1 Burell College of Osteopathic Medicine, Las Cruces, New Mexico
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
An external protrusion of the intestines and occasionally other organs without a protective membrane is the hallmark of gastroschisis. Prenatal US, specifically the marker Intraabdominal bowel distention, is the most effective in diagnosing and differentiating between simple and complex gastroschisis. Patients diagnosed with the condition are at a risk of infection, sepsis, and electrolyte imbalances from swelling and inflammation of the exposed organs. Treatment aims for primary reduction of the herniated viscera to prevent visceral injury and abdominal compartment syndrome. Staged reduction using a spring-loaded silo is the preferred method. Complex cases should be treated individually, and any resection should be kept to a minimum to prevent short-gut syndrome.
Keywords
gastrointestinal, congenital, intestine
Categories
Case Summary
A mother with a history of cocaine use during pregnancy underwent detailed fetal US due to findings on screening US. The fetus was born at term via cesarean section and transferred to the neonatal intensive care unit.
Imaging Findings
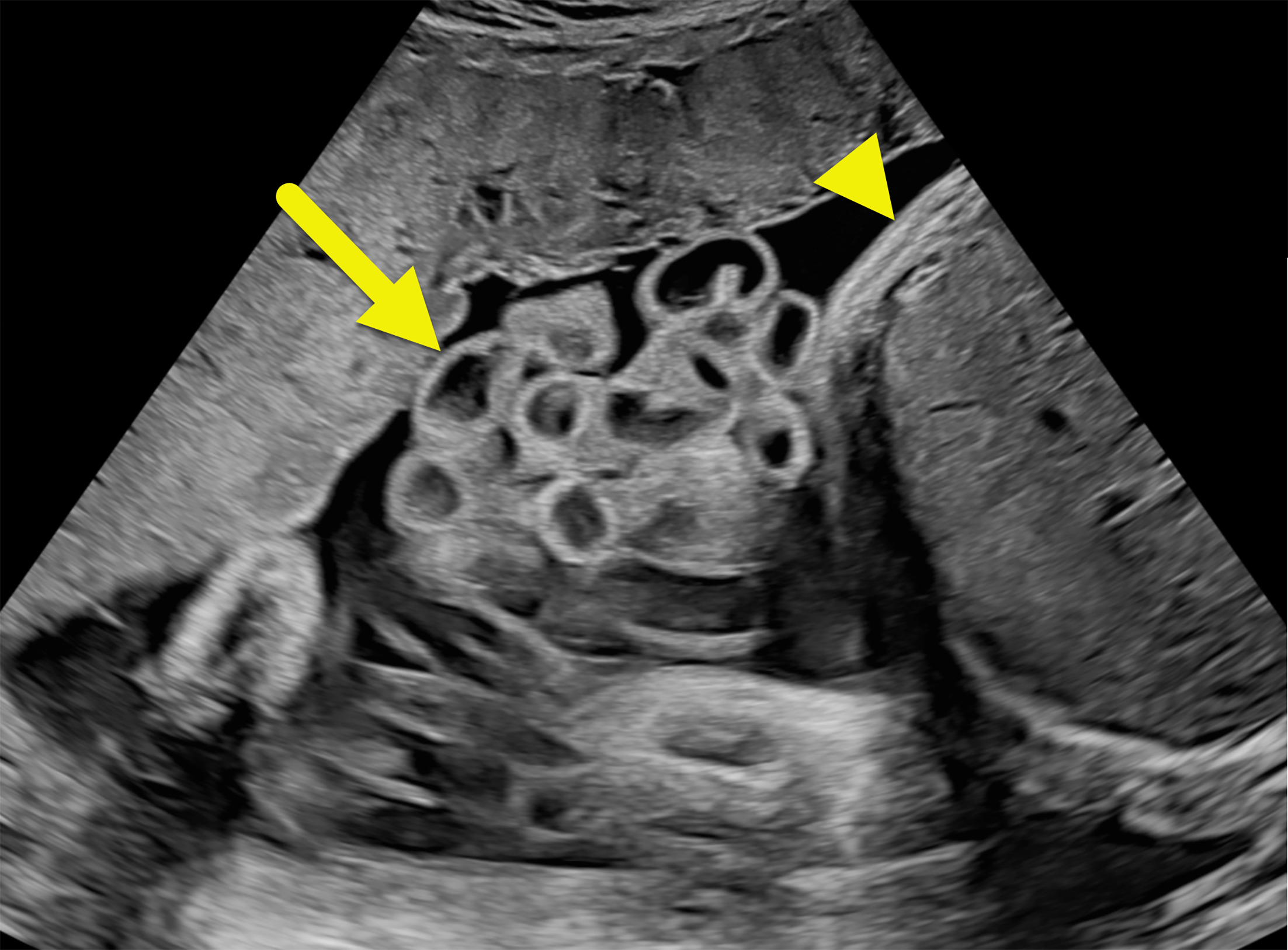
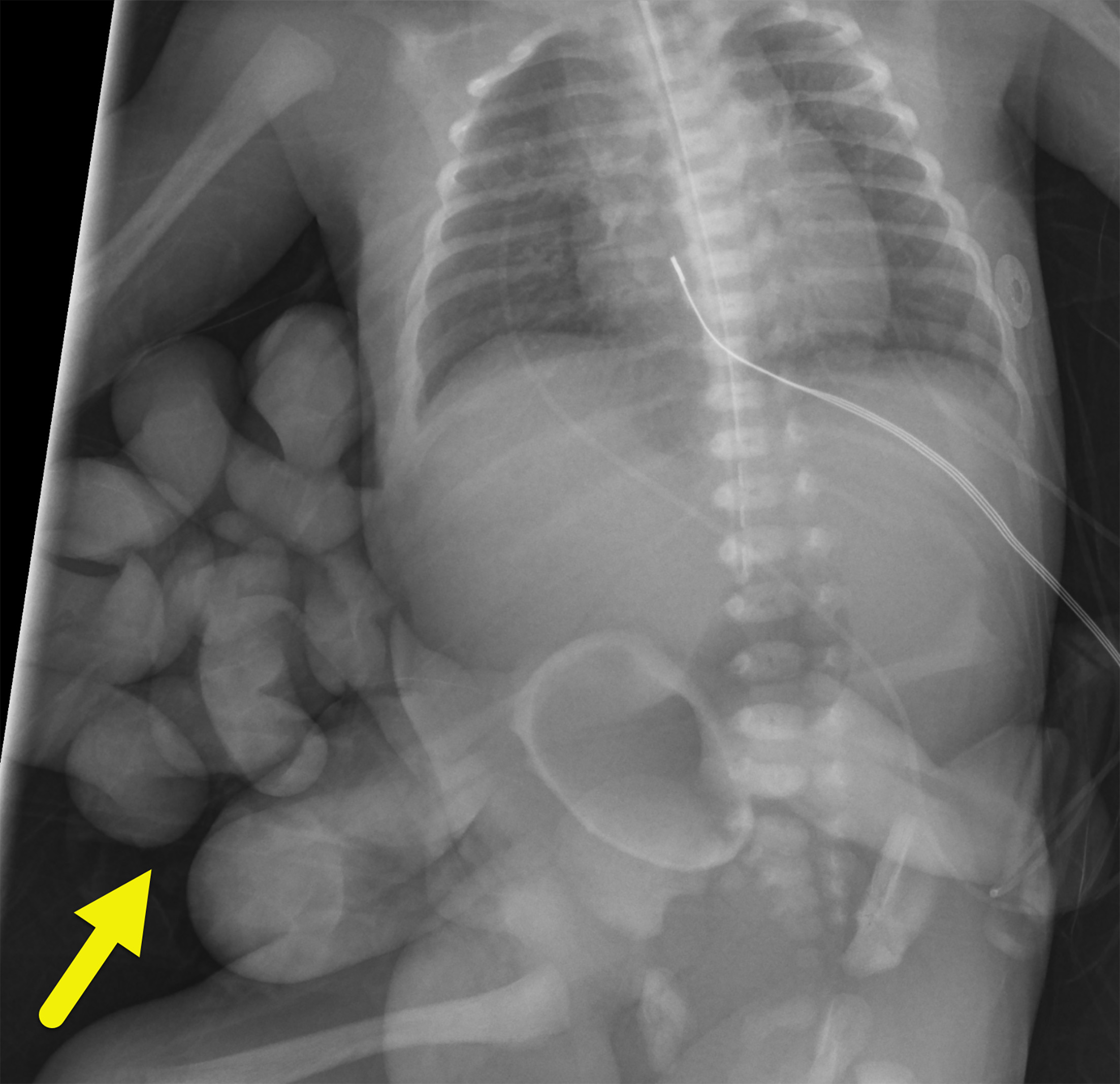
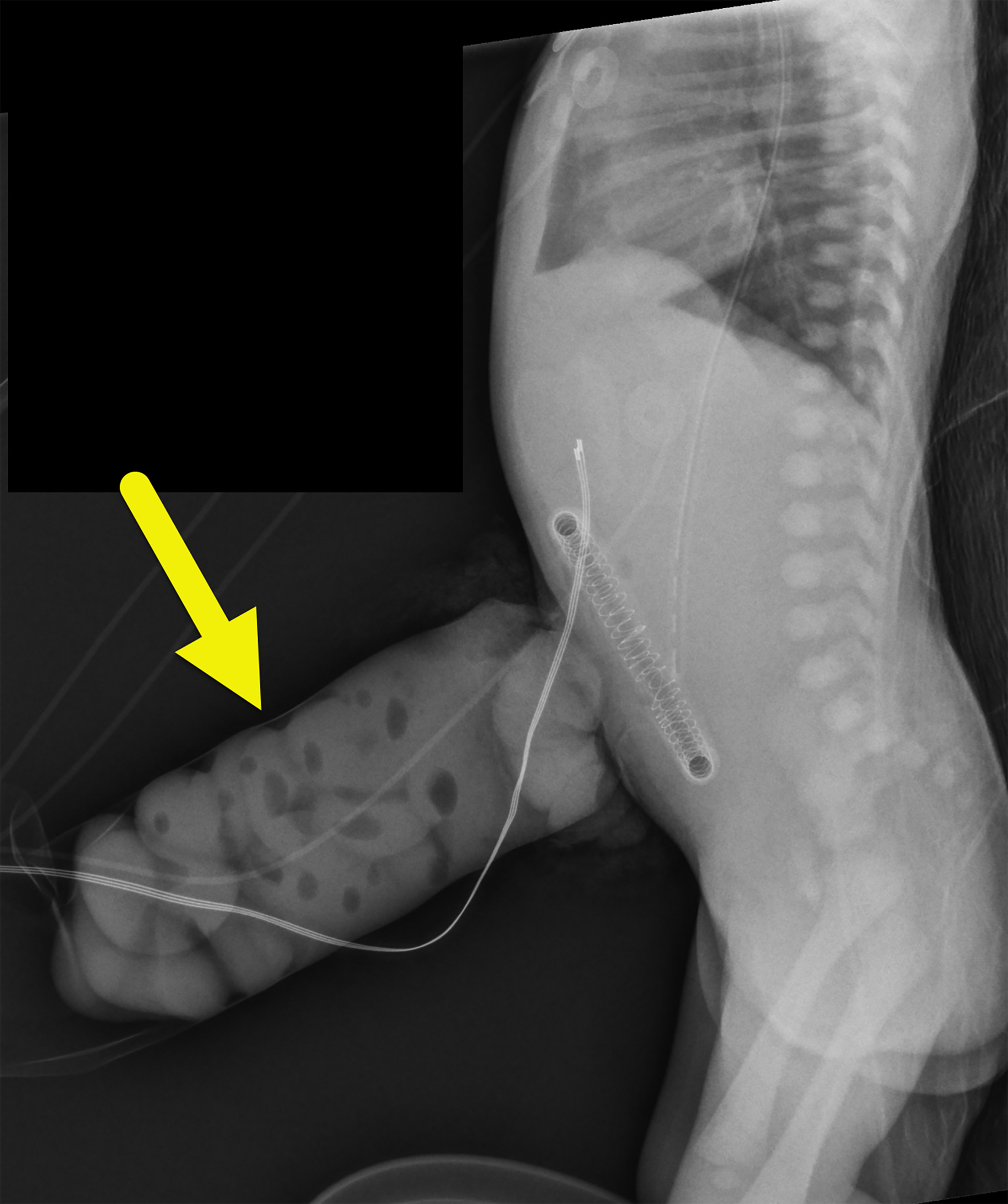
Fetal US (Figure 1) showed gastroschisis with dilated loops of bowel with thickened walls extending through a midline abdominal wall defect adjacent to the umbilical cord. Postnatal radiograph (Figure 2) showed eviscerated bowel loops external to the abdomen. A radiograph performed 2 hours later (Figure 3) showed the loops of bowel within an abdominal silo.
Diagnosis
Gastroschisis.
The differential diagnosis for an anterior abdominal wall defect with protrusion of organs outside of the fetus is an omphalocele.
Discussion
Gastroschisis is a full-thickness, congenital defect involving the anterior abdominal wall that occurs in utero. The cause of gastroschisis is currently unknown. The uncovered viscera herniates through the abdominal wall defect near the base of the umbilical cord. Typically, gastroschisis is diagnosed on fetal ultrasonography at 20 weeks of gestational age. 1 Depending on the state of the colon, there are 2 types of gastroschisis: simple and complex. The bowel is healthy in simple gastroschisis. In contrast, complex gastroschisis is associated with conditions such as volvulus, ischemia, atresia, or necrosis. 2
Although gastroschisis and omphalocele are both abdominal wall defects, their presentation has characteristic differences. Gastroschisis is an abdominal wall defect, most often to the right of the umbilicus. It is usually a solitary anomaly with postdelivery outcomes related to the prolapsed bowel. The prolapsed bowel lacks a covering membranous sac, and the intestines protrude outside the fetal abdomen into the amniotic cavity because of an in utero interruption of the lateral ventral body folds that occur between the 4-8 weeks of gestation. 3 While gastroschisis is not associated with other congenital anomalies, it is commonly associated with bowel complications, which include intestinal atresia or stenosis (10% of cases) or malrotation, that further complicates the condition. 2
Omphalocele is an abdominal wall defect that differs from gastroschisis due to its midline location and sac covering the herniated intestines. The abdominal wall defect in omphaloceles can vary in size. When small, only a portion of the intestines may herniate. When a large abdominal wall defect occurs, most abdominal organs can herniate. Omphaloceles are associated with genetic syndromes such as trisomy 13 and 18, and anomalies that will determine the patient’s outcome. Multiple congenital abnormalities are present in 40-80% of patients and include chromosomal (15-57%), cardiac (11-23%), genitourinary (6-21%), musculoskeletal (21%), gastrointestinal (7-19%), and neurologic (4-8%) issues. 3 The survival rate for patients with isolated omphalocele is 90% and decreases depending upon the type, number, and severity of associated anomalies.
Fetal growth restriction occurs in 24-67% of fetuses with gastroschisis and is thought to be due to the nonselective loss of nutrients, mainly proteins, through the externalized bowel loops, causing chronic undernutrition of the fetus. This is supported by the fact that high levels of proteins are found in the amniotic fluid. In a recent meta-analysis, delivery at 38 weeks was found to minimize overall perinatal mortality and maximize total quality-adjusted life-years in fetuses with gastroschisis. Cesarean section was once thought by some to be the best delivery route for the fetus with gastroschisis because it reduced the risk of trauma to intestinal loops and avoided contact with vaginal flora. 4 However, based on current evidence, vaginal delivery for infants with gastroschisis has no contraindications based on factors such as timing (lung maturity), US findings (fetal growth, bowel appearance), and fetal testing results. Therefore, vaginal delivery at the 38th week of gestation is the preferred method for women carrying a fetus with gastroschisis. If there are associated complications, such as marked liver herniation, then cesarean section should be considered. 5
At birth, neonates with gastroschisis may have hypothermia or intestines that appear discolored, suggesting injury or insufficient blood flow. Rarely, additional internal organs may herniate, including the pancreas, stomach, liver, spleen, bladder, uterus, ovaries, and fallopian tubes. 1 Neonates affected by this condition may also suffer from sepsis, necrotizing enterocolitis (NEC), short bowel syndrome, bowel obstruction, and volvulus. 4
Prenatal US can diagnose gastroschisis as early as the first trimester. The prenatal US shows the herniated bowel floating in the amniotic fluid. Prenatal US can also provide prognostic information. Measurement of intra-abdominal bowel dilation (IABD) at the most dilated bowel segment can distinguish complex from simple gastroschisis. A recent longitudinal, prospective multicenter study of 104 patients showed that an intra-abdominal bowel distention of ≥10 mm between 20 and 22 weeks’ gestation is predictive of complex gastroschisis with a specificity of 100%, a positive predictive value of 100%, and a negative predictive value of 77%. 6
The goal of treatment for simple gastroschisis is primary reduction of the herniated viscera. Delays in reduction increase the risk of visceral injury and the development of abdominal compartment syndrome (persistent intra-abdominal pressure (IAP > 20 mm Hg). Staged reduction, usually with the use of a spring-loaded silo, is the preferred method to decrease IAP and lessen the risk of complications with primary reduction. Ultimately, the closure may be sutured, which is associated with a high risk of infection or sutureless closure, which can be performed at the bedside, but is associated with a high rate of secondary hernia. Postoperatively, the infant is advanced to full feedings, with a return of bowel function typically occurring within 4 weeks. 7
The treatment of complex gastroschisis is often intensive and must be individualized depending on comorbidities, gestational age at the time of delivery, and the proportion of herniated viscera to abdominal domain. Intestinal perforation or necrosis is addressed at the time of surgical exploration and reduction; primary resection and anastomosis is often feasible. Resections should be minimal to avoid the development of short-gut syndrome, and ostomies are usually avoidable. 7
Common to both simple and complex gastroschisis, the complications include abdominal compartment syndrome, NEC, midgut volvulus, and adhesive small bowel obstruction. Abdominal compartment syndrome is defined as persistent IAP (> 20 mm Hg), which leads to organ dysfunction, including anuria. NEC develops in approximately 5% of patients, is usually mild, and infrequently requires surgical intervention. Midgut volvulus develops in approximately 1.2% of patients due to adhesion of the small bowel to the lateral abdominal wall. Small bowel obstruction due to adhesions is reported in 20-25% of patients, usually within the first year of life. In complicated gastroschisis, more severe complications are likely related to the increased IAP and fascia closure tension, which can result in organ dysfunction, bowel inflammation, and adhesions. 7 In uncomplicated cases, survival rates can be as high as 97.8% at 1 year.
Conclusion
An external protrusion of the intestines and occasionally other organs without a protective membrane is the hallmark of gastroschisis. Prenatal US, specifically the marker IABD, is the most effective in diagnosing and differentiating between simple and complex gastroschisis. Patients diagnosed with the condition are at a risk of infection, sepsis, and electrolyte imbalances from swelling and inflammation of the exposed organs. Treatment aims for primary reduction of the herniated viscera to prevent visceral injury and abdominal compartment syndrome. Staged reduction using a spring-loaded silo is the preferred method. Complex cases should be treated individually, and any resection should be kept to a minimum to prevent short-gut syndrome. Reported complications include abdominal compartment syndrome (up to 25%), NEC (5%), midgut volvulus (1.2%), and adhesive small bowel obstruction (20-25%).
References
- Fatona O, Opashola K, Faleye A. Gastroschisis in Sub-Saharan Africa: a scoping review of the prevalence, management practices, and associated outcomes. Pediatr Surg Int. 2023;39(1):246. doi:10.1007/s00383-023-05531-w.
- Bhat V, Moront M, Bhandari V. Gastroschisis: a state-of-the-art review. Children. 2020;7(12):302. doi:10.3390/children7120302.
- Bence C, Wagner A. Abdominal wall defects. Transl Pediatr. 2021;10(5):1461-1469. doi:10.21037/tp-20-94.
- Muniz T, Rolo L, Araujo Júnior E. Gastroschisis: embriology, pathogenesis, risk factors, prognosis, and ultrasonographic markers for adverse neonatal outcomes. J Ultrasound. 2024;27(2):241-250. doi:10.1007/s40477-024-00887-8.
- Rentea R, Gupta G. In: StatPearls [Internet]. 2020.
- Joyeux L, Belfort M, Coppi P. Complex gastroschisis: a new indication for fetal surgery?. Ultrasound Obstet Gynecol. 2021;58(6):804-812. doi:10.1002/uodg.24759.
- Bielicki I, Somme S, Frongia G, Holland-Cunz S, Vuille-Dit-Bille R. Abdominal wall defects-current treatments. Children. 2021;8(2):170. doi:10.3390/children8020170.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Gastroschisis. Applied Radiology. 2025. doi:10.37549/JPCR-25-0059.