1 Rowan College of Osteopathic Medicine, Stratford, New Jersey
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Meconium ileus is a mechanical obstruction of the small bowel and is often the first clinical manifestation of cystic fibrosis in the neonatal period. Affected neonates typically present with abdominal distention and failure to pass meconium within the first 48 hours of life. Diagnosis relies on a combination of imaging modalities, including radiographs and US, as well as confirmatory testing for cystic fibrosis through genetic and sweat chloride analysis. Management begins with hyperosmolar contrast enemas, which can be both diagnostic and therapeutic, while surgical intervention is reserved for complicated cases or when enema fails to resolve the obstruction.
Keywords
bowel obstruction, neonate, therapeutic enema
Categories
Case Summary
A 1-day-old newborn presented with failure to pass meconium. Both parents were known to carry a gene for cystic fibrosis.
Imaging Findings
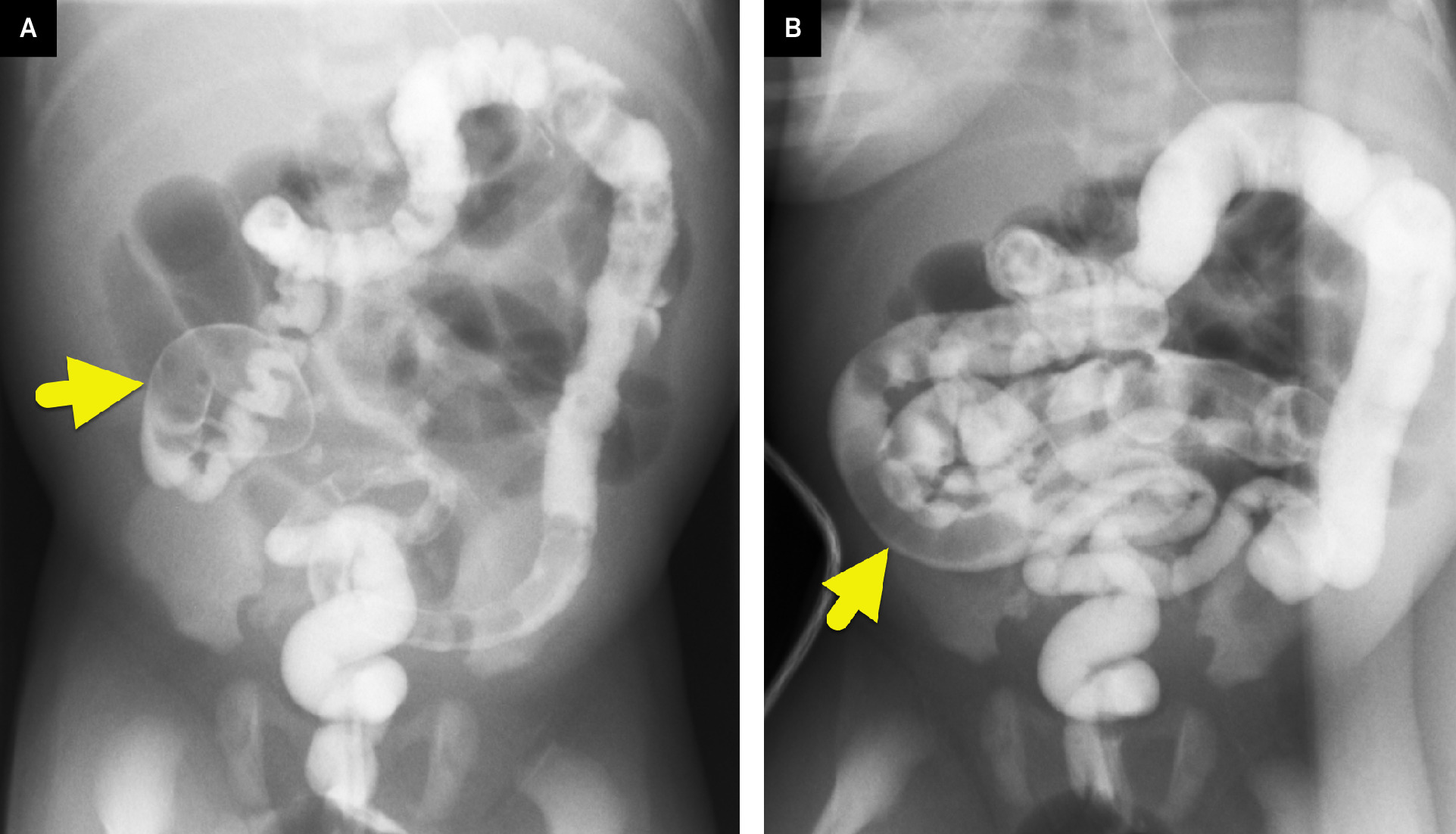
Abdominal radiograph (Figure 1) showed findings of a distal bowel obstruction with dilated air-filled loops of small bowel. Water-soluble contrast enema (Figure 2) showed a small-caliber colon with filling defects in the terminal ileum.

Diagnosis
Meconium ileus.
The differential diagnosis for a neonate who fails to pass meconium includes Hirschsprung’s disease, bowel atresia, and meconium plug syndrome.
Discussion
Meconium ileus is a rare cause of neonatal intestinal obstruction, resulting from inspissated meconium within the terminal ileum. 1 The condition arises due to abnormal intestinal secretions, leading to a dehydrated environment in the gut lumen and the formation of thick, sticky meconium that obstructs the bowel. 1 Meconium ileus is associated with cystic fibrosis, occurring in 12-20% of neonates with the disease, and is often the first clinical manifestation of cystic fibrosis in the neonatal period. 1 Importantly, the presence of meconium ileus does not confer a worse prognosis for neonates with cystic fibrosis compared with those without meconium ileus. 2 The condition affects both sexes, with a slight female predominance (55% female vs 45% male).
Meconium ileus can be broadly categorized into 2 forms: simple and complicated. In simple meconium ileus, neonates typically present with failure to pass meconium within the first 48 hours of life, accompanied by proximal small bowel dilation due to obstruction. 1 Clinical signs often include abdominal distention, feeding intolerance, and bilious emesis. 3 Complicated meconium ileus presents similarly but is associated with hemodynamic instability and additional findings such as volvulus of the affected ileal segment, intestinal atresia, ischemic necrosis, meconium cyst formation, and meconium peritonitis. 2,3
Imaging typically begins with thoracoabdominal radiographs to assess for signs of bowel obstruction. 1 Radiographs may demonstrate dilated bowel loops and a characteristic “soap-bubble” appearance (Newhauser sign) in the right lower quadrant, caused by gas trapped within the inspissated meconium. 4 . In simple meconium ileus, water-soluble contrast enema is the diagnostic study of choice, revealing a microcolon with multiple intraluminal filling defects in the ileum due to impacted meconium pellets. 4 If malrotation with midgut volvulus is suspected, an upper gastrointestinal series can be performed for further evaluation. 5 In complicated meconium ileus, abdominal radiographs may demonstrate peritoneal calcifications, while US can reveal the calcifications, dilated small bowel loops, and potentially a meconium pseudocyst.
A water-soluble contrast enema is both diagnostic and therapeutic in meconium ileus. For simple meconium ileus, hyperosmolar contrast enemas administered under fluoroscopic guidance help draw fluid into the bowel lumen to soften and evacuate the inspissated meconium. 5 If the obstruction resolves, additional saline enemas and follow-up abdominal radiographs are recommended to ensure complete clearance. 5 Hyperosmolar enemas can be safely repeated if needed. However, if the enemas are unsuccessful or if complicated meconium ileus is present, surgical intervention is typically required. 5
When imaging confirms meconium ileus, genetic testing and sweat chloride testing are performed to confirm the diagnosis of cystic fibrosis. 1 While simple meconium ileus generally resolves without long-term sequelae, patients remain at risk for complications related to cystic fibrosis. One such complication is distal intestinal obstruction syndrome (DIOS), which is considered a meconium ileus equivalent. 6 Like meconium ileus, DIOS results from inspissated intestinal contents, causing obstruction. DIOS occurs in 7-20% of patients in their lifetime, with a peak between 6 and 10 years of age. Lavie and colleagues found that patients with DIOS had 2 prominent mutations (DeltaF508 and W1282X0). 7 Management is similar, typically involving hyperosmolar water-soluble contrast enemas to relieve the obstruction.
Conclusion
Meconium ileus is a mechanical obstruction of the small bowel and is often the first clinical manifestation of cystic fibrosis in the neonatal period. Affected neonates typically present with abdominal distention and failure to pass meconium within the first 48 hours of life. Diagnosis relies on a combination of imaging modalities, including radiographs and US, as well as confirmatory testing for cystic fibrosis through genetic and sweat chloride analysis. Management begins with hyperosmolar contrast enemas, which can be both diagnostic and therapeutic, while surgical intervention is reserved for complicated cases or when enema fails to resolve the obstruction.
References
- Donos M, Ghiga G, Trandafir L. Diagnosis and management of simple and complicated meconium ileus in cystic fibrosis, a systematic review. Diagnostics (Basel). 2024;14(11). doi:10.3390/diagnostics14111179.
- Tobias J, Tillotson M, Maloney L, Fialkowski E. Meconium ileus, distal intestinal obstruction syndrome, and other gastrointestinal pathology in the cystic fibrosis patient. Surg Clin North Am. 2022;23(1):873-882. doi:10.3348/kjr.2021.0111.
- Carlyle B, Borowitz D, Glick P. A review of pathophysiology and management of fetuses and neonates with meconium ileus for the pediatric surgeon [published correction appears in J Pediatr Surg 2012 Aug;47(8):1633]. J Pediatr Surg. 2012;47(4):772-781. doi:10.1016/j.jpedsurg.2012.02.019.
- Choi G, Je B, Kim Y. Gastrointestinal emergency in neonates and infants: a pictorial essay. Korean J Radiol. 2022;23(1):124-138. doi:10.3348/kjr.2021.0111.
- Sathe M, Houwen R. Meconium ileus in cystic fibrosis. J Cyst Fibros. 2017;16 Suppl 2(suppl 2):S32-S39. doi:10.1016/j.jcf.2017.06.007.
- Parikh N, Ibrahim S, Ahlawat R. StatPearls. 2023.
- Lavie M, Manovitz T, Vilozni D. Long-term follow-up of distal intestinal obstruction syndrome in cystic fibrosis. World J Gastroenterol. 2015;21(1):318-325. doi:10.3748/wjg.v21.i1.318.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Meconium Ileus. Applied Radiology. 2025. doi:10.37549/JPCR-25-0028.