Hypertrophic Pyloric Stenosis
Applied Radiology
Published: October 21, 2025
1 University of California, San Diego, College of Medicine, San Diego, California
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Children Hospital Medical Center, Cincinnati, Ohio
4 University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Male infants with persistent or projectile vomiting with a suspicion of hypertrophic pyloric stenosis (HPS) should be referred for an abdominal ultrasound. Once HPS is suspected or confirmed, the initial treatment should be rehydration and correction of electrolyte imbalances. Then, a pyloromyotomy (open or laparoscopic) is curative.11
Keywords
stomach obstruction, neonate, gastrointestinal
Categories
Case Summary
A term male infant presented with weeks of vomiting. However, there was a progression of vomiting after feeding over the past 3 days with non-bilious, non-bloody projectile emesis three times per day. The infant also had associated lethargy, decreased urine and stool output, and weight loss. Laboratory findings included a potassium of 2.3 (normal=3.6-5.2) mmol/L, sodium 126 (133-145) mmol/L, chloride 75 (90-110) mmol/L, and bicarbonate (CO2)>40 (17-27). The patient was fluid resuscitated and electrolytes normalized prior to surgery, after which a laparoscopic pyloromyotomy was performed.
Imaging Findings
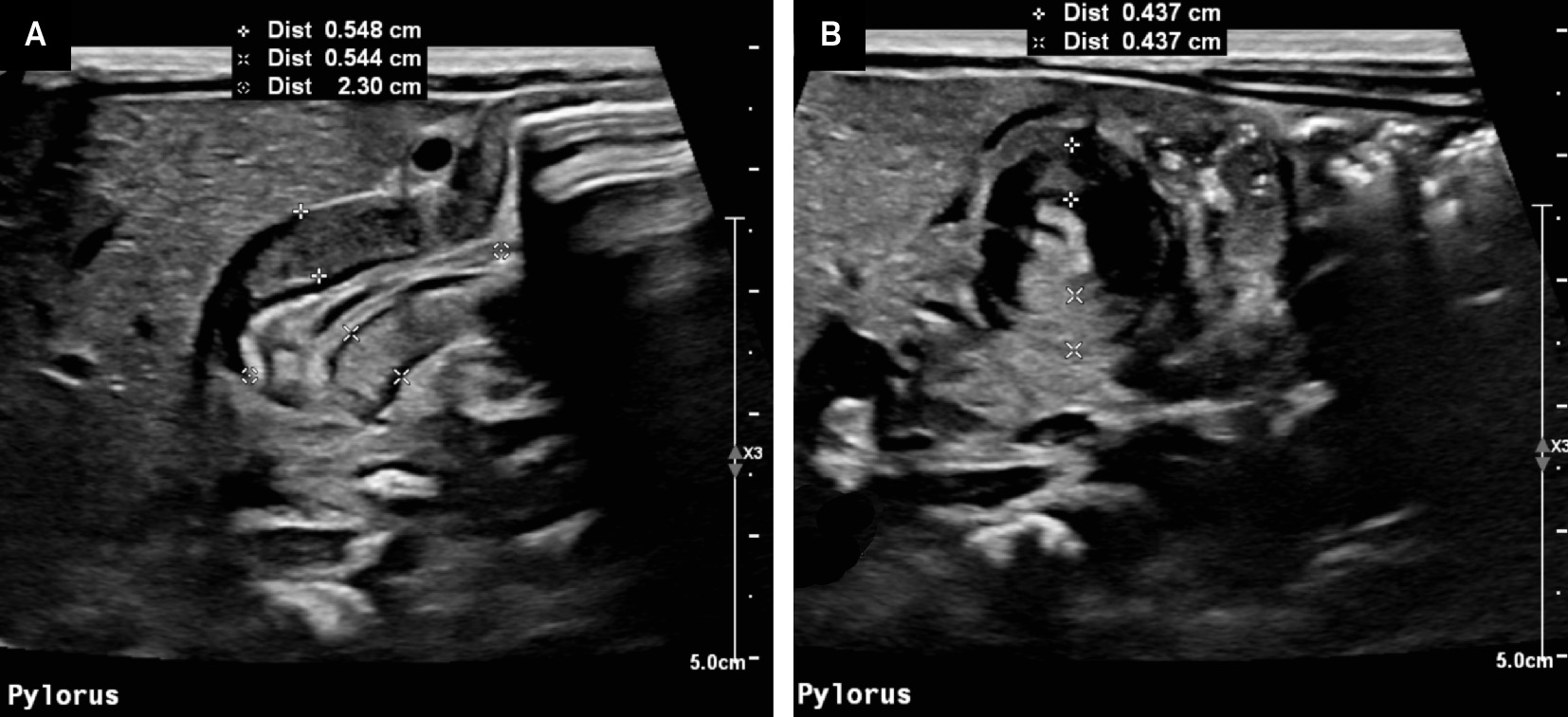
Abdominal ultrasound (Figure 1) was performed, and imaging of the pylorus was abnormal and diagnostic of hypertrophic pyloric stenosis (HPS).
Diagnosis
Infantile HPS.
Differential diagnoses based on clinical findings include midgut volvulus, pylorospasm, gastroesophageal reflux, gastric antral web, annular pancreas, and duodenal stenosis.
Discussion
HPS is an abnormal thickening of the pyloric sphincter obstructing gastric emptying in infants. The cause of HPS is unknown, but it usually presents between 2 and 6 weeks of life. The normal pyloric sphincter is the thickening of the smooth muscle that surrounds the gastric outlet (pylorus). When the pyloric sphincter contracts, gastric contents cannot be propelled into the small intestine. When the sphincter relaxes, gastric contents can pass into the duodenum and continue to be digested. In HPS, the pyloric muscle hypertrophy obstructs flow between the duodenum and the stomach, leading to an increase in intragastric pressure after feeding, leading to projectile vomiting. 1 About one-third of children with the condition do not present with projectile vomiting.
The incidence of HPS is approximately two to five per one thousand births. It typically affects males more frequently than females in a 4:1 ratio. 2 In families with a child with HPS, the likelihood of another child with the condition is increased. If a female child has HPS, the incidence of a future son with the condition is 20%. If a male child has HPS, the incidence of a future son with HPS is 5%. 3 While the etiology is unclear, there is an increased association of HPS with maternal smoking, bottle-feeding, and macrolide antibiotic exposure. 4,5 Additionally, a portion of cases may be attributable to a lack of nitric oxide synthase, which prevents the smooth muscle from relaxing. 6
Typical symptoms involve postprandial non-bilious projectile vomiting in children less than 6 months of age. The increased vomiting contributes to a variety of symptoms. Infants may be lethargic, dehydrated, and exhibit signs such as a sunken anterior fontanelle, dry mucous membranes, and lack of tears when crying. 7 The diagnostic feature on physical examination is palpation of an “olive-shaped” mass in the right upper abdominal quadrant and/or peristaltic waves moving from the left to the right side (“caterpillar sign”). 8 Approximately 20-40% of patients do not have a palpable olive on examination by an experienced examiner.
Laboratory findings classically show hypochloremic, hypokalemic metabolic alkalosis; however, because diagnoses are being made earlier in life due to a high level of clinical suspicion and confirmed with abdominal ultrasound, about 88% of infants have normal or minimally abnormal electrolytes at presentation. Then, prior to surgery, fluid therapy is instituted to correct the electrolyte imbalances. 9 Hypernatremia or hyponatremia may be seen in these infants due to associated dehydration.
Ultrasound is the diagnostic modality of choice and will reveal pyloric wall thickening of 3 mm or greater and a length of 15 mm or greater. The “target sign,” which appears as alternating rings of high and low echogenicity, may be seen due to the thickened pylorus. The sensitivity of 97%, specificity of 100%, and overall reliability and ease of use have made ultrasound the standard method by which pyloric stenosis is diagnosed (Figure 1). 10 Additionally, ultrasound has the added benefit of not requiring the use of radiation or contrast medium. If, however, the ultrasound examination is inconclusive, an upper gastrointestinal series can be useful. The UGI findings may demonstrate an elongated pylorus (“string sign”), beak-like entrance to the pylorus (“beak sign”), and bulging of hypertrophied pyloric muscle (“shoulder sign”). Abdominal radiography lacks the same sensitivity and specificity and is not recommended. Abdominal radiography, however, may show gastric distension but is not diagnostic. Infants with HPS will be cured with a pyloromyotomy. Laparoscopic pyloromyotomy is currently the procedure of choice. Complications from pyloromyotomies are rare and more common in open procedures. The outcomes from pyloromyotomy are very good in the pediatric age group, and infants will grow and thrive.
Conclusion
Male infants with persistent or projectile vomiting with a suspicion of HPS should be referred for an abdominal ultrasound. Once HPS is suspected or confirmed, the initial treatment should be rehydration and correction of electrolyte imbalances. Then, a pyloromyotomy (open or laparoscopic) is curative. 11
References
- Galea R, Said E. Infantile hypertrophic pyloric stenosis: an epidemiological review. Neonatal Netw. 2018;37(4):197-204. doi:10.1891/0730-0832.37.4.197.
- Hernanz-Schulman M. Infantile hypertrophic pyloric stenosis. Radiology. 2003;227(2):319-331. doi:10.1148/radiol.2272011329.
- Pyloric stenosis in children | symptoms, diagnosis & treatment.
- Lund M, Pasternak B, Davidsen R. Use of macrolides in mother and child and risk of infantile hypertrophic pyloric stenosis: nationwide cohort study. BMJ. 2014;348. doi:10.1136/bmj.g1908.
- Krogh C, Biggar R, Fischer T. Bottle-feeding and the risk of pyloric stenosis. Pediatrics. 2012;130(4). doi:10.1542/peds.2011-2785.
- Subramaniam R, Doig C, Moore L. Nitric oxide synthase is absent in only a subset of cases of pyloric stenosis. J Pediatr Surg. 2001;36(4):616-619. doi:10.1053/jpsu.2001.22301.
- Garfield K, Sergent S. StatPearls. 2022.
- Lin C, Chi H, Hsu C. Peristaltic waves in infantile hypertrophic pyloric stenosis. J Pediatr. 2014;164(2):423. doi:10.1016/j.jpeds.2013.08.052.
- Kaye P. Acquired pyloric stenosis resulting in hypokalaemic, hyperchloraemic normal anion gap metabolic acidosis. Persistent vomiting in an adult: cause and effect. BMJ Case Rep. 2018;2018. doi:10.1136/bcr-2017-222800.
- Godbole P, Sprigg A, Dickson J, Lin P. Ultrasound compared with clinical examination in infantile hypertrophic pyloric stenosis. Arch Dis Child. 1996;75(4):335-337. doi:10.1136/adc.75.4.335.
- Binet A, Klipfel C, Meignan P. Laparoscopic pyloromyotomy for hypertrophic pyloric stenosis: a survey of 407 children. Pediatr Surg Int. 2018;34(4):421-426. doi:10.1007/s00383-018-4235-3.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Hypertrophic Pyloric Stenosis. Applied Radiology. 2025. doi:10.37549/JPCR-25-0008.