1 University of Cincinnati College of Medicine, Cincinnati, Ohio
2 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
3 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
* Corresponding author: Alexander J. Towbin (Alexander.Towbin@cchmc.org)
Abstract
Hemiplegic migraine is an uncommon type of migraine with aura caused by abnormalities in calcium ion transport. Because its symptoms overlap with stroke, patients are often initially treated in the emergency room. There, standard anatomic brain imaging is normal. Perfusion imaging, if performed, can aid in the diagnosis. However, the diagnosis is often made clinically based on standard diagnostic criteria.
Keywords
brain, vascular, stroke-like
Categories
Case Summary
An adolescent girl presented to the emergency room for a recurrent episode of headache, right-sided numbness, and right-sided facial droop. An MRI of the brain was conducted to investigate potential structural and cerebrovascular causes of her symptoms.
Imaging Findings
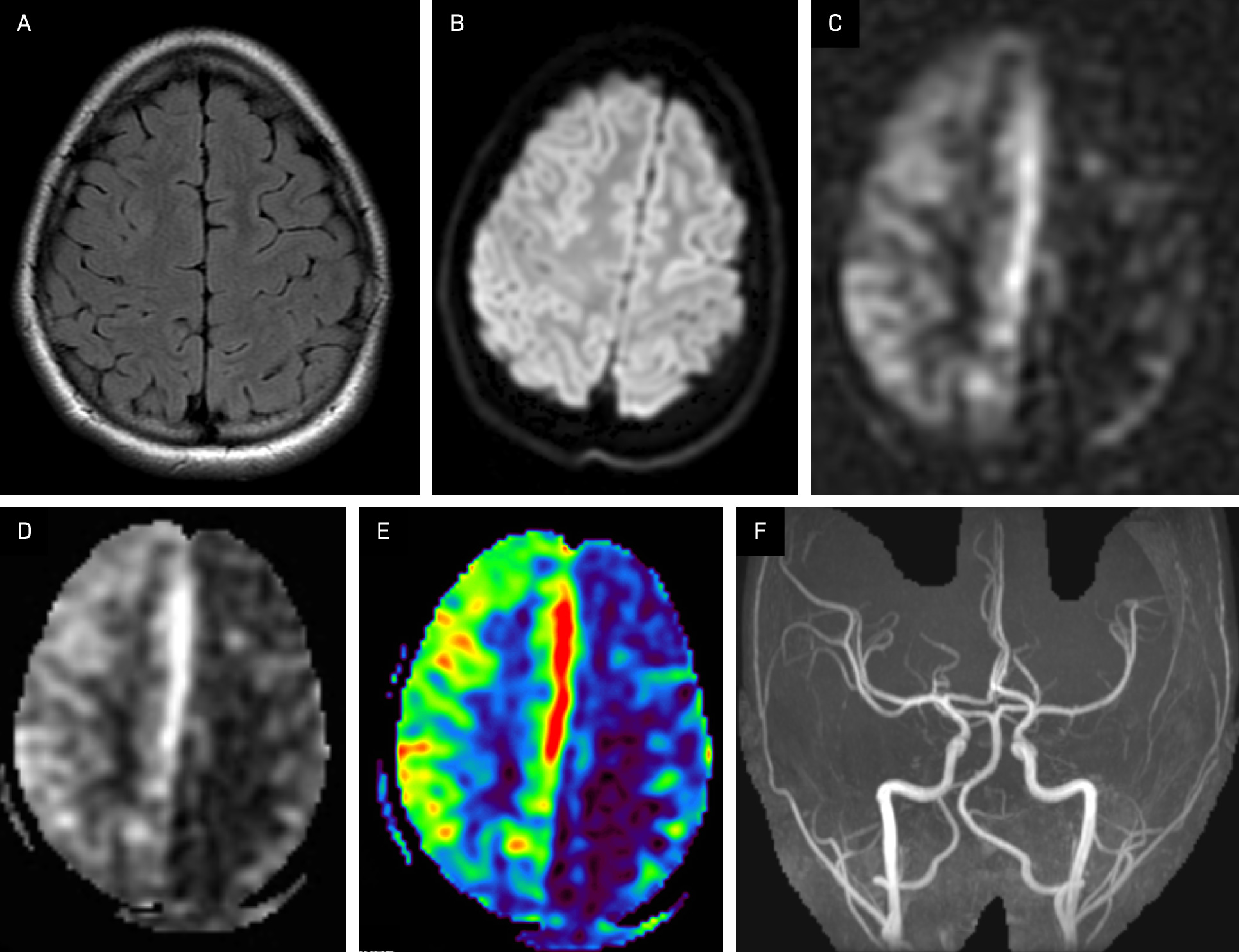
MRI of the brain (Figure 1) revealed normal brain parenchyma with no underlying mass or hemorrhage. MR angiography of the cerebral vasculature was normal. Arterial spin labeling (ASL) perfusion MR revealed markedly decreased perfusion to the left cerebral hemisphere.
Diagnosis
Hemiplegic migraine.
The differential diagnosis for hemiplegic migraines includes transient ischemic attacks, ischemic strokes, and other stroke mimics, including seizures, metabolic disorders such as mitochondrial encephalomyopathy with lactic acidosis and stroke-like episodes, and structural lesions (eg, brain tumors), though this is not a comprehensive list.
Discussion
Hemiplegic migraine is a relatively rare subset of migraine headaches with aura characterized by transient hemiparesis, visual, sensory, and speech disturbances. 1 The diagnosis is made by identifying the clinical symptoms. Because its aura symptoms overlap with stroke, imaging is often used to exclude other conditions. According to the International Classification of Headache Disorders, hemiplegic migraine is diagnosed in patients who have had at least 2 attacks that meet the criteria for migraine with aura. These criteria include fully reversible aura symptoms such as visual, sensory, speech/language, motor, brainstem, or retinal disturbances, accompanied by at least 3 of the following 6 characteristics: gradual spreading of at least 1 aura symptom over 5 minutes, 2 or more aura symptoms in succession lasting 5‐60 minutes each, at least 1 symptom being unilateral, at least 1 symptom being positive, and the aura being accompanied by a headache within 60 minutes. Additionally, the aura must consist of fully reversible motor weakness and fully reversible visual, sensory, and/or speech/language symptoms and cannot be better explained by another diagnosis. 1
Patients who present with hemiplegic migraine will typically present with an evolving aura. The aura often begins with visual symptoms and progresses to include motor weakness. A headache typically begins during the aura phase and may be unilateral or bilateral. 2 Additionally, the headache may be either ipsilateral or contralateral to the motor aura, so laterality of headache cannot be used to aid in diagnostic decision-making. 3 Patients typically first present during adolescence. Like other forms of migraines, a hemiplegic migraine is more common in females. 4 Most attacks of a hemiplegic migraine occur without a recognized trigger, though there are some described triggers, which are like those of typical migraine. These include emotions (including stress), changes in sleep patterns, and bright lights. 5
Hemiplegic migraines can occur sporadically in individuals or can occur as a familial hemiplegic migraine. Familial hemiplegic migraine usually occurs due to mutations in the CACNA1A gene, encoding a subunit of the P/Q-type calcium channel, termed FHM1. 2,6 Several other suspected genetic variants not associated with a classified FHM type are believed to interact with ion transport, supporting the suspected mechanism of hemiplegic migraine caused by atypical depolarization spreading across the cortex, leading to aura symptoms. Familial cases of hemiplegic migraine follow an autosomal dominant inheritance pattern and exhibit high penetrance, which can be reassuring when a young patient presents with typical aura symptoms and has a positive family history. Patients with the sporadic forms of hemiplegic migraine frequently have the same type of genetic mutations.
When diagnosing hemiplegic migraine, imaging is used to exclude other potential causes of focal neurological deficits, such as stroke and tumor. Because of this, a non-contrast head CT is often the initial imaging study performed. Most anatomic imaging techniques, including contrast-enhanced and non-contrast CT and MRI, are normal. Although not necessary for diagnosis, ASL perfusion MR may demonstrate markedly decreased perfusion in the contralateral cerebral hemisphere early during an attack, aiding in the diagnosis of hemiplegic migraine. 7 The hypoperfusion may give rise to hyperperfusion as the attack progresses. The mechanisms for these perfusion abnormalities are not well understood, and the location does not necessarily correlate with aura symptoms. 8 Similar findings may be seen on CT perfusion imaging, but of the two, MRI is the preferred imaging modality because of the lack of ionizing radiation and higher sensitivity for the other conditions in the differential diagnosis. 9
The symptoms of hemiplegic migraine typically resolve within a few hours. Hemiplegic migraines are managed in a similar fashion to other forms of migraine. Verapamil is the usual medication of choice. Preventive options include topiramate, amitriptyline, and acetazolamide. 10-12 While used to treat other forms of migraines, triptans and ergotamine derivatives are avoided in patients with hemiplegic migraines to stay away from the medication’s vasoconstrictive effects. 12
Conclusion
Hemiplegic migraine is an uncommon type of migraine with aura caused by abnormalities in calcium ion transport. Because its symptoms overlap with stroke, patients are often initially treated in the emergency room. There, standard anatomic brain imaging is normal. Perfusion imaging, if performed, can aid in the diagnosis. However, the diagnosis is often made clinically based on standard diagnostic criteria.
References
- Olesen J. International classification of headache disorders. Lancet Neurol. 2018;17(5):396-397. doi:10.1016/S1474-4422(18)30085-1.
- Ducros A, Denier C, Joutel A. The clinical spectrum of familial hemiplegic migraine associated with mutations in a neuronal calcium channel. N Engl J Med. 2001;345(1):17-24. doi:10.1056/NEJM200107053450103.
- Russell M, Ducros A. Sporadic and familial hemiplegic migraine: pathophysiological mechanisms, clinical characteristics, diagnosis, and management. Lancet Neurol. 2011;10(5):457-470. doi:10.1016/S1474-4422(11)70048-5.
- Thomsen L, Eriksen M, Roemer S. A population-based study of familial hemiplegic migraine suggests revised diagnostic criteria. Brain. 2002;125(pt 6):1379-1391. doi:10.1093/brain/awf132.
- Hansen J, Hauge A, Ashina M, Olesen J. Trigger factors for familial hemiplegic migraine. Cephalalgia. 2011;31(12):1274-1281. doi:10.1177/0333102411415878.
- Riant F, Roze E, Barbance C. PRRT2 mutations cause hemiplegic migraine. Neurology. 2012;79(21):2122-2124. doi:10.1212/WNL.0b013e3182752cb8.
- Ryan D, Coughlan S, McSweeney N, Dineen J, Fanning N. Hemiplegic migraine as a stroke mimic: imaging and electroencephalography findings. Stroke. 2023;54(7). doi:10.1161/STROKEAHA.122.041369.
- Charles A. The migraine aura. Continuum. 2018;24(4, Headache):1009-1022. doi:10.1212/CON.0000000000000627.
- Strambo D, Nannoni S, Rebordão L, Dunet V, Michel P. Computed tomographic perfusion abnormalities in acute migraine with aura: characteristics and comparison with transient ischemic attack. Eur Stroke J. 2022;7(4):431-438. doi:10.1177/23969873221114256.
- Yu W, Horowitz S. Treatment of sporadic hemiplegic migraine with calcium-channel blocker verapamil. Neurology. 2003;60(1):120-121. doi:10.1212/01.wnl.0000042051.16284.70.
- Pelzer N, Stam A, Haan J, Ferrari M, Terwindt G. Familial and sporadic hemiplegic migraine: diagnosis and treatment. Curr Treat Options Neurol. 2013;15(1):13-27. doi:10.1007/s11940-012-0208-3.
- Wammes-van der Heijden E, Rahimtoola H, Leufkens H, Tijssen C, Egberts A. Risk of ischemic complications related to the intensity of triptan and ergotamine use. Neurology. 2006;67(7):1128-1134. doi:10.1212/01.wnl.0000240128.76399.fa.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript, and no part of this article has been previously published elsewhere.
Citation
. Hemiplegic Migraine. Applied Radiology. 2025. doi:10.37549/JPCR-25-0060.