Metastatic Neuroblastoma
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -3
Published: September 1, 2025
1 Quillen School of Medicine, East Tennessee University, Johnson City, Tennessee
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Categories
Case Summary
A middle-childhood youngster with known neuroblastoma presented to the emergency room with right eye swelling. An orbital CT was performed.
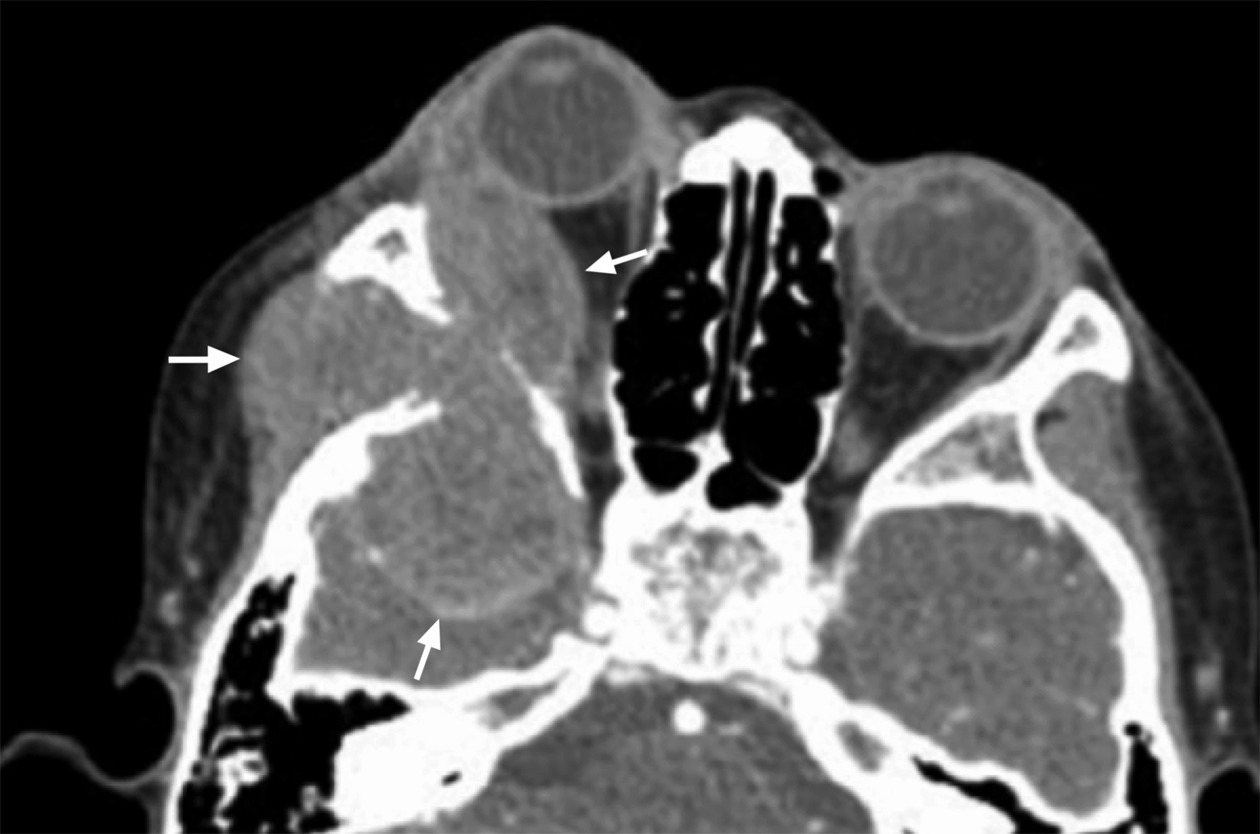
Imaging Findings
A blowout lesion of the right lateral orbital wall with permeative bone changes, a soft-tissue mass extending into the lateral temporal soft tissue, bony orbit, and middle cranial fossa (Figure 1). This pattern of metastasis is distinctive and indicative of a bone marrow origin.
Diagnosis
Neuroblastoma with orbital metastasis.
In pediatric patients, permeative destruction of the bone on 3 sides of the lateral orbit indicates an aggressive condition that originates in the marrow cavity. The differential diagnosis includes neuroblastoma, rhabdomyosarcoma, retinoblastoma, Langerhans cell histiocytosis (LCH), non-Hodgkin lymphoma, and Ewing sarcoma.
Discussion
In pediatric populations, lytic bone lesions of the orbital wall can indicate metastases from several malignancies that spread hematogenously to the bone marrow (Figure 1). The frequency of bone marrow metastasis to the orbital bone is highest in neuroblastoma (10-20%), 1,2 rhabdomyosarcoma (10%), 3 retinoblastoma (6.3-7.6%), 4 and non-Hodgkin lymphoma (3-9%). 3 Of note, LCH is non-neoplastic and features primary or metastatic orbital bone involvement in 20-37.5% of cases. 5 When isolated, LCH can have a favorable outcome. In rare cases, Ewing sarcoma can also metastasize to this area. It is also important to recognize that orbital metastases indicate a high degree of disease severity and, in most instances, a poor prognosis.
Neuroblastoma is caused by pathologic neural crest cell derivatives and is associated with primary malignancy and metastasis to the facial bones and periorbital calvarium (which are also partially derived from neural crest cells). 6 Neuroblastoma has a few characteristic symptoms, including proptosis, periorbital ecchymoses (“raccoon eyes”), and opsoclonus-myoclonus syndrome (“dancing eyes, dancing feet”). 3 The imaging findings of metastatic neuroblastoma, and the group of small blue round cell tumors, are bone marrow metastasis with permeative bone destruction on all sides of the bone with adjacent soft-tissue masses. 6 The lesion most frequently localizes to the posterolateral region of the orbit at the junction of the frontal bone and greater wing of the sphenoid bone. 6 The mass also frequently appears bilaterally. 6 The metastases may also appear circumscribed or poorly defined, are increased in attenuation compared to muscle, can feature small calcific foci, and can invade adjacent structures (including intracranially) on CT and MRI. 3 The presence of aggressive spiculated periosteal reactions (with a “hair on end appearance”) around the orbits is another characteristic finding on x-ray or CT. 7 On MRI, lesions are low intensity on T1-weighted images (T1WI), heterogeneous on T2-weighted images (T2WI) due to hemorrhage or necrosis, and heterogeneously enhance with contrast. 3 The most useful study for diagnosis, staging, and monitoring of treatment of metastatic neuroblastoma is radioiodinated metaiodobenzylguanidine (MIBG) scintigraphy. PET/CT has also been shown to successfully stage and monitor disease with improved spatial resolution compared with MIBG scintigraphy for structural mapping for surgical planning. 3
Rhabdomyosarcoma is a soft-tissue sarcoma derived from mesenchymal stem cells with 2 major subtypes in the orbit: the more aggressive, less common alveolar subtype and the less aggressive, more common embryonal subtype. 3 The most common sites for metastases are the lungs and bone, so a CT of the chest is often indicated to evaluate for pulmonary metastases. Most commonly, the alveolar subtype localizes to the inferior aspect of the orbit and the embryonal subtype localizes to the superomedial quadrant of the orbit. 3 CT and MRI are often used complementarily in evaluating the extent of the disease. On non-contrast CT imaging, rhabdomyosarcoma is attenuating to muscle. With contrast, the tumor is a markedly enhancing, extraconal, homogeneous, and well-circumscribed mass with calcifications and bone destruction. 3 On MRI , the tumor is isointense to muscle on T1WI, hyperintense on T2WI, and demonstrates moderate to marked enhancement with contrast. 3 The tumor can displace the globe and extraocular muscles but rarely invades these structures. 3
Retinoblastoma is the most common pediatric intraocular tumor that can spread to the orbital wall through the optic nerve in advanced cases. 7 It is derived from the maturing cone precursor cells in the retina and is often due to autosomal-dominant mutations in the Rb gene. Importantly, if bilateral tumors are seen, retinoblastoma should be suspected until proven otherwise and may be associated with trilateral disease (bilateral retinoblastoma plus pineoblastoma). As 95% of retinoblastoma cases have characteristic diffuse calcifications, orbital US is an easy and effective way to confirm the clinical diagnosis of retinoblastoma. 3 CT imaging normally reveals a hyperattenuating mass in the posterior globe with calcifications. 3 When assessing retinoblastoma orbital metastases, MRI of the orbits and brain is often necessary to assess the degree of tumor extension and central nervous system (CNS) infiltration, so it is the preferred imaging modality for retinoblastoma. Retinoblastoma follows the signal intensity of gray matter with tumor hyperintense to vitreous on T1WI and hypointense on T2WI. 3 Tumor lesions can also demonstrate a high level of restricted diffusion on diffusion-weighted images. 3
Lymphoproliferative disease and non-Hodgkin lymphoma rarely manifest in the orbital bone but are most seen in the superotemporal aspect with predilection for the lacrimal gland and extraocular muscles. 3 Metastasis to the orbit is generally a feature of high-grade lymphoma with heterogeneous lesions, no calcifications, and permeative bony destruction on CT imaging. Bilateral lesions are possible and indicate systemic disease. 8 MRI normally reveals hypointense or isointense lesions on T1WI and hyperintense on T2WI. 8 Gadolinium enhancement is seen on T1WI, which is indicative of high cellularity. 8 In many cases, F-18 fluorodeoxyglucose PET (FDG-PET) scans are more useful than conventional imaging methods in detecting these extranodal lymphoma metastases and have a higher sensitivity (86% vs 72%) than CT imaging in detecting distant metastases. 8
LCH is a collection of disorders involving the proliferation of Langerhans cells, the resident tissue macrophage of the skin (also derived from neural crest cells), in both reactive and neoplastic growth patterns. LCH has classically been divided into 3 clinical presentations of the same disorder: eosinophilic granuloma, Hand-Schüller-Christian disease, and Letterer-Siwe disease. Any organ can be involved in this disease process with unifocal or multifocal sites, but bone lesions are the most common site of involvement (80% of patients). 9 LCH of the orbit most commonly involves a unifocal lesion of the superotemporal orbit that presents clinically with proptosis, ptosis, erythema, enlarging palpebral fissures, and pain surrounding the lesion. 3 This is a typical presentation of eosinophilic granuloma. On CT imaging, these lesions manifest as a soft-tissue lesion that destroys and replaces surrounding tissues. It can be well-defined, diffusely homogeneous, and shows moderate enhancement after contrast administration. 3 MRI is a more useful diagnostic tool compared with the normal bright bone marrow signal; it shows hyperintense lesions on T1WI, hypointense lesions on T2WI, and enhancement on T1WI after administration of contrast. 3 Technitium-99 bone scintigraphy and FDG-PET scans have also been used with radiographic skeletal survey to identify extracranial bone involvement. 3 Importantly, LCH of the orbit can lead to increased risk of intracranial CNS involvement. Rarely in later stages of the disease, this can lead to endocrinopathies, like diabetes insipidus and growth hormone deficiency (due to hypothalamic-pituitary involvement), and due to an unknown etiology, focal demyelination causing cerebellar dysfunction and neurocognitive deficits. 5
Ewing sarcoma is another small round blue cell tumor that most commonly presents as a primary tumor in the pelvis, extremities, or ribs but has metastasized to the calvarium and facial bones in 0.5-1% of cases. 10 Rarely, Ewing sarcoma has metastasized to the orbital wall with similar findings to neuroblastoma. 11 Ewing sarcoma presents clinically with a destructive bony lesion with prominent surrounding soft-tissue swelling causing pain. The appearance of this lesion is highly variable but can feature aggressive bone destruction with moth-eaten to permeative processes and a wide transition zone (poor margination) on radiography and CT imaging. 11 Other common features are a periosteal reaction and either lamellated (“onion skin”) or spiculated (sunburst or “hair on end”) structure. MRI is the preferred diagnostic imaging modality as it can reveal bone marrow replacement and cortical destruction with its associated circumferential soft-tissue mass. MRI features include low to intermediate signal on T1WI and heterogeneous high signal on T2WI. 11
Conclusion
In cases of ophthalmic clinical findings, including proptosis, leukocoria, erythema, or periorbital ecchymoses in pediatric patients, radiologists are often the first physicians to make the appropriate diagnosis. Therefore, it is important for radiologists to quickly recognize the differentiating features of these orbital pathologies so that patients can receive rapid access to treatment.
References
- Parija S, Banerjee A. Neuroblastoma presenting as orbital metastasis: case report and review of literature. Journal of Current Oncology. 2020;3(1):44. doi:10.4103/jco.jco_18_19.
- Ahmed S, Goel S, Khandwala M. Neuroblastoma with orbital metastasis: ophthalmic presentation and role of ophthalmologists. Eye (Lond). 2006;20(4):466-470. doi:10.1038/sj.eye.6701912.
- Rao A, Naheedy J, Chen J, Robbins S, Ramkumar H. A clinical update and radiologic review of pediatric orbital and ocular tumors. J Oncol. 2013;2013. doi:10.1155/2013/975908.
- Ali M, Honavar S, Reddy V. Orbital retinoblastoma: present status and future challenges - a review. Saudi J Ophthalmol. 2011;25(2):159-167. doi:10.1016/j.sjopt.2010.10.010.
- Herwig M, Wojno T, Zhang Q, Grossniklaus H. Langerhans cell histiocytosis of the orbit: five clinicopathologic cases and review of the literature. Survey of Ophthalmology. 2013;58(4):330-340. doi:10.1016/j.survophthal.2012.09.004.
- D’Ambrosio N, Lyo J, Young R, Haque S, Karimi S. Common and unusual craniofacial manifestations of metastatic neuroblastoma. Neuroradiology. 2010;52(6):549-553. doi:10.1007/s00234-010-0697-2.
- Joseph A, Guerin J, Eckel L. Imaging findings of pediatric orbital masses and tumor mimics. Radiographics. 2022;42(3):880-897. doi:10.1148/rg.210116.
- Ocular lymphoma: acronyms, overview, epidemiology. Published online December 30, 2022.
- Monsereenusorn C, Rodriguez-Galindo C. Clinical characteristics and treatment of langerhans cell histiocytosis. Hematol Oncol Clin North Am. 2015;29(5):853-873. doi:10.1016/j.hoc.2015.06.005.
- Murphey M, Senchak L, Mambalam P. From the radiologic pathology archives: Ewing sarcoma family of tumors: radiologic-pathologic correlation. Radiographics. 2013;33(3):803-831. doi:10.1148/rg.333135005.
- Howard D, Lund V. Primary Ewing’s sarcoma of the ethmoid bone. J Laryngol Otol. 1985;99(10):1019-1023. doi:10.1017/s0022215100098108.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Metastatic Neuroblastoma. Applied Radiology. 2025;1(1):1-3. doi:10.37549/JPCR-25-0011.