1 Texas Tech University Health Sciences Center El Paso, El Paso, Texas
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Children’s Hospital of Cincinnati, University of Cincinnati College of Medicine, Cincinnati, Ohio
Abstract
Contrast enema is the primary modality for diagnosing Hirschsprung’s disease in the neonate. The most common findings on imaging are a rectosigmoid transitional zone, an abnormal rectosigmoid index, and a saw-tooth pattern depicting impaired peristalsis. The absence of a transitional zone in the neonate may observed due to immature bowel. A suction rectal biopsy is the gold standard to confirm the diagnosis.
Keywords
Gastrointestinal, Congenital, Colon
Categories
Case Summary
A term neonate presented with abdominal distension and failure to pass meconium.
Imaging Findings
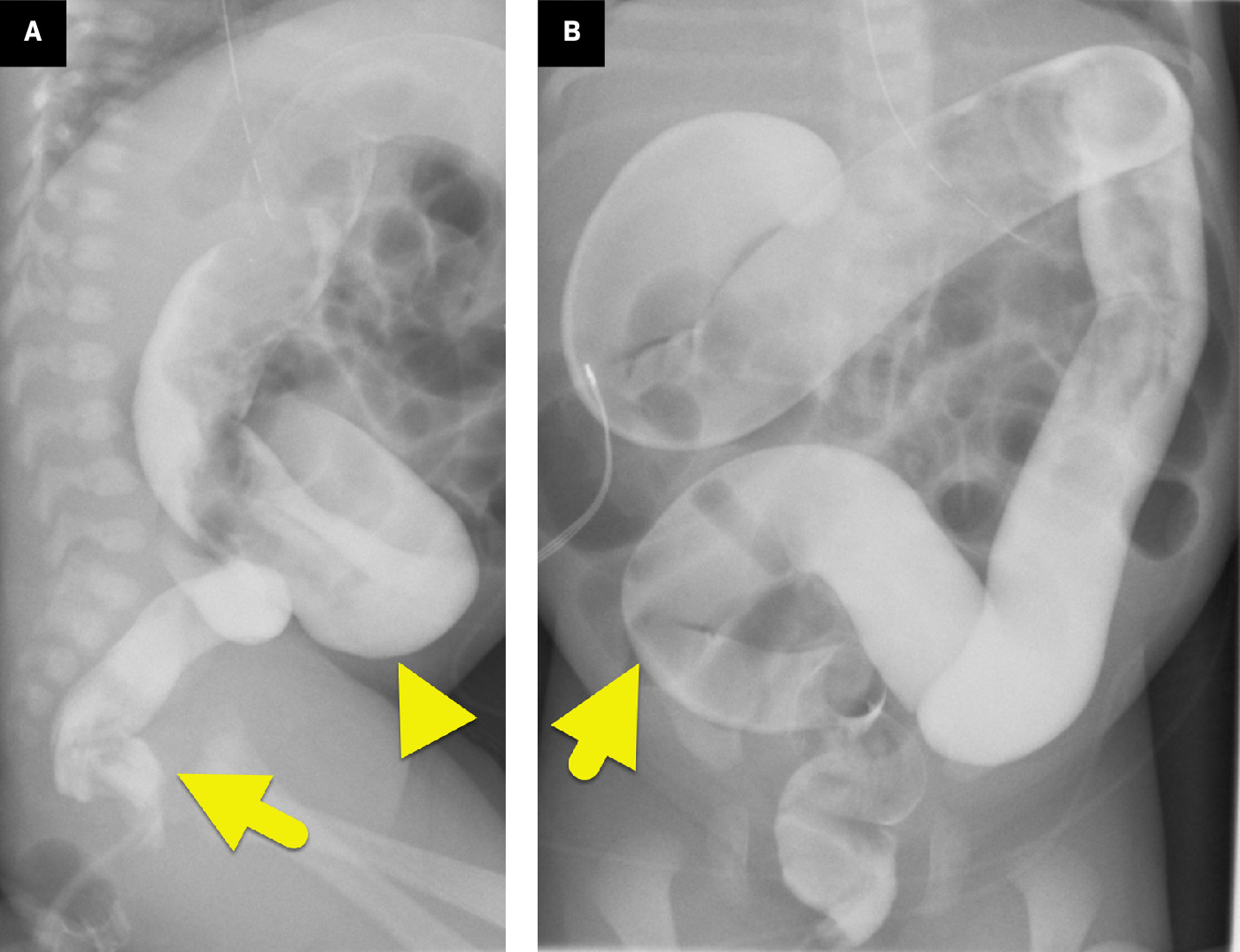
Abdominal radiograph (Figure 1) showed dilated, air-filled loops of bowel. No gas was present in the rectum. Water-soluble contrast enema (Figure 2) showed an abnormal rectosigmoid ratio and a transition point at the mid-sigmoid colon. More proximal colon was dilated and had meconium filling defects.

Diagnosis
Hirschsprung disease.
Presenting with imaging findings of dilated small bowel and colonic loops of intestines suggests a distal colonic obstruction. The differential diagnosis includes colonic atresia, anorectal malformations, megacystis-microcolon-intestinal hypoperistalsis syndrome, meconium plug syndrome, and functional immaturity of the left colon. The diagnosis is made by a combination of clinical features and imaging with abdominal radiographs and contrast enema to determine the level of obstruction.
Discussion
Hirschsprung disease is the most common enteric nervous system developmental disorder and occurs in approximately 1 in 5000 live births worldwide. 1 There is a male-to-female predominance of 4:1, and around 26.1% of patients will have associated congenital defects. 1,2 Of the associated congenital abnormalities, trisomy 21 has shown a constant association with 2-15% incidence. 3 Sensorineural deafness, Waardenburg syndrome, neurofibromatosis, neuroblastoma, Multiple Endocrine Neoplasia syndromes, and pheochromocytoma are additional chromosomal abnormalities that have a well-defined association with Hirschsprung. 1,3 By order of frequency, individual anomalies include gastrointestinal tract (8.05%), the central nervous system and sensorineural anomalies (6.79% each), genitourinary tract (6.05%), musculoskeletal (5.12%), and cardiovascular system (4.99%). 3
Hirschsprung is a heritable condition with a multigenetic component, namely mutations in key signaling pathways such as the RET and endothelin receptor B (EDNRB). 1,4 Enteric neural crest-derived cells are the building blocks of the neural tube, forming the brain and spinal cord. These cells migrate, proliferate, then differentiate into the many cell types contributing to tissues and organs. The differentiation of neural crest cells into the enteric nervous system, innervating gastrointestinal mobility, is tightly regulated by signaling pathways and transcriptional factors. The tyrosine kinase transmembrane receptor, RET, is the most notable, ensuring appropriate proliferation, migration, and survival of enteric neural crest cells. SOX10 and PHOX2B are the key transcription factors required to activate the RET pathway. 1 EDNRB, a G protein-coupled receptor, is another crucial component helping proliferation of cells toward gastrointestinal development. 1,4 Any disruption of these pathways interrupts enteric cell proliferation, causing aganglionosis, and therefore is associated with Hirschsprung. 1,3,4
Hirschsprung is a neurocristopathy that arises due to various errors in key signaling pathways. With this variability, arrest of craniocaudal migration of vagal neural crest cells during the 5th and 12th weeks of gestation can lead to differences in colonic involvement. 80% of cases are short segment, involving only the rectosigmoid colon, and 10-15% extend proximally to the sigmoid colon. 5% of cases have total colon involvement. 4 The lack of parasympathetic intermuscular and submucosal plexuses (Auerbach and Meissner, respectively) results in the inability of colonic relaxation and a functional obstruction. 5
Clinical symptoms share similarities with distal intestinal obstruction such as abdominal distension, bilious vomiting, and failure to pass meconium beyond the first 24-48 hours of life. Late presentations include chronic constipation and failure to thrive. 2 Diagnosis is confirmed based primarily on rectal biopsy; however, imaging guides surgical planning and helps differentiate from other obstructive pathologies. 5 Diagnosis is confirmed with suction or full-thickness rectal biopsy. A suction biopsy can be an office procedure and is less invasive and does not need general anesthesia. The biopsy specimen is from the submucosa. It results in a small tissue sample that can be insufficient for diagnosis. A full-thickness biopsy is performed under general anesthesia and obtains tissue from all rectal wall layers and is considered the gold standard. The procedure selected often depends upon the child’s age and clinical suspicion of HD. Suction biopsy is often preferred in young infants because it is less invasive. A full-thickness biopsy is usually chosen for older children and those with an inconclusive suction biopsy. The pathological findings include absence of the myenteric plexus of colon in the submucosal layer of the wall, leading to a functional obstruction. Histologically, there are hypertrophied nerve fibers using H&E stains or acetylcholinesterase histochemistry and calretinin immunohistochemistry, and thickened bowel wall.
Abdominal radiographs are typically the first imaging modality performed, and findings may be nonspecific. Findings include dilated bowel loops proximal to the aganglionic region, suggesting the diagnosis of a distal bowel obstruction. 2,5 Fluoroscopy-guided contrast enema remains the mainstay of diagnostic imaging for Hirschsprung, increasing the probability of diagnosis compared with clinical suspicion alone. 2
Characteristic findings on a contrast enema include an abnormal rectosigmoid index (RSI) and radiographic transition zone (RTZ) in patients with short-segment disease. 6 A lateral view is best to visualize the transition zone, a cone-shaped delineation between dilated proximal bowel and normal caliber distal bowel. An RSI is calculated by dividing the widest diameter of the rectum by the widest diameter of the sigmoid colon. Hirschsprung is defined by an RSI index of <1. A serrated, “saw-tooth” appearance may be seen as a result of impaired peristalsis with uncoordinated contractions. 7 As a result, a 24-hour delayed image is valuable. 2 The sensitivity and specificity of an RTZ or abnormal RSI on enema are 75-85% and 95-96%, respectively. 7 In patients with total colonic disease, the key imaging findings on abdominal radiography are distended small bowel and possibly proximal colon and absent gas in the rectum. A contrast enema shows an indistinct transition zone between dilated and collapsed bowel loops, shortened colon (comma or question mark shaped) that can be normal or near normal in caliber, sawtooth contractions, and delayed evacuation of contrast may be present. 2,4 Using imaging alone, it can be challenging to distinguish between long-segment and total colonic agangliosis. The imaging features of a contrast enema may be variable, and a transition zone may be absent in up to 25% of cases. 6 Of these findings, ileocecal valve reflux and the question mark sign are the better predictors of total colonic involvement. 6 Therefore, it is important to understand that the gold standard for diagnosis is a biopsy.
The features that suggest the diagnosis of long-segment disease include visualization of a transition zone between dilated and narrowed bowel, there may be a saw-toothed pattern of contractions, and contrast evacuation is delayed around 24 hours. In contrast, in total colonic HD, there is no transition zone, comma, or question mark-shaped, featureless microcolon present, and dilated terminal ileum and very delayed contrast evacuation.
While the transition zone and RSI are common radiographic signs, this is not always the case in patients with total colonic involvement. Total colonic aganglionosis often presents with normal, nonspecific findings. 6 Signs of a microcolon, question mark sign, and ileocecal valve reflux suggest aganglionosis that extends toward the ileum.
In cases with a rectosigmoid transition zone, the sensitivity and specificity are about 63% and 100%, respectively. However, in patients with total colonic involvement, the predictive value is 25% or less. 8 Additionally, a transition zone and sawtooth pattern may be difficult to visualize in neonates with immature bowel development. 5 In patients with total colonic disease, aganglionosis is often found to be more proximal to the transition zone and can include false transition zones, making surgical planning difficult. 2,8
Radiography is the first line of investigation serving as a noninvasive approach that can aid in surgical planning. 7 Confirmation of diagnosis is made by suction rectal biopsy as its sensitivity and specificity are near 100% compared with the use of RTZ and RSI (75-85% and 95-96%, respectively). 7,9
HD is treated surgically with resection of the aganglionic segment and anastomosis of the healthy colon to the normally innervated anal segment (pull-through). This pull-through procedure can be performed using an open procedure or laparoscopically, which is the preferred approach. The Swenson procedure resects the entirety of the aganglionic segment and anastomosis of normal bowel to the rectal sphincter. The Duhamel procedure is similar, though the denervated anterior bowel wall is left in place and is anastomosed posteriorly with functional bowel. 2 This procedure is most used with total colonic Hirschsprung disease to preserve the rectal innervation. 2,8 The endorectal pull-through is performed using denervated mucosal resection and pulling of the muscular cylinder distally toward the pectineal line. 2 Patients with total colonic HD can undergo a 2-stage procedure or total colectomy and ileoanal anastomosis. Stage 1 of the 2-staged procedure is to remove the aganglionic bowel and create an ostomy. After several months, the second stage takes down the ostomy and connects the healthy bowel to the anus. 2 Intraoperatively, biopsies are performed to confirm that the aganglionic bowel has been totally removed. Complications occur in almost 50% of cases. They include constipation, bowel obstruction, rectal perforation, and enterocolitis. If untreated, enterocolitis can be fatal. The overall mortality rate has been reduced by advances in surgical techniques and postoperative care and is 1-3%. 2 The long-term prognosis is variable and depends upon the severity of HD and the associated finding. Although the quality of life can be suboptimal, long-term survival can be expected with uncomplicated diseases. As surgery is not without complications, stem cell transplantation is a hopeful prospect.
Treatment is surgical, with the initial procedure being the Swensen. The Swenson procedure resects the entirety of the aganglionic segment and anastomosis of normal bowel to the rectal sphincter. The Duhamel procedure is similar, though the denervated anterior bowel wall is left in place and is anastomosed posteriorly with functional bowel. 2 This procedure is most used with total colonic Hirschsprung disease to preserve the rectal innervation. 2,8 The endorectal pull-through is performed using denervated mucosal resection and pulling of the muscular cylinder distally toward the pectineal line. Intraoperatively, biopsies are performed to confirm that the aganglionic bowel has been totally removed.
Conclusion
Contrast enema is the primary modality for diagnosing Hirschsprung disease in the neonate. The most common findings on imaging are a rectosigmoid transitional zone, an abnormal RSI, and a sawtooth pattern depicting impaired peristalsis. The absence of a transitional zone in the neonate may observed due to immature bowel. A suction rectal biopsy is the gold standard to confirm the diagnosis.
References
- Klein M, Varga I. Hirschsprung’s disease-recent understanding of embryonic aspects, etiopathogenesis and future treatment avenues. Medicina. 2020;56(11):611. doi:10.3390/medicina56110611.
- Hernanz-Schulman M, Coley B. Caffey’s Pediatric Diagnostic Imaging. 2019:1008-1023.
- Moore S. Chromosomal and related mendelian syndromes associated with hirschsprung’s disease. Pediatr Surg Int. 2012;28(11):1045-1058. doi:10.1007/s00383-012-3175-6.
- Mueller J, Goldstein A. The science of hirschsprung disease: what we know and where we are headed. Semin Pediatr Surg. 2022;31(2):151157. doi:10.1016/j.sempedsurg.2022.151157.
- Stanescu A, Liszewski M, Lee E, Phillips G. Neonatal gastrointestinal emergencies: step-by-step approach. Radiol Clin North Am. 2017;55(4):717-739. doi:10.1016/j.rcl.2017.02.010.
- Yan J, Sun J, Wu R. Barium enema findings in total colonic aganglionosis: a single-center, retrospective study. BMC Pediatr. 2020;20(1):499. doi:10.1186/s12887-020-02403-3.
- Putnam L, John S, Greenfield S. The utility of the contrast enema in neonates with suspected hirschsprung disease. J Pediatr Surg. 2015;50(6):963-966. doi:10.1016/j.jpedsurg.2015.03.019.
- Proctor M, Traubici J, Langer J. Correlation between radiographic transition zone and level of aganglionosis in Hirschsprung’s disease: implications for surgical approach. J Pediatr Surg. 2003;38(5):775-778. doi:10.1016/jpsu.2003.50165.
- Allen A, Putnam A, Presson A. Accuracy of suction rectal biopsy for diagnosis of Hirschsprung’s disease in neonates. Eur J Pediatr Surg. 2019;29(5):425-430. doi:10.1055/s-0038-1667040.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Hirschsprung Disease. Applied Radiology. 2026. doi:10.37549/JPCR-25-0063.