Fetal Ureteropelvic Junction Obstruction
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 10, 2026
1 Central Michigan University, College of Medicine, Mount Pleasant, Michigan
2 Phoenix Children’s Hospital, Phoenix, Arizona
3 Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Ureteropelvic junction obstruction is the most common cause of congenital hydronephrosis and typically presents with dilation of the renal pelvis and calyces without associated ureteral dilation. Although many cases are suspected prenatally as urinary tract dilation, definitive evaluation occurs postnatally through integration of US findings and functional assessment. US remains the primary imaging modality, with CT or MR urography used when additional anatomic detail is required, particularly to evaluate for extrinsic causes. Renal drainage and differential function are most assessed with mercaptoacetyltriglycine-3 diuretic renography. Management is individualized based on symptoms, severity of dilation, and renal function. While many children are managed conservatively, surgical pyeloplasty is indicated in patients with significant obstruction or declining function and is associated with favorable long-term outcomes.
Keywords
genitourinary, renal, obstruction
Categories
Case Summary
A pregnant woman presented at 35 weeks’ gestation for advanced imaging following detection of prenatal hydronephrosis on routine screening US.
Imaging Findings
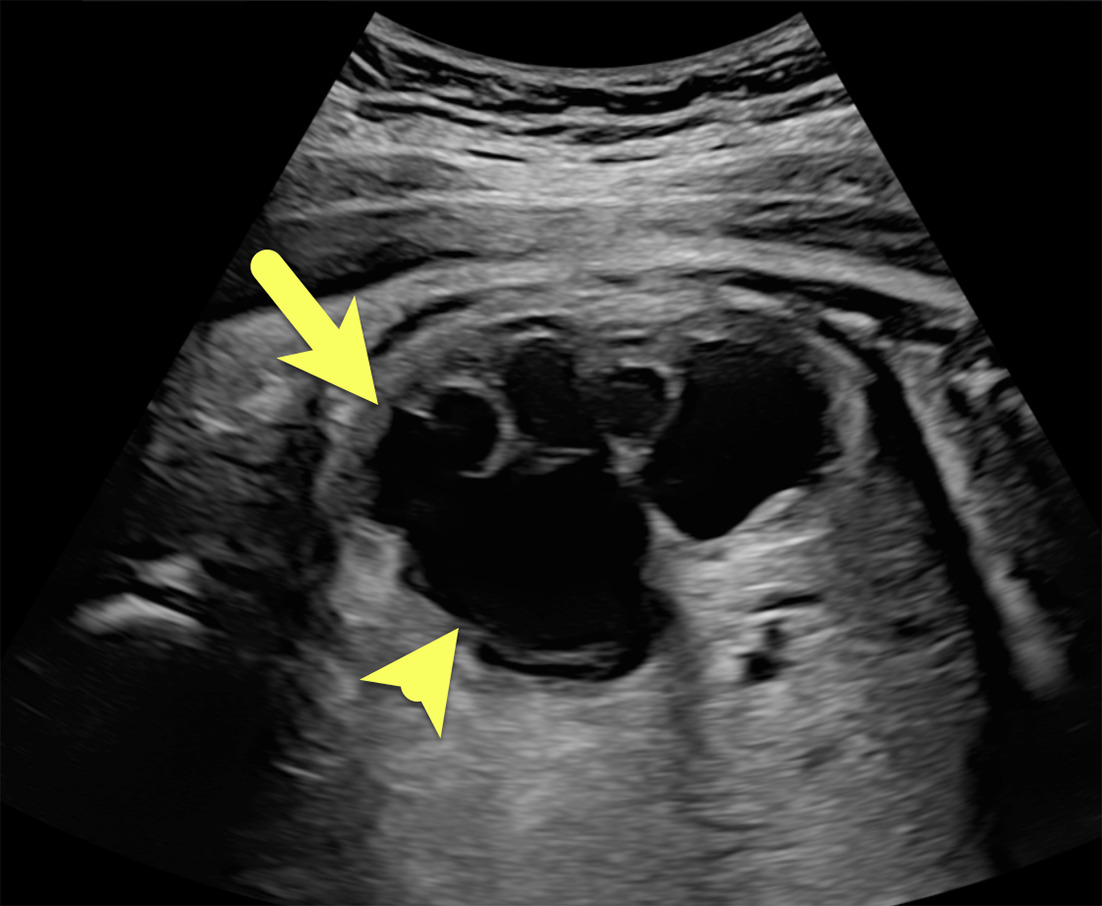
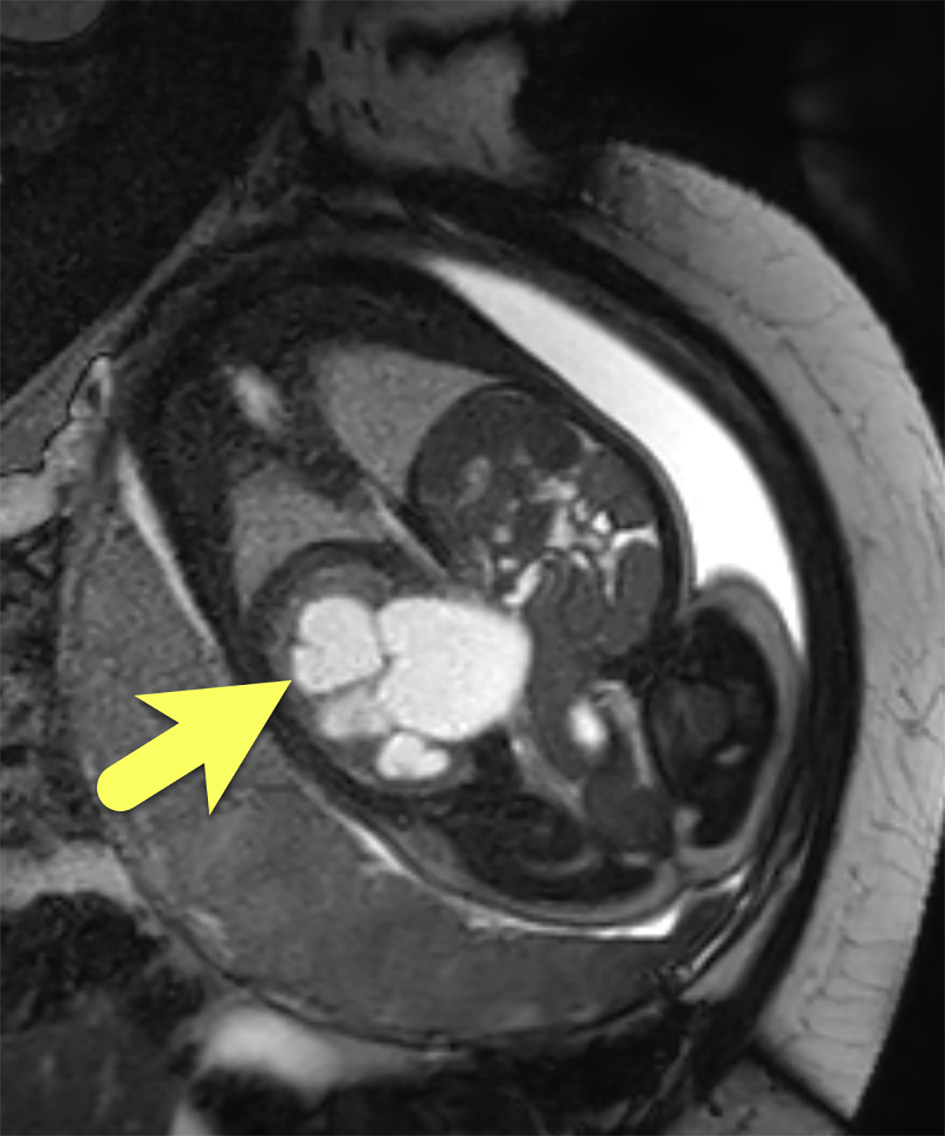
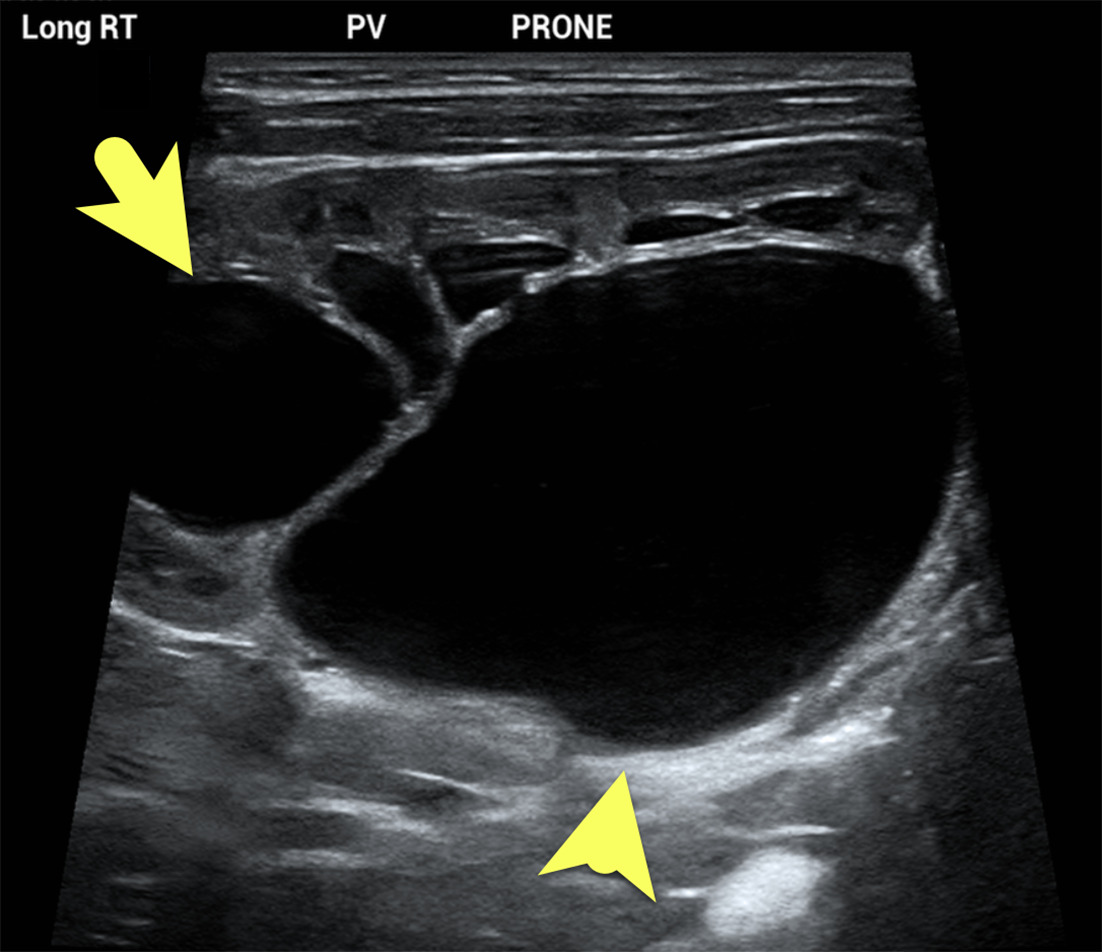
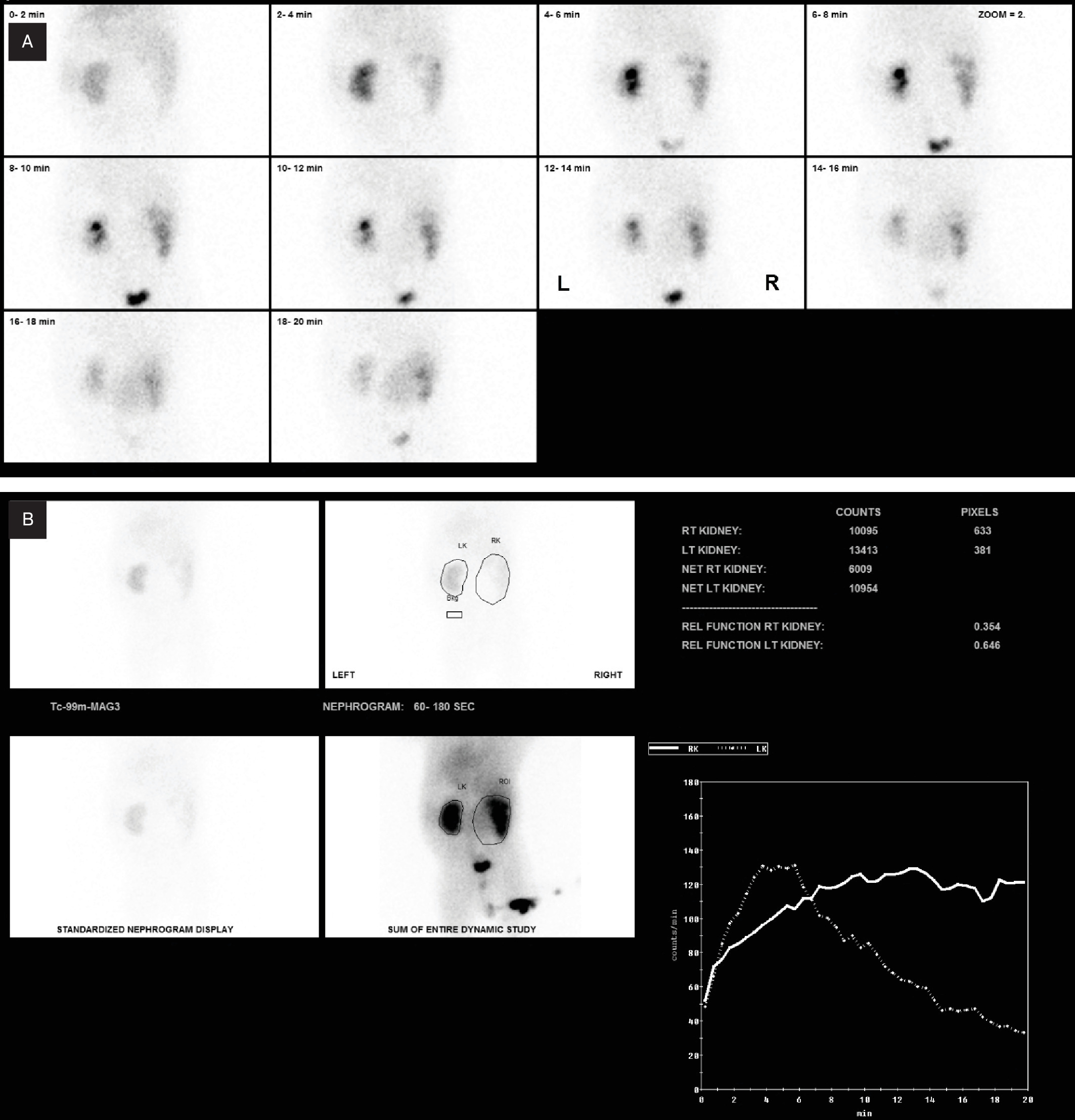
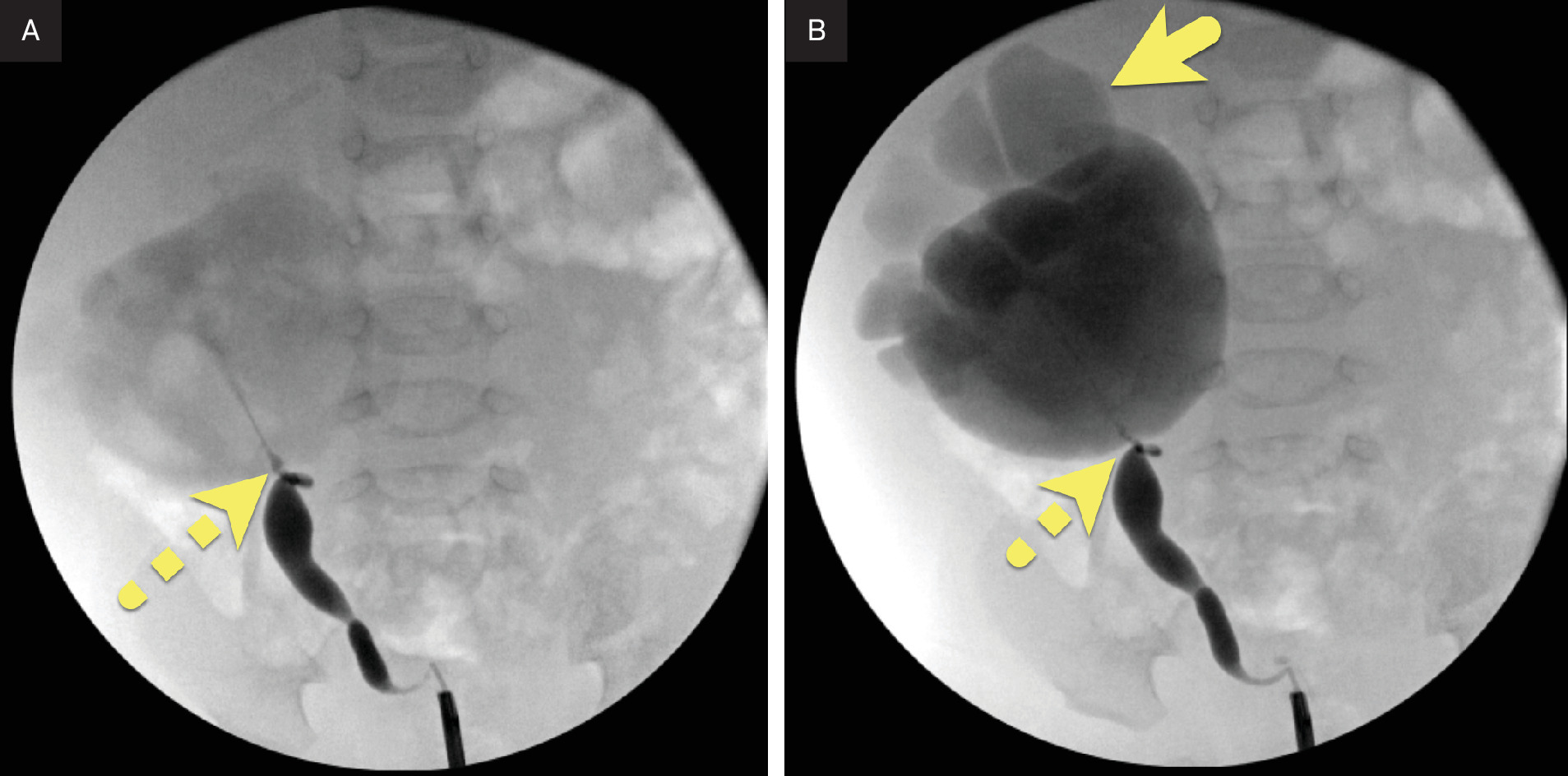
Prenatal US (Figure 1) and MRI (Figure 2) confirmed marked pelvocaliectasis of the right kidney. The right ureter was not visible. Postnatal US (Figure 3) showed similar findings. Tc-99m mercaptoacetyltriglycine (MAG) nuclear medicine study (Figure 4) confirms severe delay in the excretion of the radiopharmaceutical from the right kidney. Intraoperative ureteroscopy with contrast injection confirmed a right ureteropelvic junction (UPJ) obstruction (Figure 5).
Diagnosis
Fetal UPJ obstruction.
The differential diagnosis of isolated pelvocaliectasis includes intrinsic UPJ obstruction, extrarenal pelvis, parapelvic cyst, and vesicoureteral reflux.
Discussion
UPJ obstruction is the most common cause of congenital hydronephrosis and the most frequent obstructive uropathy in children. It occurs in approximately 1 in 1000 newborns, demonstrates a male predominance of roughly 3:1, and is typically unilateral, most often affecting the left kidney. 1,2 The disorder reflects impaired urine flow from the renal pelvis into the proximal ureter, most commonly due to intrinsic narrowing and less frequently from extrinsic compression at the UPJ. 3
Intrinsic obstruction most commonly results from abnormal smooth muscle development. Other distinct intrinsic causes include disorganized innervation or fibrosis at the UPJ. Regardless of mechanism, intrinsic obstruction leads to impaired peristalsis and urinary drainage. Extrinsic causes are less common and include aberrant crossing vessels, high ureteral insertion, or renal malrotation. 1
Most children with UPJ obstruction are first identified in utero during routine obstetric US, where antenatal urinary tract dilation is identified. 4 Postnatal evaluation then determines whether the dilation represents physiologic variation or true obstruction. When not diagnosed prenatally, presentation varies. In the neonatal period or later in childhood, patients may develop intermittent, crampy abdominal or flank pain accompanied by nausea and vomiting due to episodic dilation of the collecting system, a presentation referred to as Dietl’s crisis. 5
Postnatal diagnosis relies primarily on US, which demonstrates dilation of the renal pelvis and calyces without ureteral dilation. 6,7 Evaluation should be performed when the infant is well hydrated, with images obtained before and after voiding. The urinary tract dilatation (UTD) classification system provides a standardized framework for describing urinary tract dilation and stratifying its severity but does not establish a specific diagnosis. 8
Although US is well suited for evaluating the collecting system, it may not identify all causes of obstruction. When additional anatomic detail is required, CT and particularly MR urography allow more comprehensive evaluation, especially when extrinsic causes such as crossing vessels, ureteral kinking, or renal malrotation are suspected. Crossing vessels should be carefully assessed with Doppler US, CT, or MRI to identify a potential source of obstruction and assist in surgical planning. 9 Functional MR urography provides both quantitative functional assessment and high-resolution anatomy without radiation exposure but is generally reserved for complex cases and preoperative planning. 7,10
Renal function is most assessed with technetium Tc-99m MAG-3 diuretic renography, which evaluates drainage and differential renal function following administration of furosemide. The half-time of tracer clearance is measured, with values greater than 20 minutes typically indicating significant obstruction. 4,10 Although renal scintigraphy provides important functional information, it offers limited anatomic detail.
Management is individualized and depends on renal function, severity of dilation, symptoms, and underlying anatomy. Most children are managed conservatively with serial US and functional assessment, as many cases resolve spontaneously, although approximately 20% ultimately require intervention. Surgical pyeloplasty remains the gold standard and is indicated in patients with high-grade UTD, declining or reduced differential renal function, persistent or worsening symptoms, or recurrent infection. 11 The Anderson-Hynes dismembered pyeloplasty is the most performed technique and may be carried out via open, laparoscopic, or robotic approaches. The procedure involves excision of the narrowed UPJ segment and reanastomosis of the ureter to the renal pelvis. 11
Recurrent obstruction has been reported in up to 7% of cases and warrants close postoperative follow-up. 12 Long-term sequelae, including early-onset hypertension and proteinuria, should also be monitored, particularly in patients with bilateral disease. 11-13 Despite these potential complications, surgical outcomes are generally favorable, with high long-term success rates.
Conclusion
UPJ obstruction is the most common cause of congenital hydronephrosis and typically presents with dilation of the renal pelvis and calyces without associated ureteral dilation. Although many cases are suspected prenatally as urinary tract dilation, definitive evaluation occurs postnatally through integration of US findings and functional assessment.
US remains the primary imaging modality, with CT or MR urography used when additional anatomic detail is required, particularly to evaluate for extrinsic causes. Renal drainage and differential function are most commonly assessed with MAG-3 diuretic renography. Management is individualized based on symptoms, severity of dilation, and renal function. While many children are managed conservatively, surgical pyeloplasty is indicated in patients with significant obstruction or declining function and is associated with favorable long-term outcomes.
References
- Williams B, Tareen B, Resnick M. Pathophysiology and treatment of ureteropelvic junction obstruction. Curr Urol Rep. 2007;8(2):111-117. doi:10.1007/s11934-007-0059-8.
- Fwu C, Barthold J, Mendley S. Epidemiology of infantile ureteropelvic junction obstruction in the US. Urology. 2024;183:185-191. doi:10.1016/j.urology.2023.09.024.
- Tsai J, Huang F, Lin C. Intermittent hydronephrosis secondary to ureteropelvic junction obstruction: clinical and imaging features. Pediatrics. 2006;117(1):139-146. doi:10.1542/peds.2005-0583.
- Cai P, Lee R. Ureteropelvic junction obstruction/hydronephrosis. Urol Clin North Am. 2023;50(3):361-369. doi:10.1016/j.ucl.2023.04.001.
- Potenta S, D’Agostino R, Sternberg K, Tatsumi K, Perusse K. CT urography for evaluation of the ureter. Radiographics. 2015;35(3):709-726. doi:10.1148/rg.2015140209.
- Kleiner B, Callen P, Filly R. Sonographic analysis of the fetus with ureteropelvic junction obstruction. AJR Am J Roentgenol. 1987;148(2):359-363. doi:10.2214/ajr.148.2.359.
- Meshaka R, Biassoni L, Leung G, Mushtaq I, Hiorns M. Radiological and surgical correlation of pelviureteric junction obstruction in positional anomalies of the kidney in children. Pediatr Radiol. 2023;53(3):544-557. doi:10.1007/s00247-022-05557-7.
- Riccabona M, Lobo M, Ording-Muller L. European society of paediatric radiology abdominal imaging task force recommendations in paediatric uroradiology, part IX: imaging in anorectal and cloacal malformation, imaging in childhood ovarian torsion, and efforts in standardising paediatric uroradiology terminology. Pediatr Radiol. 2017;47(10):1369-1380. doi:10.1007/s00247-017-3837-6.
- Nguyen H, Phelps A, Coley B. 2021 update on the Urinary Tract Dilation (UTD) classification system: clarifications, review of the literature, and practical suggestions. Pediatr Radiol. 2022;52(4):740-751. doi:10.1007/s00247-021-05263-w.
- Houat A, Guimarães C, Takahashi M. Congenital anomalies of the upper urinary tract: a comprehensive review. Radiographics. 2021;41(2):462-486. doi:10.1148/rg.2021200078.
- Szavay P, Zundel S. Surgery of uretero-pelvic junction obstruction (UPJO). Semin Pediatr Surg. 2021;30(4). doi:10.1016/j.sempedsurg.2021.151083.
- Chen R, Jiang C, Li X. Analysis of risk factors for stenosis after laparoscopic pyeloplasty in the treatment of ureteropelvic junction obstruction. Int Urol Nephrol. 2024;56(6):1911-1918. doi:10.1007/s11255-023-03906-5.
- Zouari M, Dghaies R, Rhaiem W. Risk factors for adverse outcomes after pediatric pyeloplasty: a retrospective cohort study. Int J Urol. 2024;31(1):45-50. doi:10.1111/iju.15305.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Fetal Ureteropelvic Junction Obstruction. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0077.