Fontan-Associated Liver Disease
Applied Radiology
Published: November 1, 2025
1 Creighton University School of Medicine, Omaha, Nebraska
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Cincinnati Children’s Hospital Medical Center and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Fontan-associated liver disease (FALD) is a ubiquitous complication in patients with Fontan physiology. Optimal monitoring of FALD development typically starts with imaging. Liver stiffness values can help guide therapy and can act as a surrogate for disease severity. When nodules are present, they can be challenging. Looking for a lesion that behaves differently than other lesions is the best way to identify hepatocellular carcinoma.
Keywords
Abdomen, Liver, Vascular
Categories
Case Summary
A teenage male with a history of hypoplastic left heart syndrome and staged surgical repair, including Fontan procedure with subsequent closure of the Fontan fenestration to improve his resting oxygen saturation, underwent routine imaging surveillance for Fontan-associated liver disease (FALD). Two years prior, the liver MRI demonstrated findings concerning for advanced FALD (stage 3-4) fibrosis. Presently he is feeling well and has increased energy; however, he has low exercise capacity. Additionally, he is receiving growth hormone for growth delay and short stature.
Imaging Findings
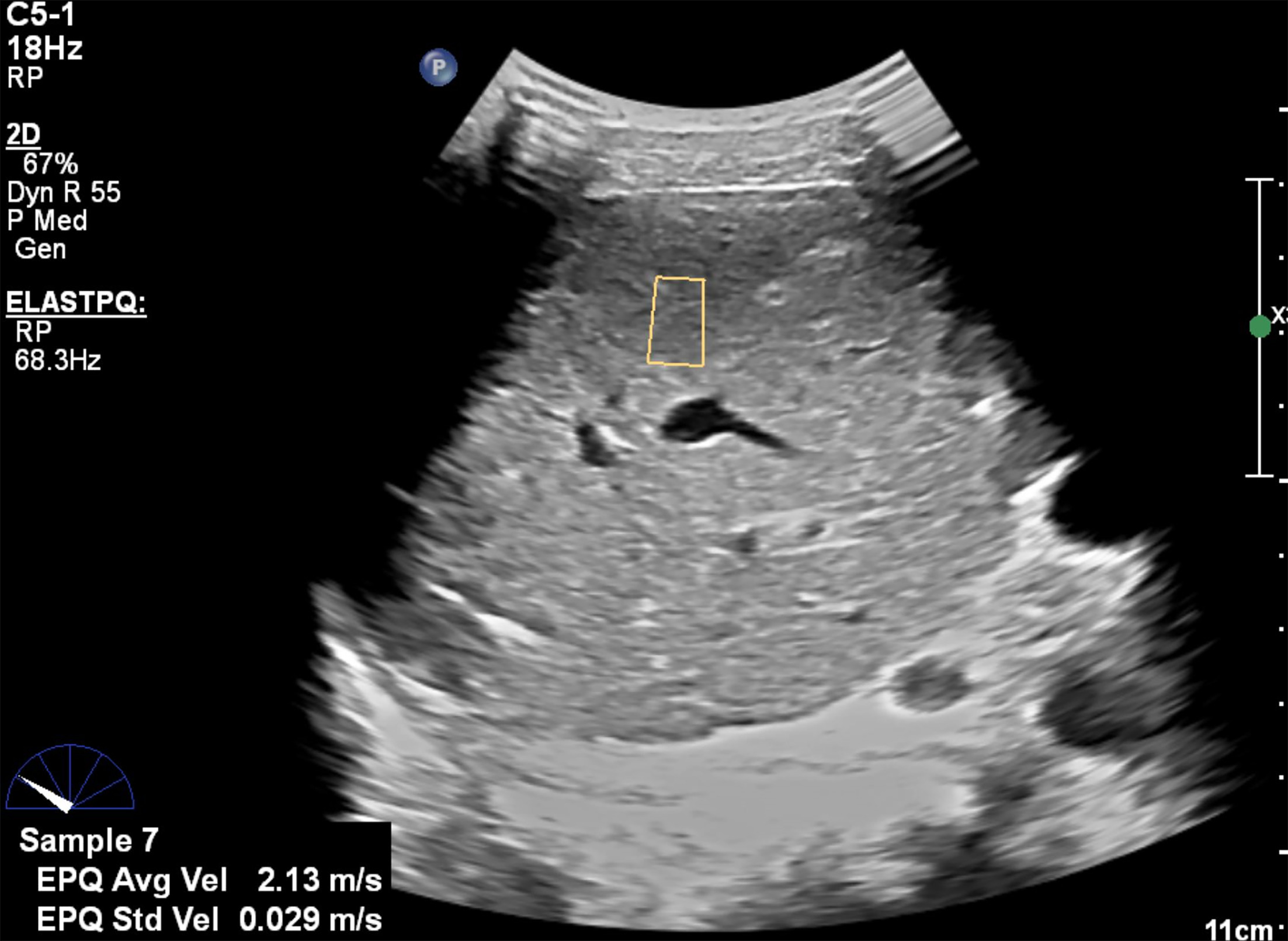
US of the liver with elastography (Figure 1) demonstrated heterogeneous echotexture and a shear wave elastography Elast-PQ average velocity of 2.15 m/second in the right lobe, categorized as advanced fibrosis/cirrhosis suspected. Focal hepatic lesions were not identified.
An MRI of the abdomen with and without Eovist intravenous contrast and MR elastography was performed (Figure 2). There is diffuse hepatic heterogeneous signal intensity on T2-weighted images and heterogeneous enhancement. Additionally, innumerable sub-centimeter parenchymal nodules with enhancement greater than the background liver on the hepatobiliary phase imaging were present out to 30 minutes following contrast administration, which suggests focal nodular hyperplasia (FNH)-like lesions. The mean shear stiffness value for the liver was calculated at 5.2 kPa (stage 4 or cirrhosis). There is no contrast washout in the lesions during the portal phase nor delayed phases of imaging to suggest hepatocellular carcinoma (HCC).
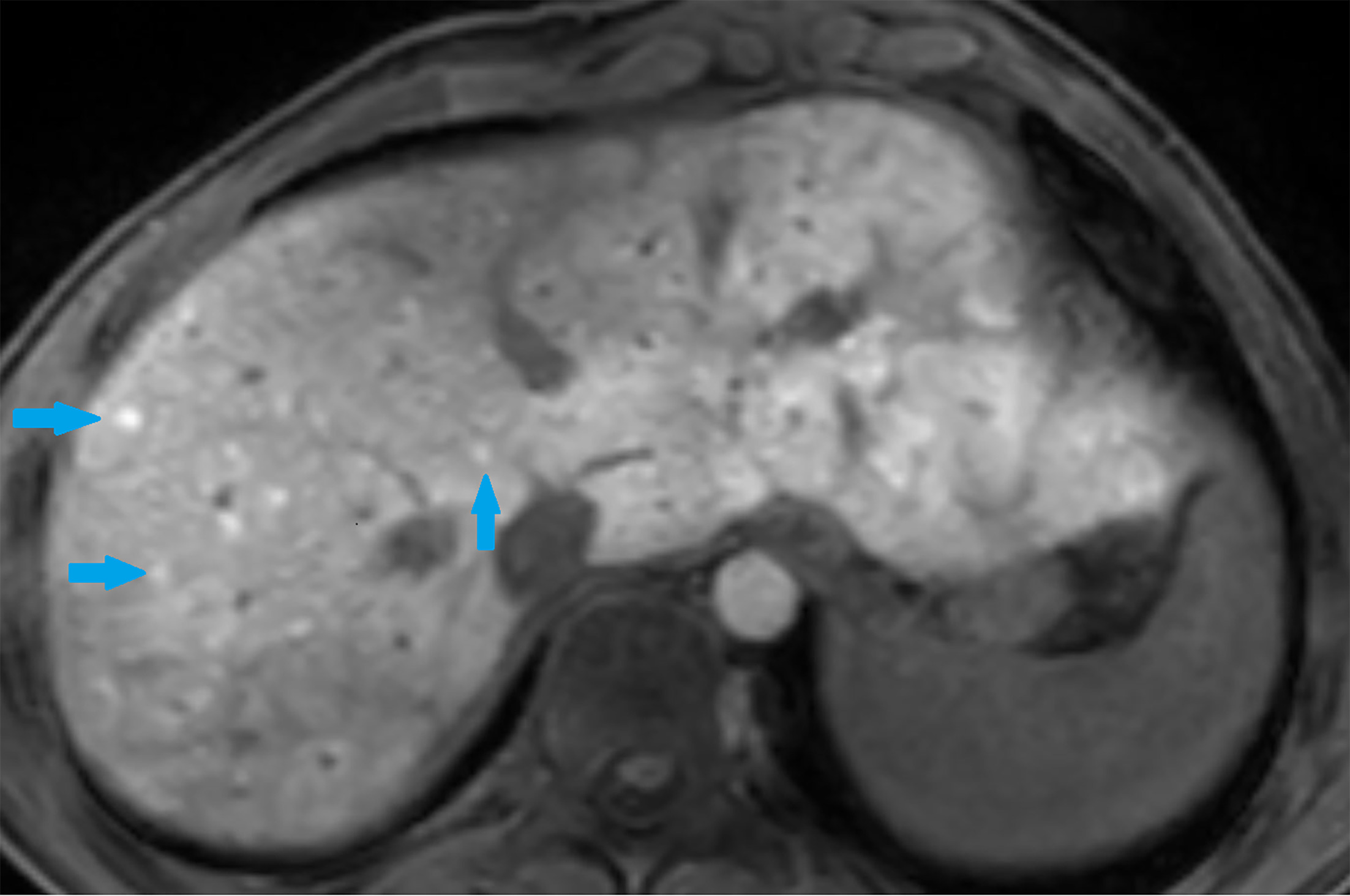
Because of imaging findings of progressive hepatic fibrosis following closure of the Fontan fenestration, repeat hemodynamic assessment of the Fontan pressure was requested, as well as a liver biopsy (Figure 2).
In the early stages of FALD, abdominal US may reveal a normal or slightly hypoechoic hepatic parenchyma. As fibrosis progresses, a coarse heterogeneous hyperechoic parenchyma with a nodular surface is observed, and caudate lobe hypertrophy may also be seen.
Diagnosis
FALD
Discussion
The Fontan procedure is an operation that shunts blood from the systemic venous system to the lungs without first traveling through a ventricle. Multiple iterations of the procedure exist. However, the original procedure involves an anastomosis of the right atrium to the pulmonary artery. It can be performed for multiple different types of congenital heart diseases with a single-ventricle physiology. 1,2 Due to increased long-term survival, the number of patients living with a Fontan circulation continues to grow. In 2018, it was estimated that there were 50,000-70,000 patients living with a Fontan physiology. 3
Long-term survival of patients with Fontan circulation has translated to increased complications. The Fontan procedure alters native circulation by increasing central venous pressure and decreasing cardiac output. This causes numerous downstream consequences. Over time, the elevated central venous pressures, which are similar in physiology to hepatic venous outflow obstruction, result in arterialization of hepatic blood flow, leading to increased liver stiffness. 4 These impeded hepatic flow dynamics result in a spectrum of structural and functional liver alterations, known collectively as FALD. This spectrum of congestive hepatopathy can lead to liver fibrosis, cirrhosis, and liver lesions including HCC.
FALD occurs in virtually 100% of patients after a Fontan procedure, with the severity of liver disease increasing with age and the time since the operation. 5 Algorithms have been proposed to screen for advanced liver disease. However, there are no data related to the efficacy of these algorithms and their impact on patient outcomes or detection of HCC. 6,7 ,
US or MR elastography is performed to assess liver stiffness. The stiffness value helps provide an estimate of the severity of liver congestion and fibrosis. While the stiffness value cannot distinguish congestion and fibrosis, the anatomic findings can help provide context. On US, hepatic fibrosis can appear as coarsened hepatic echotexture. In more advanced diseases, the liver can have a nodular contour, and multiple nodules may be present. On MRI, fibrosis appears with wispy T1 hypointense/T2 hyperintense signal, most notable at the liver periphery. As the fibrosis progresses, the abnormal signal becomes thicker and distributed throughout the liver. Nodules may be present throughout the liver. These nodules are variable in signal depending on their etiology. Potential types of nodules include regenerative nodules (RNs), dysplastic nodules (DN), FNH-like lesions, hepatocellular adenomas (HAs), and HCC. RNs are caused by chronic elevation of central venous pressure and consequent passive hepatic congestion. This leads to reduced blood flow to areas of the liver, especially the centrilobular zones, and reduced oxygen delivery to hepatocytes, resulting in reactive fibrogenesis and scarring. The liver compensates for damaged tissue by forming hyperplastic nodules of liver cells. RNs appear as multiple round, sharply defined nodules throughout the liver. On post-contrast CT and MRI, the nodules enhance like normal liver in portal venous and delayed phases. 8 Arterial phase enhancement is usually absent or minimal and increases with the degree of dysplastic transformation. 8 DNs are RD usually > 1 cm, with atypical cells and histologic disorganization and are considered pre-malignant lesions of HCC. FNH-like lesions are histologically the same as FNH but associated with an abnormal liver. FNH is a benign liver tumor characterized by a proliferation of normal hepatocytes that are disorganized around a central scar. HAs are benign tumors and are histologically distinct nodules of mature hepatocytes and lack portal tracts and unpaired arteries. HAs are usually associated with the use of oral contraceptives, and they can also be found in patients with FALD. The imaging features include a variable appearance but are usually hyperintense compared with the liver on T1 and T2 sequences because of increased fat content. 8 The risk of HCC is increased in patients with cirrhosis, with the incidence estimated to be 1.5-5% per year and has a mortality rate of about 30%. The 30-year cumulative incidence of HCC after a Fontan operation is about 7%.
Because HCC is in the differential diagnosis for hepatic nodules, it is crucial to try to differentiate it from other lesions. Unfortunately, there are no reliable criteria to make the diagnosis. In adult patients, the Liver Imaging Reporting and Data System (LI-RADS) criteria are used to help identify lesions concerning for HCC. However, the LIRADS criteria do not apply to patients with cardiac disease or children. Prior studies in children have shown that the LIRADS criteria are neither sensitive nor specific for distinguishing HCC from other lesions. 9 The best way to identify lesions at risk for HCC is to look for lesions that differ from the others. Key findings include a lesion within a lesion, lesional washout of contrast on the delayed venous phase, and lack of retained contrast on the hepatobiliary phase of imaging. 10,11
Conclusion
FALD is a ubiquitous complication in patients with Fontan physiology. Optimal monitoring of FALD development typically starts with imaging. Liver stiffness values can help guide therapy and can act as a surrogate for disease severity. When nodules are present, they can be challenging. Looking for a lesion that behaves differently than other lesions is the best way to identify HCC.
References
- Fredenburg T, Johnson T, Cohen M. The Fontan procedure: anatomy, complications, and manifestations of failure. Radiographics. 2011;31(2):453-463. doi:10.1148/rg.312105027.
- Chavhan G, Yoo S, Lam C, Khanna G. Abdominal imaging of children and young adults with fontan circulation: pathophysiology and surveillance. AJR Am J Roentgenol. 2021;217(1):207-217. doi:10.2214/AJR.20.23404.
- Schilling C, Dalziel K, Nunn R. The Fontan epidemic: population projections from the Australia and New Zealand Fontan registry. Int J Cardiol. 2016;219:14-19. doi:10.1016/j.ijcard.2016.05.035.
- Rychik J, Atz A, Celermajer D. Evaluation and management of the child and adult with Fontan circulation: a scientific statement from the American Heart Association. Circulation. 2019;140(6). doi:10.1161/CIR.0000000000000696.
- Goldberg D, Surrey L, Glatz A. Hepatic fibrosis is universal following Fontan operation, and severity is associated with time from surgery: a liver biopsy and hemodynamic study. J Am Heart Assoc. 2017;6(5). doi:10.1161/JAHA.116.004809.
- Emamaullee J, Zaidi A, Schiano T. Fontan-associated liver disease. Circulation. 2020;142(6):591-604. doi:10.1161/CIRCULATIONAHA.120.045597.
- Agnoletti G, Ferraro G, Bordese R. Fontan circulation causes early, severe liver damage. Should we offer patients a tailored strategy?. Int J Cardiol. 2016;209:60-65. doi:10.1016/j.ijcard.2016.02.041.
- Zafar F, Lubert A, Trout A. Abdominal CT and MRI findings of portal hypertension in children and adults with fontan circulation. Radiology. 2022;303(3):557-565. doi:10.1148/radiol.211037.
- Khanna G, Chavhan G, Schooler G. Diagnostic performance of LI-RADS version 2018 for evaluation of pediatric hepatocellular carcinoma. Radiology. 2021;299(1):190-199. doi:10.1148/radiol.2021203559.
- Silva-Sepulveda J, Fonseca Y, Vodkin I. Evaluation of Fontan liver disease: correlation of transjugular liver biopsy with magnetic resonance and hemodynamics. Congenit Heart Dis. 2019;14(4):600-608. doi:10.1111/chd.12770.
- Borquez A, Silva-Sepulveda J, Lee J. Transjugular liver biopsy for Fontan associated liver disease surveillance: technique, outcomes and hemodynamic correlation. Int J Cardiol. 2021;328:83-88. doi:10.1016/j.ijcard.2020.11.037.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Fontan-Associated Liver Disease. Applied Radiology. 2025. doi:10.37549/JPCR-25-0027.