Hemolytic Uremic Syndrome
Journal of Pediatric Case Reports — Vol. 1 , Issue 3
Published: April 1, 2026
1 University of Arizona College of Medicine-Phoenix Campus, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Hemolytic uremic syndrome (HUS) is a thrombotic microangiopathy defined by the triad of renal failure, hemolytic anemia, and thrombocytopenia. It is a leading cause of acute kidney injury in young children. HUS is now classified by etiology rather than clinical features, with Shiga toxin-producing Escherichia coli accounting for most pediatric cases. Atypical HUS, most often due to complement dysregulation, is less common and carries a higher risk for chronic renal impairment. Diagnosis is clinical, supported by gastrointestinal symptoms and characteristic laboratory findings. Imaging plays an important role in evaluating complications and guiding treatment. Renal US can help assess disease severity, while neuroimaging is used in patients with suspected central nervous system involvement. Management is primarily supportive, with early hydration and dialysis when indicated. Outcomes depend on the underlying etiology and severity of organ involvement, with neurologic and cardiac complications being the primary drivers of mortality.
Keywords
renal, vascular, chronic kidney disease
Categories
Case Summary
A toddler presented with 2 days of diarrhea and vomiting without fever. Stool cultures confirmed infection with Escherichia coli.
Imaging Findings
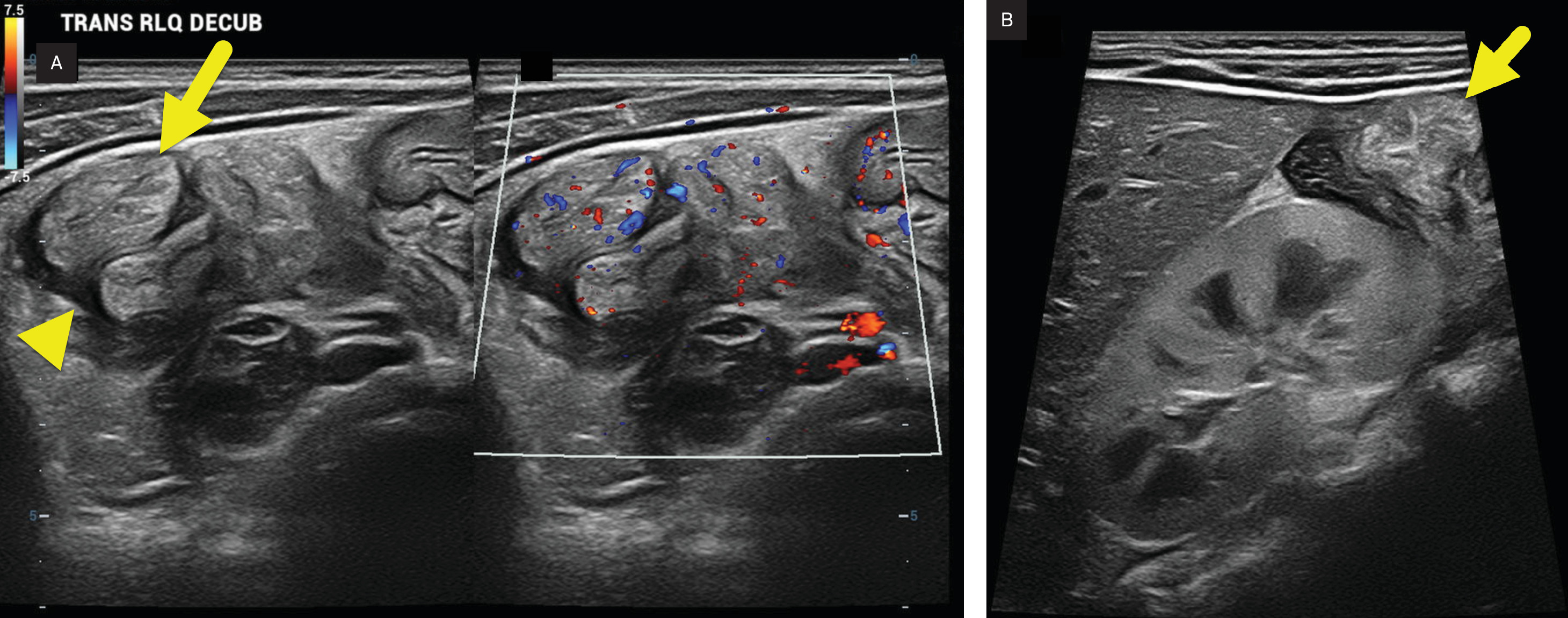
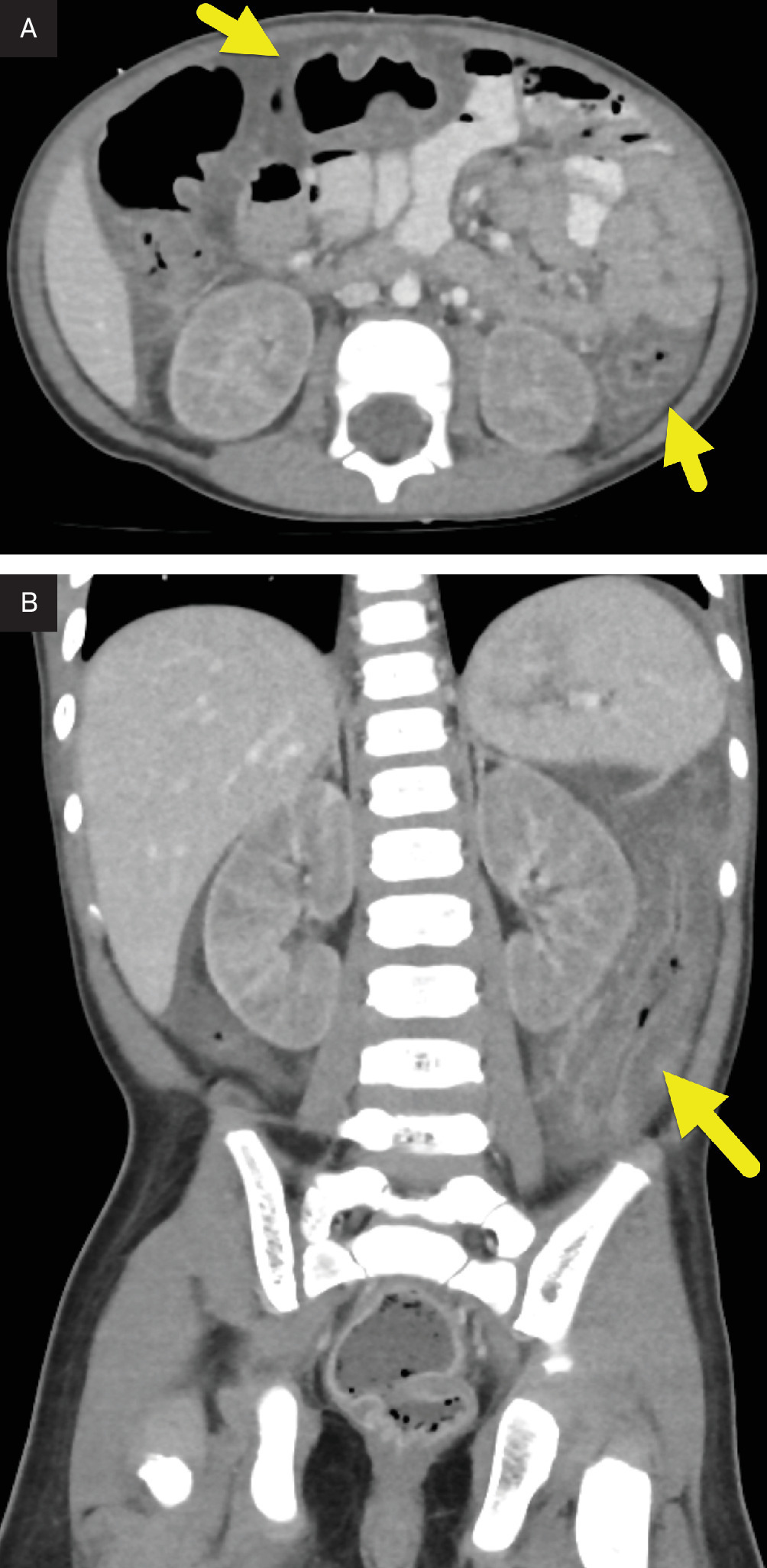
Bowel US (Figure 1) showed diffuse bowel wall thickening, bowel hyperemia, and mild ascites. The kidneys were enlarged and echogenic. Subsequent abdominal CT (Figure 2) showed similar findings. The kidneys appeared enlarged with abnormal decreased cortical enhancement.
Diagnosis
Hemolytic uremic syndrome (HUS).
The differential diagnosis includes thrombotic thrombocytopenic purpura, disseminated intravascular coagulation, malignant hypertension, juvenile-onset, and systemic lupus erythematosus.
Discussion
HUS is a thrombotic microangiopathy characterized by a clinical triad of renal failure, hemolytic anemia, and thrombocytopenia. It is a major cause of acute kidney injury and acquired chronic kidney disease in children under 5 years of age.1
Historically, HUS was classified by the presence or absence of diarrhea: “typical” or “diarrhea-positive” HUS, and “atypical” or “diarrhea-negative” HUS.2 However, recent studies have shown that atypical HUS (aHUS) can present with diarrhea in up to 30% of cases.3 As a result, a classification based on etiology is now preferred. Shiga toxin-producing Escherichia coli hemolytic uremic syndrome (STEC-HUS) accounts for 85-90% of pediatric cases.2,3 Approximately 15% of children infected with STEC develop HUS. The Shiga toxin binds to globotriaosylceramide receptors on renal endothelial cells, initiating inflammation, endothelial damage, and microvascular thrombosis.4,5
In contrast, aHUS is primarily a result of dysregulation of the alternative complement pathway. It accounts for 5-10% of HUS cases and may be either genetic or sporadic. Mutations in complement regulatory genes are identified in about 50% of patients with aHUS.5 Additional rare variants include Streptococcus pneumoniae-associated HUS and secondary forms related to autoimmune diseases, transplants, or infections. Despite evolving classification schemes, inconsistency in terminology remains across the literature. aHUS usually presents with nonspecific symptoms such as fatigue, pallor, or somnolence that may progress to acute kidney injury. The risk of progression to end-stage kidney disease is high. Like HUS, aHUS demonstrates extrarenal findings and can present with diarrhea in about a third of cases.6
Epidemiologic patterns vary by geography and age.2 Children have the highest incidence. In Europe and North America, STEC-HUS occurs at rates of 0.6‐0.8 per 100,000 children under 15‐18 years of age, and 1.9‐2.9 per 100,000 in those under 3‐5 years. Incidence in Latin America is approximately 10 times higher. In contrast, aHUS is rare, with an estimated incidence of 0.10‐0.11 cases per million children.7
Diagnosis is clinical, supported by a history of gastrointestinal illness and laboratory findings consistent with the HUS triad. Patients with STEC-HUS typically develop watery, bloody diarrhea 3‐8 days after exposure to contaminated food.2 Associated symptoms include abdominal pain, vomiting, and hypertension. Renal involvement ranges from hematuria and proteinuria to oliguria and acute kidney failure, with approximately 20% requiring dialysis.8
Central nervous system involvement occurs in 20-50% of patients and is the most serious complication leading to increased mortality and long-term neurologic deficits.4 Neurologic symptoms include seizures, irritability, altered mental status, and focal deficits. Other organ systems may also be affected, with potential complications including gastrointestinal injury, cardiac ischemia, diabetes mellitus, and hepatomegaly.2 The overall mortality rate for HUS is about 5%, primarily due to central nervous system and cardiac complications.
Laboratory evaluation typically reveals hemolytic anemia, thrombocytopenia, and elevated creatinine. Schistocytes may be seen on peripheral smear. Stool culture or PCR for E. coli O157:H7 can support a diagnosis of STEC-HUS, although serum anti-O157 antibody may be more sensitive.4
Imaging is used to help support the diagnosis, identify potential complications, and assess disease severity. Chest radiography may help assess for pulmonary edema and cardiac enlargement. Echocardiography is indicated when cardiac dysfunction is suspected.9
Renal US is helpful during the prodromal phase. Resistive index (RI) and kidney size are useful in assessing disease severity. Rink et al. found that patients with HUS had elevated RI (mean 0.87±0.10) and increased kidney volume (mean 177.4% of age-adjusted normal) at disease onset. Patients requiring dialysis had larger kidneys than those who did not.10
Neuroimaging is used to evaluate central nervous system complications. Noncontrast CT is typically used to exclude hemorrhage or infarction. MRI provides greater sensitivity for cytotoxic edema and is useful for assessing disease severity and prognosis. Bilateral T2 and diffusion-weighted hyperintensities in the basal ganglia, thalami, and white matter are common findings.4,11 These changes are often reversible, although in severe cases they may predict poor neurologic outcomes.
Management is primarily supportive. Most patients require transfusion of volume-reduced, platelet-depleted red blood cells.4 Early aggressive intravenous hydration (10 mL/kg/hour of 0.9% saline for 3 hours) can reduce dialysis requirements, hospital stay, and the risk of central nervous system injury.12 About half of the STEC-HUS patients require dialysis. End-stage renal disease is more common in aHUS and may necessitate kidney transplantation. Antibiotics and antidiarrheal agents are avoided in STEC-HUS due to the risk of increased Shiga toxin release. In contrast, antibiotics are indicated for S. pneumoniae-associated HUS.
Conclusion
HUS is a thrombotic microangiopathy defined by the triad of renal failure, hemolytic anemia, and thrombocytopenia. It is a leading cause of acute kidney injury in young children. HUS is now classified by etiology rather than clinical features, with STEC accounting for the majority of pediatric cases. aHUS, most often due to complement dysregulation, is less common and carries a higher risk for chronic renal impairment.
Diagnosis is clinical, supported by gastrointestinal symptoms and characteristic laboratory findings. Imaging plays an important role in evaluating complications and guiding treatment. Renal US can help assess disease severity, while neuroimaging is used in patients with suspected central nervous system involvement. Management is primarily supportive, with early hydration and dialysis when indicated. Outcomes depend on the underlying etiology and severity of organ involvement, with neurologic and cardiac complications being the primary drivers of mortality.
References
- Grisaru S. Management of hemolytic-uremic syndrome in children. Int J Nephrol Renovasc Dis. 2014;7:231-239. doi:10.2147/IJNRD.S41837.
- Gülhan B, Özaltın F. Hemolytic uremic syndrome in children. Turk Arch Pediatr. 2021;56(5):415-422. doi:10.5152/TurkArchPediatr.2021.21128.
- Bhandari J, Rout P, Sedhai Y. In: StatPearls. 2023.
- Boyer O, Niaudet P. Hemolytic-uremic syndrome in children. Pediatr Clin North Am. 2022;69(6):1181-1197. doi:10.1016/j.pcl.2022.07.006.
- Petruzziello-Pellegrini T, Marsden P. Shiga toxin-associated hemolytic uremic syndrome: advances in pathogenesis and therapeutics. Curr Opin Nephrol Hypertens. 2012;21(4):433-440. doi:10.1097/MNH.0b013e328354a62e.
- Jokiranta T. HUS and atypical HUS. Blood. 2017;129(21):2847-2856. doi:10.1182/blood-2016-11-709865.
- Raina R, Krishnappa V, Blaha T. Atypical hemolytic-uremic syndrome: an update on pathophysiology, diagnosis, and treatment. Ther Apher Dial. 2018;23(1):4-21. doi:10.1111/1744-9987.12763.
- Rivetti G, Gizzone P, Petrone D. Acute kidney injury in children: a focus for the general pediatrician. Children. 2024;11(8). doi:10.3390/children11081004.
- Kim E, Kim S. Multiple extrarenal manifestations in hemolytic uremic syndrome: a case report. Korean J Pediatr. 2007;50(12):1261. doi:10.3345/kjp.2007.50.12.1261.
- Rink L, Finkelberg I, Kreuzer M. Ultrasound analysis of different forms of hemolytic uremic syndrome in children. Front Pediatr. 2024;12. doi:10.3389/fped.2024.1433812.
- Mansour M, Khalil D, Hasham M. Hemolytic uremic syndrome with central nervous system manifestations, a case report and literature review. Radiol Case Rep. 2023;18(6):2268-2273. doi:10.1016/j.radcr.2023.02.035.
- Bilkis M, Bonany P. Hydration in hemolytic uremic syndrome. Arch Argent Pediatr. 2021;119(1):62-66. doi:10.5546/aap.2021.eng.62.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Hemolytic Uremic Syndrome. Journal of Pediatric Case Reports. 2026;1(3). doi:10.37549/JPCR-26-0091.