Fibrosing Mediastinitis
Journal of Pediatric Case Reports — Vol. 1 , Issue 2
Published: April 1, 2026
1 University of Tennessee, Knoxville, Tennessee
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Heart Institute, Le Bonheur Children’s Hospital, Memphis, Tennessee
4 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Fibrosing mediastinitis (FM) is a potentially destructive disease that affects mostly young patients who present with signs and symptoms related to obstructed mediastinal structures. Most granulomatous FM cases are unilateral and caused by histoplasmosis infection. Nongranulomatous FM is more diffuse and has varying causes but is thankfully rare. CT and MRI are key in the diagnosis and management of FM, vital to assessing the extent of mediastinal involvement, and essential for guiding either surgical or transcatheter therapy.
Keywords
thorax, mediastinum, infection
Categories
Case Summary
An a dolescent male presented with chest pain and mild shortness of breath with activity. Physical exam showed normal vital signs, normal heart sounds, and breath sounds were clear to auscultation bilaterally.
Imaging Findings
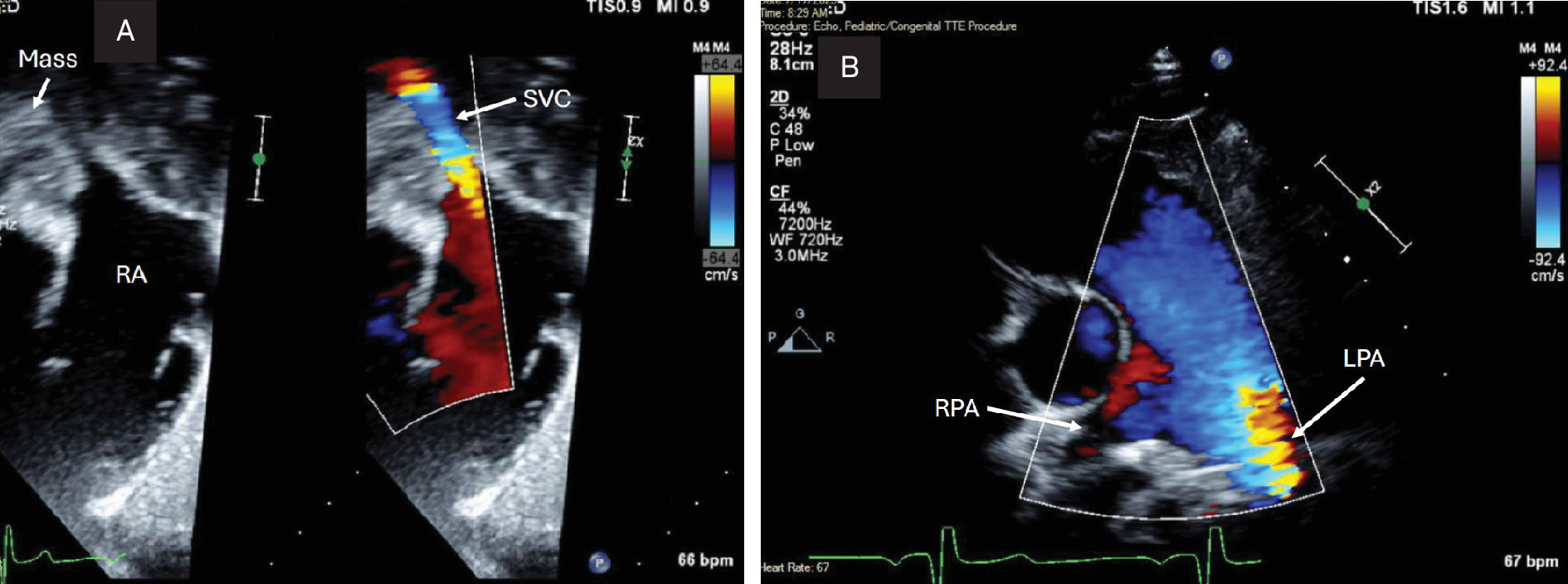
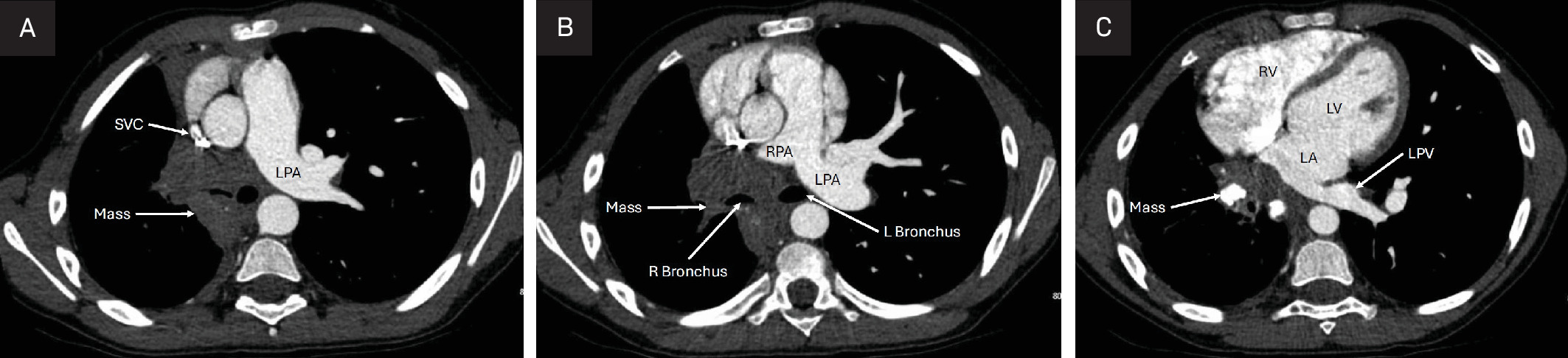
Chest x-ray (Figure 1) showed right basilar atelectasis, trace right pleural effusion, and right middle lobe volume loss. Transthoracic echocardiogram (Figure 2) showed external compression of the proximal superior vena cava, right pulmonary artery, and right pulmonary veins from a mediastinal mass. Chest CTA (Figure 3) showed a partially calcified conglomerate right hilar mass causing near occlusion of the right pulmonary artery, right pulmonary veins, right mainstem bronchus, bronchus intermedius, right middle -lobe bronchus, and right lower lobe bronchus.

Diagnosis
Fibrosing m ediastinitis (FM) , granulomatous form from histoplasmosis infection.
The differential diagnosis of FM is other infections causing granulomas like tuberculosis, mycobacterial infections, and other fungal infections (aspergillosis and coccidioidomycosis). Most cases of granulomatous FM are unilateral and caused by h istoplasmosis. Nongranulomatous causes of FM include sarcoidosis, autoimmune diseases (rheumatoid arthritis and lupus), radiation therapy, medications, and idiopathic conditions. Malignancies (lymphoma, thymoma, lung cancer, and metastatic cancers), amyloidosis, lymphangiomatosis, and granulomatosis with polyangiitis are also important differentials to consider.
Discussion
FM or sclerosing mediastinitis is a rare disorder consisting of inflamed fibrous tissues within the mediastinum. Within the mediastinum are the heart, blood vessels, trachea, esophagus, lymph nodes, and the thymus. 1 These structures can all be subject to compression by the invasive fibrous tissues, resulting in pain and discomfort for patients diagnosed with this disorder. FM occurs in regions where fungal antigens have been seen to be associated with a fibrosing response within the body’s immune system. 2 This response can be the result of the fungus Histoplasma capsulatum spreading within the mediastinum forming granulomas and is typically the most common cause in the United States. 3 The exact prevalence of FM is unknown as it typically occurs in regions where fungal infections are endemic, but not all patients experience the severity of FM. 4 Clinical cases of histoplasmosis infections mostly appear benign, with progression to FM rare.
Not all cases of FM are related to histoplasmosis. Other infections like tuberculosis and other fungal infections (aspergillosis and mucormycosis) can cause FM. 5 FM has also been reported in the setting of autoimmune diseases, rheumatic fever, radiation therapy, cancers, and certain drug therapy. 6 Patients with FM exhibit various symptoms , including pleuritic chest pain, cough, dyspnea, and hemoptysis commonly, and fever, tachycardia, and weight loss rarely. FM typically involves individuals from 20 to 40 years old but has been described in children to older adults as well and affects men and women equally. Radiologic findings exhibit signs of mediastinal widening, hilar mass, and calcifications. 6
The appearance of FM on CT is variable depending upon the pattern of involvement. In the granulomatous or localized disease, there are mediastinal or hilar masses often with calcium deposition. Calcium deposition is common in FM associated with histoplasmosis infections. CT also clearly shows the airways and vascular structures that are affected by the hilar mass. 7 In the nongranulomatous or diffuse type, there is soft-tissue obliteration of normal fat planes that encases or invades surrounding structures. FM is seen by MRI as a heterogeneous, infiltrative mass of variable signal intensity on T1- and T2-weighted MR images. The areas of decreased signal intensity represent calcium deposits , and increased signal intensity represents inflammation. 6 Partially calcified hilar masses that do not cause external compression of surrounding structures are routinely seen on CT and MRI studies in endemic regions and do not result in FM. These patients usually never develop FM and are just observed.
Overall, mortality of FM tends to be low, depending on the affected structures in the mediastinum. 4 Severe forms of FM can result in pulmonary hypertension and right heart failure that leads to higher mortality rates. 2 Mediastinal granulomas typically are benign but do result in a worse prognosis when lesions compress neighboring structures. 2 A mortality rate as high as 3 0% has been reported, but this likely reflects the more severe cases of FM with bilateral involvement and not localized hilar masses that are more common. 8
Treatment of FM varies depending upon the presentation and severity of the disease. Treatment can range from observation to medical therapy with antifungals and steroids to procedural options (surgical debulking or stenting/balloon dilation of affected vessels). 4 As most cases of FM are related to histoplasmosis infection, antifungal therapy (ketoconazole) is often used first line with varying success. 9 Most cases of FM present well after active histoplasmosis infection and resultant inflammation has resolved, so steroid treatment has varying success as well. 1 Surgical debulking can be effective in unilateral disease but with varying success. 1,9,10 Currently, balloon dilation and/or stent angioplasty of affected vessels is utilized more than surgical debulking as a less invasive option. 1 The severity of external compression and ability to successfully re-cannulate affected vessels determines the decision to proceed with invasive options.
Conclusion
FM is a potentially destructive disease that affects mostly young patients who present with signs and symptoms related to obstructed mediastinal structures. Most cases of granulomatous FM are unilateral and caused by histoplasmosis infection. Nongranulomatous FM is more diffuse and has varying causes but is thankfully rare. CT and MRI are key in the diagnosis and management of FM, vital to assessing the extent of mediastinal involvement, and essential for guiding either surgical or transcatheter therapy.
References
- Lin J, Jimenez C. Acute mediastinitis, mediastinal granuloma, and chronic fibrosing mediastinitis: a review. Semin Diagn Pathol. 2022;39(2):113-119. doi:10.1053/j.semdp.2021.06.008.
- Peikert T, Colby T, Midthun D. Fibrosing mediastinitis: clinical presentation, therapeutic outcomes, and adaptive immune response. Medicine. 2011;90(6):412-423. doi:10.1097/MD.0b013e318237c8e6.
- Jain N, Chauhan U, Puri S, Agrawal S, Garg L. Fibrosing mediastinitis: when to suspect and how to evaluate?. BJR Case Rep. 2016;2(1). doi:10.1259/bjrcr.20150274.
- McNeeley M, Chung J, Bhalla S, Godwin J. Imaging of granulomatous fibrosing mediastinitis. AJR Am J Roentgenol. 2012;199(2):319-327. doi:10.2214/AJR.11.7319.
- Lee J, Kim Y, Lee K, Chung M. Tuberculous fibrosing mediastinitis: radiologic findings. AJR Am J Roentgenol. 1996;167(6):1598-1599. doi:10.2214/ajr.167.6.8956619.
- Rossi S, McAdams H, Rosado-de-Christenson M, Franks T, Galvin J. Fibrosing mediastinitis. Radiographics. 2001;21(3):737-757. doi:10.1148/radiographics.21.3.g01ma17737.
- Garin A, Chassagnon G, Tual A, Revel M. CT features of fibrosing mediastinitis. Diagn Interv Imaging. 2021;102(12):759-762. doi:10.1016/j.diii.2021.05.013.
- Loyd J, Tillman B, Atkinson J, Des Prez R. Mediastinal fibrosis complicating histoplasmosis. Medicine. 1988;67(5):295-310. doi:10.1097/00005792-198809000-00002.
- Urschel H, Razzuk M, Netto G, Disiere J, Chung S. Sclerosing mediastinitis: improved management with histoplasmosis titer and ketoconazole. Ann Thorac Surg. 1990;50(2):215-221. doi:10.1016/0003-4975(90)90737-q.
- Dunn E, Ulicny K, Wright C, Gottesman L. Surgical implications of sclerosing mediastinitis. a report of six cases and review of the literature. Chest. 1990;97(2):338-346. doi:10.1378/chest.97.2.338.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Fibrosing Mediastinitis. Journal of Pediatric Case Reports. 2026;1(2). doi:10.37549/JPCR-26-0087.