1 University of Arizona College of Medicine, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 University of Cincinnati College of Medicine, Cincinnati, Ohio
4 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Little league shoulder (LLS) and biceps tendonitis are both overuse injuries that are common in young athletes. LLS presents as insidious onset shoulder pain with arm flexion, point tenderness over the physis, and limited range of motion. It is best seen on radiography as widening of the physis. Biceps tendonitis presents similarly, but there is pain at rest and the point tenderness is located over the long head biceps tendonitis. Both conditions are treated supportively with rest, physical therapy, and gradual return to activity.
Keywords
sports injury, shoulder
Categories
Case Summary
A teenage boy was pitching during baseball practice and experienced acute anterior right upper extremity pain. There was no specific pitch noticed with onset, but the patient had to end practice and rest his arm for pain relief. He presented to the emergency department (ED) 2 days later for evaluation. On examination, there was pain over the proximal humeral head with biceps flexion. Swelling and point tenderness were absent. His father commented that the patient had not been using proper throwing techniques during the practice. Radiographs of the humerus were obtained, and the patient followed up with an orthopedic surgery clinic visit 4 days later.
Imaging Findings
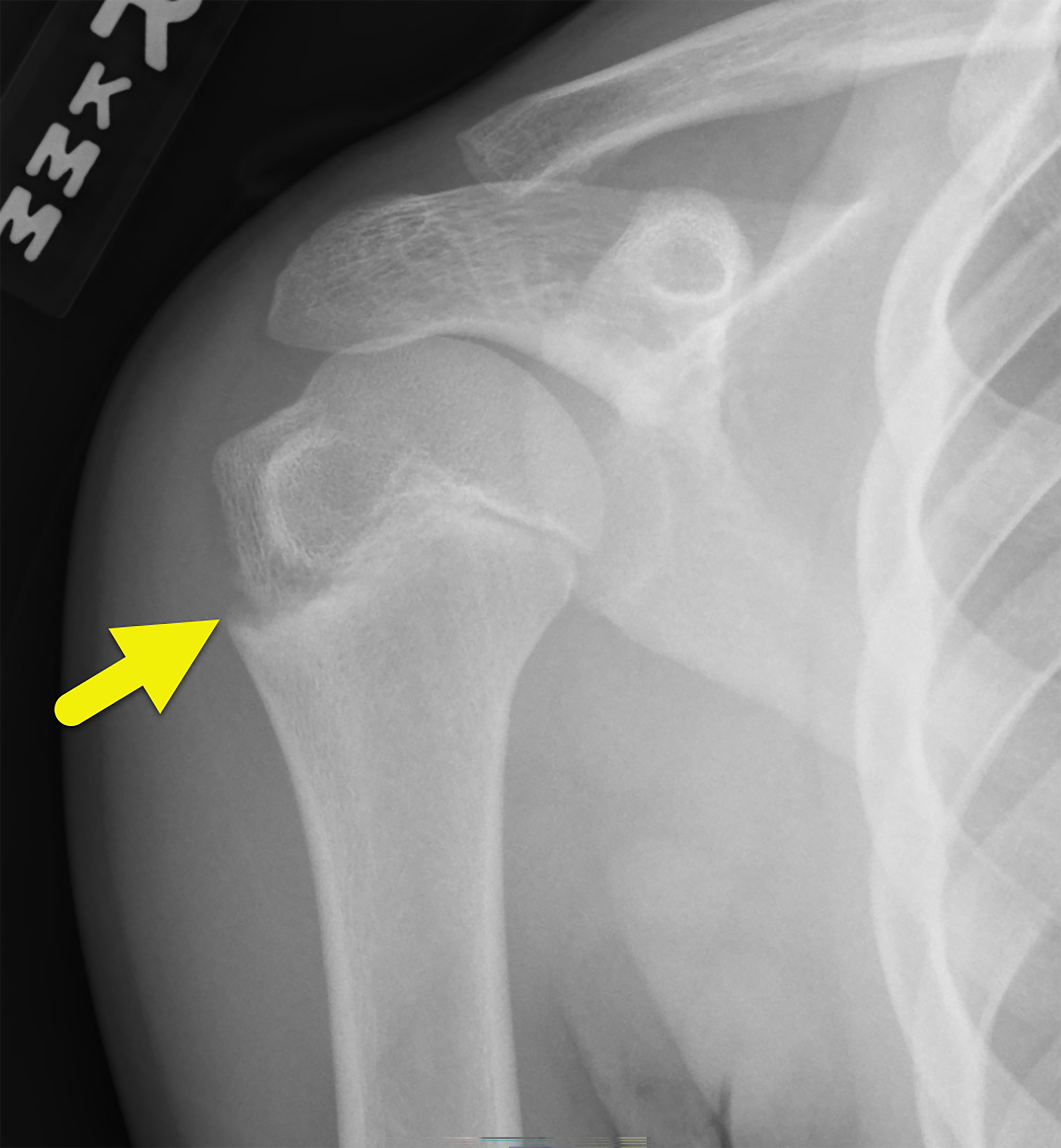
Frontal radiograph of the right humerus of a different patient was taken in the ED. Fractures were absent and soft tissues appeared normal. There was mild irregularity of the lateral aspect of the proximal right humeral physis with apparent physeal widening.
Diagnosis
Little league shoulder (LLS).
The differential diagnosis is biceps tendonitis (BT).
Discussion
The biceps brachii is one of the strongest muscles of the upper extremity. It is biarticular, spanning from the scapula to the radius and crossing both the shoulder and elbow joints. It has 2 tendinous heads named by their length. The short head originates at the coracoid process and descends into the muscle body. The long head biceps tendonitis (LHBT) originates at the supraglenoid tubercle of the scapula and superior labrum. It encircles the humeral head and descends through the bicipital groove before joining the muscle body. 1
The muscle’s positioning allows it to be a powerful elbow flexor and forearm supinator. Although controversial, some studies have suggested that it also helps stabilize the anterior shoulder, particularly during the first 30° of shoulder flexion. 2 These actions make the biceps indispensable in overhead throwing biomechanics.
This patient was diagnosed with LLS. Also known as proximal humeral epiphysiolysis, LLS is an overuse injury at the proximal humeral physis that occurs when rotational torque forces during the cocking phase of throwing exceed the protective distraction force provided by the rotator cuff muscles. LLS occurs only in skeletally immature athletes and is common in young baseball players. One study of 2055 baseball players aged 9-12 found that 13.4% reported pain in their throwing arm. Of these, 41 patients received a radiological workup and 36.6% of them had LLS. 3 Altered throwing mechanics predisposes to LLS. Glenohumeral internal rotation deficit (GIRD), a condition characterized by decreased rotational range of motion at the shoulder, is associated with a 3 times increased risk for LLS. 3
LLS most commonly presents as insidious onset shoulder pain and fatigue associated with overhead activities. Pain may also be referred to the elbow. Examination often shows tenderness over the lateral aspect of the proximal humerus with decreased range of motion and muscle weakness. Swelling of the lateral shoulder may also be present. 4 On radiography, the physis may appear normal or widened with sclerosis and fragmentation of the adjacent bone (Figure 1). It is treated with 3-6 months of rest and physical therapy. 5 Most patients recover completely, but symptom recurrence happens in 7% of cases with an average onset of 4.2 months after returning to activity. Patients with GIRD are 3.6 times more likely to experience recurrence. 6
BT and LLS can be difficult to distinguish between. BT is an inflammatory condition most commonly affecting the LHBT as it travels within the restricting bicipital groove. BT ranges from an acute inflammatory episode to chronic degenerative tendinopathy.
In most adult patients, BT is associated with concomitant shoulder pathologies, such as rotator cuff tendonitis and acromioclavicular joint impingement. However, in young athletes it often exists in isolation. The inflammation occurs in response to repetitive traction, friction, and shoulder rotation. As the tendon swells, it becomes further compressed within the bicipital groove, which can eventually lead to sheath thickening, fibrosis, and vascular compromise. In advanced stages, the tendon loses its mobility and can rupture. 7
Like LLS, BT presents with insidious onset shoulder pain that is worsened by overhead activities. However, the pain often worsens at night and may radiate down the arm. Point tenderness is located characteristically over the bicipital groove. Although the range of motion is not affected until late in the disease course, instability of the tendon may cause a palpable snap with arm movement. Radiography is the initial imaging but will be normal in most cases as is the case with this patient. US may show tendon sheath thickening or surrounding fluid but has variable sensitivity. MRI is the most sensitive imaging examination and reveals high T2 fluid signal intensity surrounding a thickened tendon. MRI also has the benefit of demonstrating concomitant shoulder pathologies. 8 The initial management is nonsurgical with rest and anti-inflammatory analgesics.
Over time, there has been increased pressure on children to participate in organized sports at a higher level, specialize in a single sport early on, and play multiple consecutive seasons to boost their standing. Between 1997 and 2016, the number of children aged 6-18 participating in sports has increased by 15 million. Of the 60 million total youth athletes in America, 27% play only one sport. 9 This increased intensity has led to more overuse injuries, overtraining, and burnout. The American Academy of Pediatrics has published recommendations for reducing overuse injuries, which include taking regular time off, early diversification in sports, and later specialization in a single sport.
Conclusion
LLS and BT are both overuse injuries that are common in young athletes. LLS presents as insidious onset shoulder pain with arm flexion, point tenderness over the physis, and limited range of motion. It is best seen on radiography as widening of the physis. BT presents similarly, but there is pain at rest and the point tenderness is located over the LHBT. Both conditions are treated supportively with rest, physical therapy, and gradual return to activity.
References
- Feger J. Radiopaedia.Org. 2021. doi:10.53347/rID-95439.
- Varacallo M, Seaman T, Mair S. StatPearls. 2022.
- Casadei K, Kiel J. StatPearls. 2022.
- Watkins R, De Borja C, Ramirez F. Common upper extremity injuries in pediatric athletes. Curr Rev Musculoskelet Med. 2022;15(6):465-473. doi:10.1007/s12178-022-09784-1.
- Bell D, Iqbal S. Radiopaedia.Org. 2020. doi:10.53347/rID-79423.
- Heyworth B, Kramer D, Martin D. Trends in the presentation, management, and outcomes of little league shoulder. Am J Sports Med. 2016;44(6):1431-1438. doi:10.1177/0363546516632744.
- Varacallo M, Mair S. StatPearls. 2022.
- El-Feky M, Ebouda F. Radiopaedia.Org. 2019. doi:10.53347/rID-68090.
- Brenner J. Sports specialization and intensive training in young athletes. Pediatrics. 2016;138(3). doi:10.1542/peds.2016-2148.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Little League Shoulder. Applied Radiology. 2025. doi:10.37549/JPCR-25-0024.