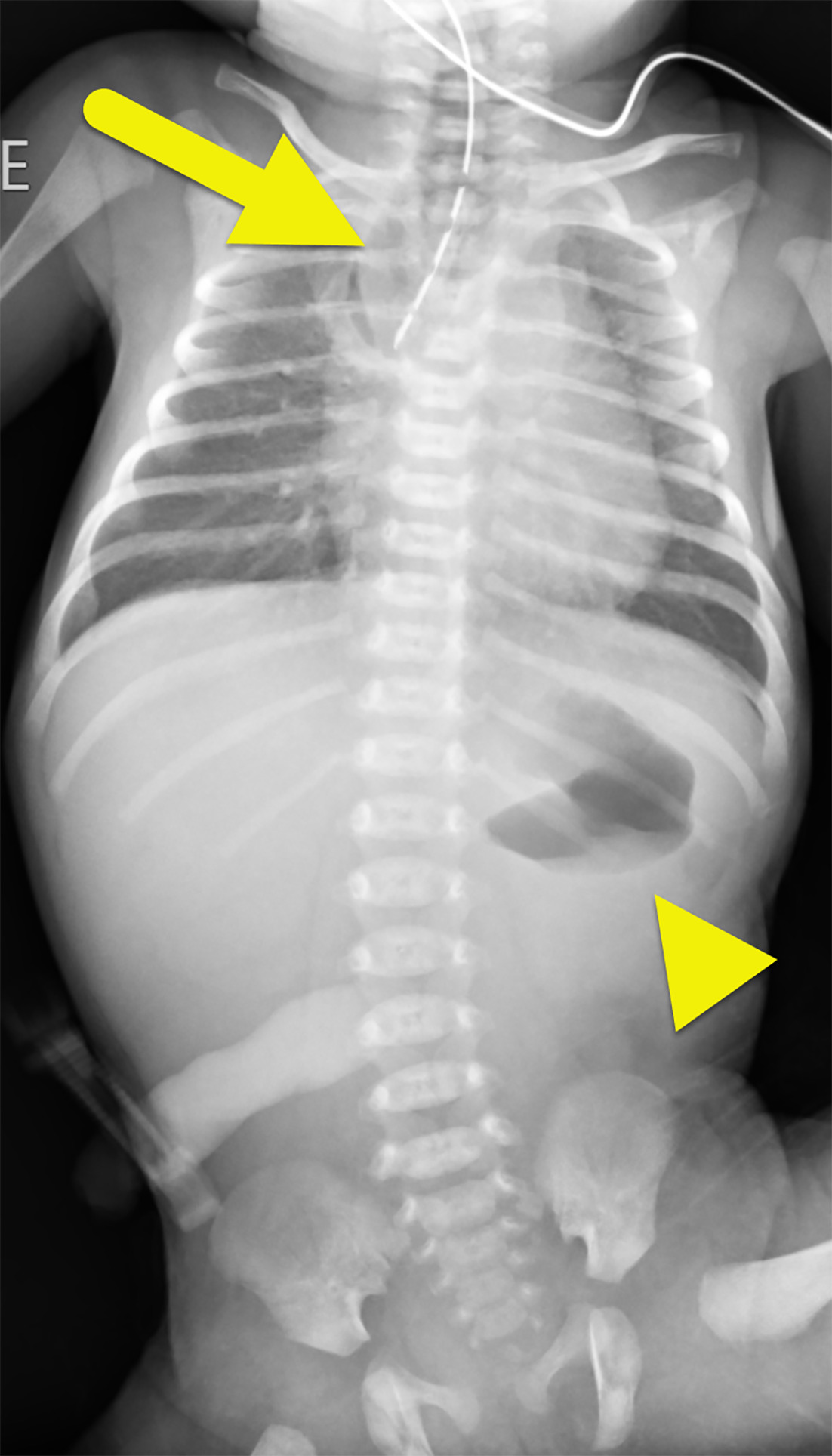
Fetal MRI (Figure 1) shows polyhydramnios and a fluid-filled proximal esophageal pouch. A small amount of fluid was also present in the stomach. A radiograph of the chest and abdomen (Figure 2) performed after birth shows an air-filled proximal esophageal pouch with a rounded distal margin. A Replogle tube extends to the distal portion of the esophageal pouch. A small amount of air was present within the stomach.
Diagnosis
Esophageal atresia (EA) and tracheoesophageal fistula (TEF).
The differential diagnosis includes a laryngotracheoesophageal cleft, congenital high airway obstruction, and tracheal agenesis.
Discussion
The trachea and esophagus are derived from the endoderm germ layer that forms the pharynx, esophagus, stomach, and the epithelial lines of the aerodigestive tract. A TEF occurs when the tracheoesophageal ridges fail to fuse between 4 and 6 weeks of gestation. The cause of EA is unknown.
EA occurs in approximately 1 in 3500 births. EA is typically associated with a TEF. However, both EA and TEF can occur in isolation. EA and TEF are typically classified into 1 of 5 types depending on the type of abnormality and the location of the fistula. Types and their frequency include 1
-
Type A: isolated EA (8%).
-
Type B: EA with a TEF fistula associated with the proximal esophagus (1%).
-
Type C: EA with a TEF associated with the distal esophagus (85%).
-
Type D: EA with a TEF associated with both the proximal and distal esophagus (1%).
-
Type E: isolated TEF (H-type TEF) (4%) without EA.
EA is associated with other congenital anomalies in 50% of patients. 2 Common associations include the VACTERL sequence (vertebral anomalies, anal atresia, cardiac defects, renal anomalies, and limb anomalies), CHARGE syndrome (coloboma, heart defect, choanal atresia, genital abnormality, and ear abnormality), trisomy 18, trisomy 21, and deletions of 22q11 or 17q22q23.3. 2
Patients with EA are usually diagnosed near birth. Symptoms include failure to pass a nasogastric tube and vomiting with every feed. Symptoms of TEF depend on the level of the fistula and the presence of EA. Patients with a fistula connected to the proximal esophagus or with an isolated TEF (H-type) present with choking when feeding and difficulty breathing. Milder symptoms such as paroxysmal coughing after swallowing fluids (Ono sign), and air movement between the esophagus and the trachea causing a high-pitched sound described as a “catlike cry” because of air moving from the esophagus to the trachea through the fistula. 3 Patients with a TEF connected to the distal esophagus may have a distended air-filled stomach.
EA can be diagnosed in utero. Prenatal US shows a small or absent stomach, polyhydramnios, and fluid-filled, blind-ending esophagus during fetal swallowing called “pouch sign.” These features are usually considered pathognomonic for EA. 4 Fetal MRI can show similar findings with a fluid-filled esophageal pouch, a small stomach, and polyhydramnios. Fetal MRI can also be used to identify other associated congenital anomalies.
Postnatally, EA is typically diagnosed on chest radiograph with a nasogastric tube in the proximal esophageal pouch. The location of a fistula can also be inferred by radiograph. Patients with a TEF connected to the distal esophagus will have bowel gas within the stomach and small bowel loops. If no bowel gas is present, the radiologist can infer that there is either a TEF connected to the proximal esophagus or isolated EA. While fluoroscopy can demonstrate a TEF connected to the proximal esophagus, it is rarely needed. Instead, fluoroscopy is reserved for patients where there is a concern for isolated TEF. In these patients, a nasoesophageal tube may be placed to decompress esophageal distention. If a fistula is present, it is best imaged with the patient in the lateral position. Postnatal CT and MRI are not needed to diagnose EA or TEF.
The surgical approach is planned according to the location of the TEF. The rare cervical and cervical-mediastinal TEF are best approached via a cervical incision with or without a median sternotomy. The mediastinal or intrathoracic TEF usually requires a right thoracotomy or a video-assisted thoracoscopic surgery. 5 EA with a short gap between segments may be amenable to immediate primary repair. Those patients with long gaps require a staged surgical approach prioritizing maintaining native esophagus. The staged approach esophageal lengthening procedures are utilized prior to delayed primary repair. In cases where the native esophagus cannot be salvaged, a gastric or colonic interposition may be necessary.
While EA has a low rate of early mortality (survival is >90%), morbidity is high during the first year of life (12-18%) due to the success of surgical management. 6 Risk factors for morbidity and mortality at 3 months of age include low birth weight, associated cardiac abnormalities, surgical complications, tracheomalacia, gastroesophageal reflux, esophageal dysmotility, and strictures. Cardiac malformations are the most strongly associated with mortality in patients with EA. In these patients, the TEF can lead to life-threatening respiratory morbidity.
Conclusion
As a result of successful surgical repairs, EA be changed from a fatal to a livable condition. However, the residual effects of the anomaly may lead to a lifetime of complications related to the underlying deformity. The condition is often diagnosed via prenatal US, which shows a dilated, fluid-filled proximal esophagus, a small or absent stomach bubble, and polyhydramnios. Imaging plays a significant role in the diagnosis and management of this complex congenital anomaly.
References
- Bluestone C. Pediatric Otolaryngology. 2003.
- Abou Chaar M, Meyers M, Tucker B. Twin pregnancy complicated by esophageal atresia, duodenal atresia, gastric perforation, and hypoplastic left heart structures in one twin: a case report and review of the literature. J Med Case Rep. 2017;11(1). doi:10.1186/s13256-016-1195-x.
- Nakazawa S, Yajima T, Numajiri K. A “catlike cry” as a symptom of congenital tracheoesophageal fistula. Chest. 2022;161(5). doi:10.1016/j.chest.2021.11.037.
- Bruhat C, Briac T, Delabaere A. Laryngotracheoesophageal cleft, a rare differential diagnosis of esophageal atresia. J Gynecol Obstet Hum Reprod. 2018;47(10):577-579. doi:10.1016/j.jogoh.2018.09.003.
- Bibas B, Cardoso P, Minamoto H, Pêgo-Fernandes P. Surgery for intrathoracic tracheoesophageal and bronchoesophageal fistula. Ann Transl Med. 2018;6(11). doi:10.21037/atm.2018.05.25.
- Sfeir R, Rousseau V, Bonnard A. Risk factors of early mortality and morbidity in esophageal atresia with distal tracheoesophageal fistula: a population-based cohort study. J Pediatr. 2021;234:99-105. doi:10.1016/j.jpeds.2021.02.064.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Esophageal Atresia and Tracheoesophageal Fistula. Applied Radiology. 2025;1(1):1-3. doi:10.37549/JPCR-25-0021.