Liposarcoma of the Lower Extremity
Applied Radiology
Published: October 28, 2025
1 University of Arizona College of Medicine, Phoenix Campus, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Mercy Children’s Hospital, Kansas City, Missouri
4 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Liposarcomas are the second most common soft-tissue tumor and primarily occur within the proximal lower extremity and the retroperitoneum. There are 5 different subtypes of tumor. While there are unique imaging features of each subtype, biopsy is required for diagnosis. Surgical excision remains the primary treatment option for all subtypes of lower extremity liposarcomas.
Keywords
musculoskeletal soft-tissue neoplasm
Categories
Case Summary
A teenage male presented to his primary care physician with left hip pain of 1-month duration and no reported injury. Subsequent outpatient imaging consisting of a noncontrast CT of the pelvis was performed.
Imaging Findings
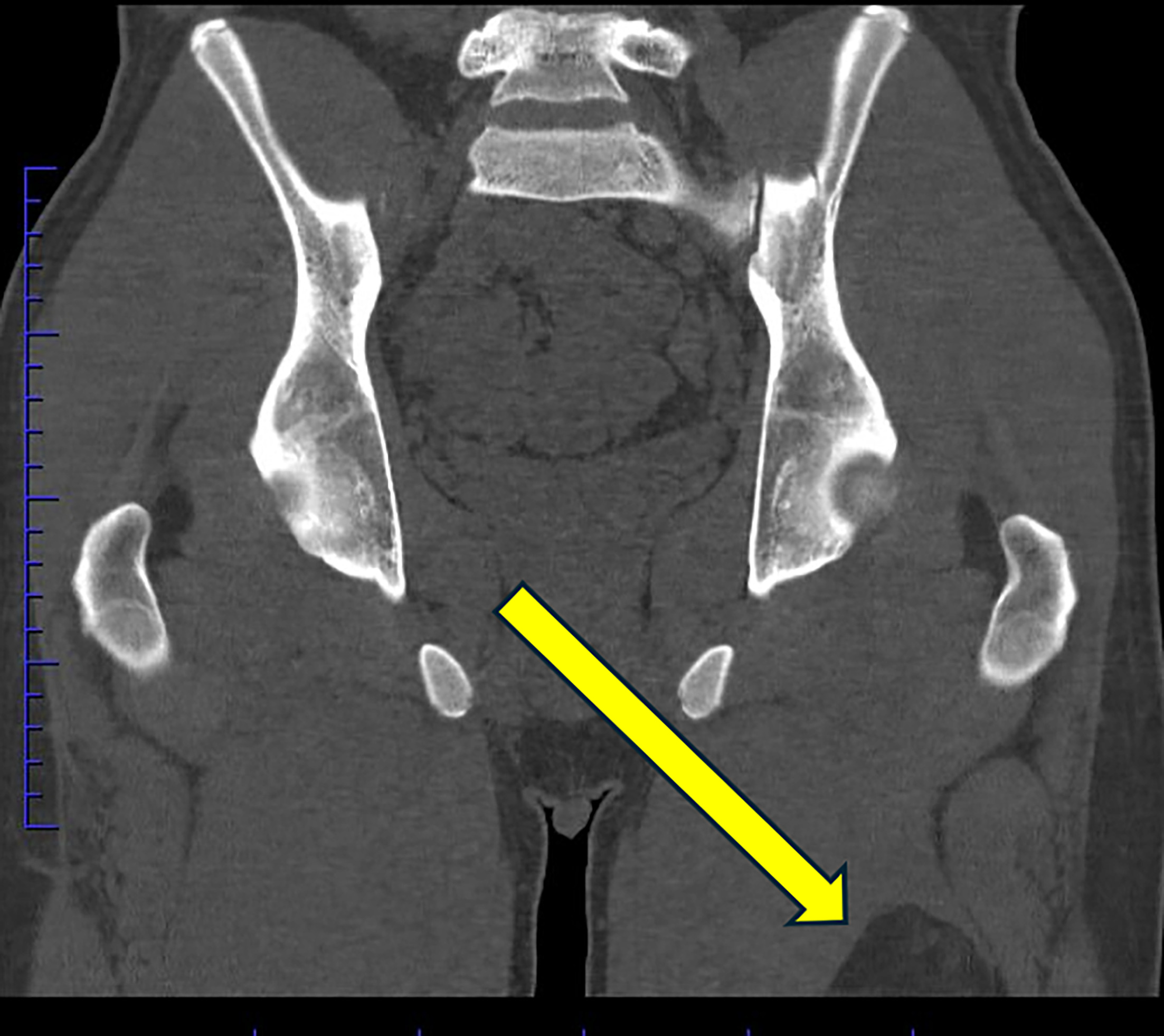
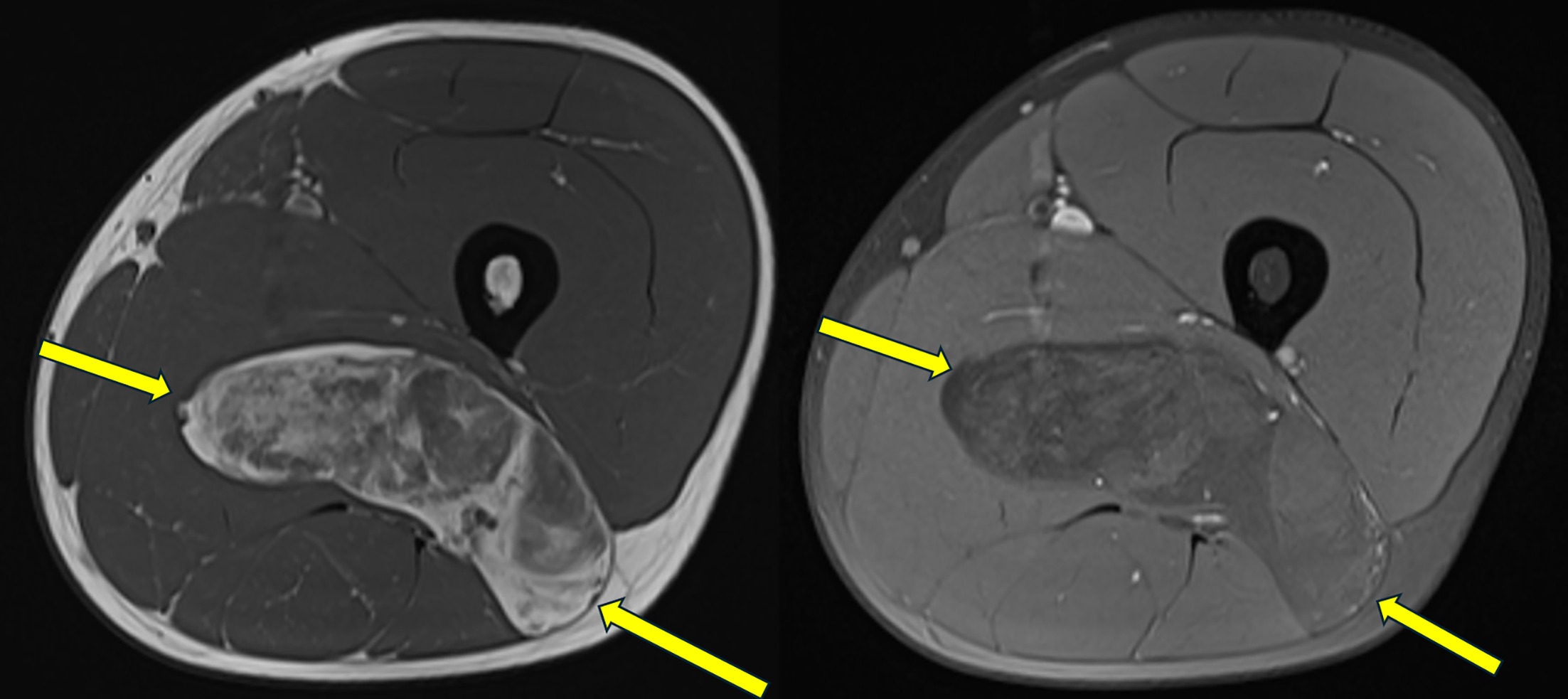
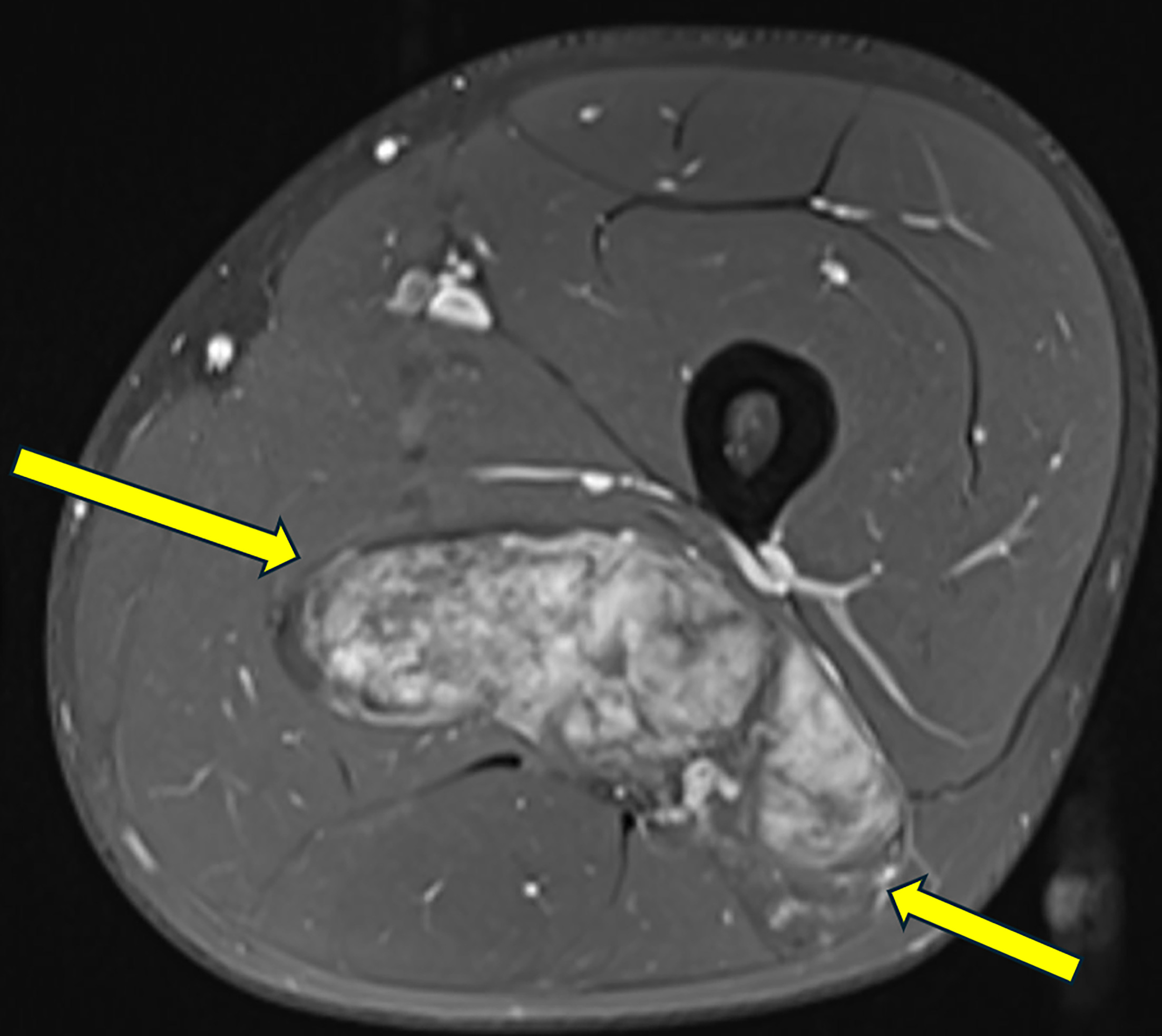
The noncontrast CT of the pelvis did not demonstrate any osseous abnormalities, but a fat density mass was partially included in the field of view (Figure 1). A subsequent MRI was undertaken, showing a fatty mass with heterogeneous internal signal intensity and enhancement (Figures 2, 3). A biopsy confirmed the diagnosis of a liposarcoma of the left lower extremity.
Diagnosis
Liposarcoma of the lower extremity.
The differential diagnoses based on imaging findings include lipoma, lipoblastoma, lipofibromatosis, and fibrous hamartoma of infancy. The latter 3 fat-containing masses typically present in children younger than 3 years of age. Patients with liposarcomas are older, typically diagnosed after 10 years of age. 1
Discussion
Liposarcomas are the second most common soft-tissue tumor, 2 second to only lipomas. 3 However, they are rare tumors diagnosed with an incidence of 1.08 per 100,000 person-years in the United States. 4 The tumors are malignancies derived from primitive mesenchymal cells that undergo adipose differentiation. 2 Patients are most commonly diagnosed in the 5th or 6th decades of life. However, they can also occur in childhood, where liposarcoma represents approximately 2% of all childhood sarcomas. 5 Overall, 60% of patients with liposarcoma are males and greater than 80% are Caucasian. 4
There are 5 major histological subtypes of liposarcoma: well-differentiated, dedifferentiated, myxoid (including the round cell variant), pleomorphic, and liposarcoma not otherwise specified. 6 The well-differentiated and dedifferentiated subtypes account for 45% of tumors. These subtypes frequently exhibit amplifications of the MDM2 and CDK4 genes. The myxoid subtype accounts for approximately 35% of tumors and is associated with a t (12;16) (q13; p11) translocation, creating the FUS-CHOP fusion gene. This subtype comprises the majority of cases in the pediatric population. 7 Pleomorphic liposarcomas account for 5% of liposarcomas and mainly occur in older populations. They are associated with a wide variety of translocations, the most common of which is 13q-14.2-q14.3, which knocks out the RB1 tumor suppressor gene. 8
Liposarcomas most frequently occur in the lower extremities or retroperitoneum. 2 When the lower extremity is affected, the tumor generally arises proximally, within the thigh. 1 Patients with lower extremity liposarcomas present with a slow-growing mass that may be associated with pain, localized swelling, and focal neurologic deficits. When the tumor originates in the retroperitoneum, it typically presents late with a large size due to the large volume the retroperitoneal space offers for unnoticed slow growth, with the average size being over 20 cm when discovered. 9 They can present with nonspecific symptoms, including abdominal pain, early satiety, lower extremity swelling, or obstructive organ symptoms from mass effect or local tissue invasion. 9
The different histologic subtypes have different appearances on MRI. 2,10,11 However, while there are features characteristic of each subtype, biopsy is required for diagnosis. Well-differentiated liposarcomas are predominantly fat-containing tumors. However, up to 25% of the tumor may comprise soft-tissue septations or nodules. 11 These septations enhance after the administration of intravenous contrast. It can be difficult to distinguish a well-differentiated liposarcoma from a lipoma. Features that favor malignancy include septations thicker than 2 mm, size larger than 10 cm, calcifications, and soft-tissue enhancement. 11 De-differentiated liposarcomas occur within a well-differentiated liposarcoma. Thus, they appear like a well-differentiated tumor. 11 Dedifferentiated tumors are distinguished on imaging by the presence of a soft-tissue nodule larger than 1 cm. 11 Myxoid liposarcomas appear as well-defined, multilobular, intramuscular tumors. 11 The tumors appear hypointense on T1-weighted images and hyperintense on T2-weighted images due to the high myxoid component. 11 The tumors contain foci of intratumoral fat within its septations or intratumoral nodules. 11 Pleomorphic liposarcomas have irregular infiltrative margins. On MRI, the tumors may only have small foci of fat. Because they predominantly comprise soft tissue, they have heterogeneous low signal on T1-weighted images and heterogeneous high signal on T2-weighted images. 2
Liposarcomas of the extremities are treated via surgical excision with wide margins, although radiation therapy has proven to be effective in some cases. 6,8 The 5-year survival rates vary with the subtype. One large retrospective study demonstrated that pleomorphic liposarcomas have the worst prognosis with a 47.6% 5-year survival rate. 12 Patients with other subtypes of liposarcoma fare better with increasing 5-year survival rates in de-differentiated tumors (54.4%), followed by the myxoid (79.7%) and well-differentiated (92.4%) subtypes. 12 The 5-year survival rates are negatively correlated with metastatic potential for each tumor subtype. 12 They have been recorded to most commonly metastasize to the lungs, liver, and other soft tissues. 13
Conclusion
Liposarcomas are the second most common soft-tissue tumor and primarily occur within the proximal lower extremity and the retroperitoneum. There are 5 different subtypes of tumor. While there are unique imaging features of each subtype, biopsy is required for diagnosis. Surgical excision remains the primary treatment option for all subtypes of lower extremity liposarcomas.
References
- Navarro O. Pearls and pitfalls in the imaging of soft-tissue masses in children. Semin Ultrasound CT MR. 2020;41(5):498-512. doi:10.1053/j.sult.2020.05.014.
- Barile A, Zugaro L, Catalucci A. Soft tissue liposarcoma: histological subtypes, MRI and CT findings. Radiol Med (Torino). 2002;104(3):140-149.
- Johnson C, Ha A, Chen E, Davidson D. Lipomatous soft-tissue tumors. J Am Acad Orthop Surg. 2018;26(22):779-788. doi:10.5435/JAAOS-D-17-00045.
- Bock S, Hoffmann D, Jiang Y, Chen H, Il’yasova D. Increasing incidence of liposarcoma: a population-based study of national surveillance databases, 2001-2016. Int J Environ Res Public Health. 2020;17(8). doi:10.3390/ijerph17082710.
- Huh W, Yuen C, Munsell M. Liposarcoma in children and young adults: a multi-institutional experience. Pediatr Blood Cancer. 2011;57(7):1142-1146. doi:10.1002/pbc.23095.
- Manji G, Schwartz G. Managing liposarcomas: cutting through the fat. J Oncol Pract. 2016;12(3):221-227. doi:10.1200/JOP.2015.009860.
- Quaglia M, Spiro S, Ghavimi F. Liposarcoma in patients younger than or equal to 22 years of age. Cancer. 1993;72(10):3114-3119. doi:10.1002/1097-0142(19931115)72:103.0.co;2-i.
- Conyers R, Young S, Thomas D. Liposarcoma: molecular genetics and therapeutics. Sarcoma. 2011;2011. doi:10.1155/2011/483154.
- Vijay A, Ram L. Retroperitoneal liposarcoma: a comprehensive review. Am J Clin Oncol. 2015;38(2):213-219. doi:10.1097/COC.0b013e31829b5667.
- El Ouni F, Jemni H, Trabelsi A. Liposarcoma of the extremities: MR imaging features and their correlation with pathologic data. Orthopaedics & Traumatology: Surgery & Research. 2010;96(8):876-883. doi:10.1016/j.otsr.2010.05.010.
- Murphey M, Arcara L, Fanburg-Smith J. Imaging of musculoskeletal liposarcoma with radiologic-pathologic correlation. Radiographics. 2005;25(5):1371-1395. doi:10.1148/rg.255055106.
- Vos M, Koseła-Paterczyk H, Rutkowski P. Differences in recurrence and survival of extremity liposarcoma subtypes. Eur J Surg Oncol. 2018;44(9):1391-1397. doi:10.1016/j.ejso.2018.03.028.
- Muratori F, Bettini L, Frenos F. Myxoid liposarcoma: prognostic factors and metastatic pattern in a series of 148 patients treated at a single institution. Int J Surg Oncol. 2018;2018. doi:10.1155/2018/8928706.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Liposarcoma of the Lower Extremity. Applied Radiology. 2025. doi:10.37549/JPCR-25-0029.