Misdiagnosed High-Grade Undifferentiated Sarcoma Mimicking Infantile Myofibroma: A Case Report
Applied Radiology
Published: January 23, 2026
1 Midwestern University Arizona College of Osteopathic Medicine, Glendale, Arizona
2 Creighton University School of Medicine, Phoenix, Arizona
3 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
* Corresponding author: Soham Bhanvadia (soham.bhanvadia@midwestern.edu)
Abstract
Accurate prenatal diagnosis of fetal masses is challenging due to their varied presentation and the limitations of current imaging modalities, which are typically restricted to obstetric US and non-contrast fetal MRI. We present a case involving a right forearm mass first identified on prenatal US and MRI, which initially appeared benign and was diagnosed as infantile myofibroma following excisional biopsy. However, due to rapid growth and persistent symptoms, the patient ultimately underwent transhumeral amputation, with final pathology revealing a high-grade undifferentiated sarcoma. This case highlights the diagnostic complexity of fetal soft tissue tumors and underscores the importance of maintaining a broad differential, including malignancy, even when imaging and initial pathology suggest a benign process.
Keywords
prenatal imaging, fetal tumor, infantile myofibroma, undifferentiated sarcoma, fetal MRI, diagnostic error, pediatric oncology, prenatal diagnosis, biopsy misdiagnosis, soft tissue tumor
Categories
Case Summary
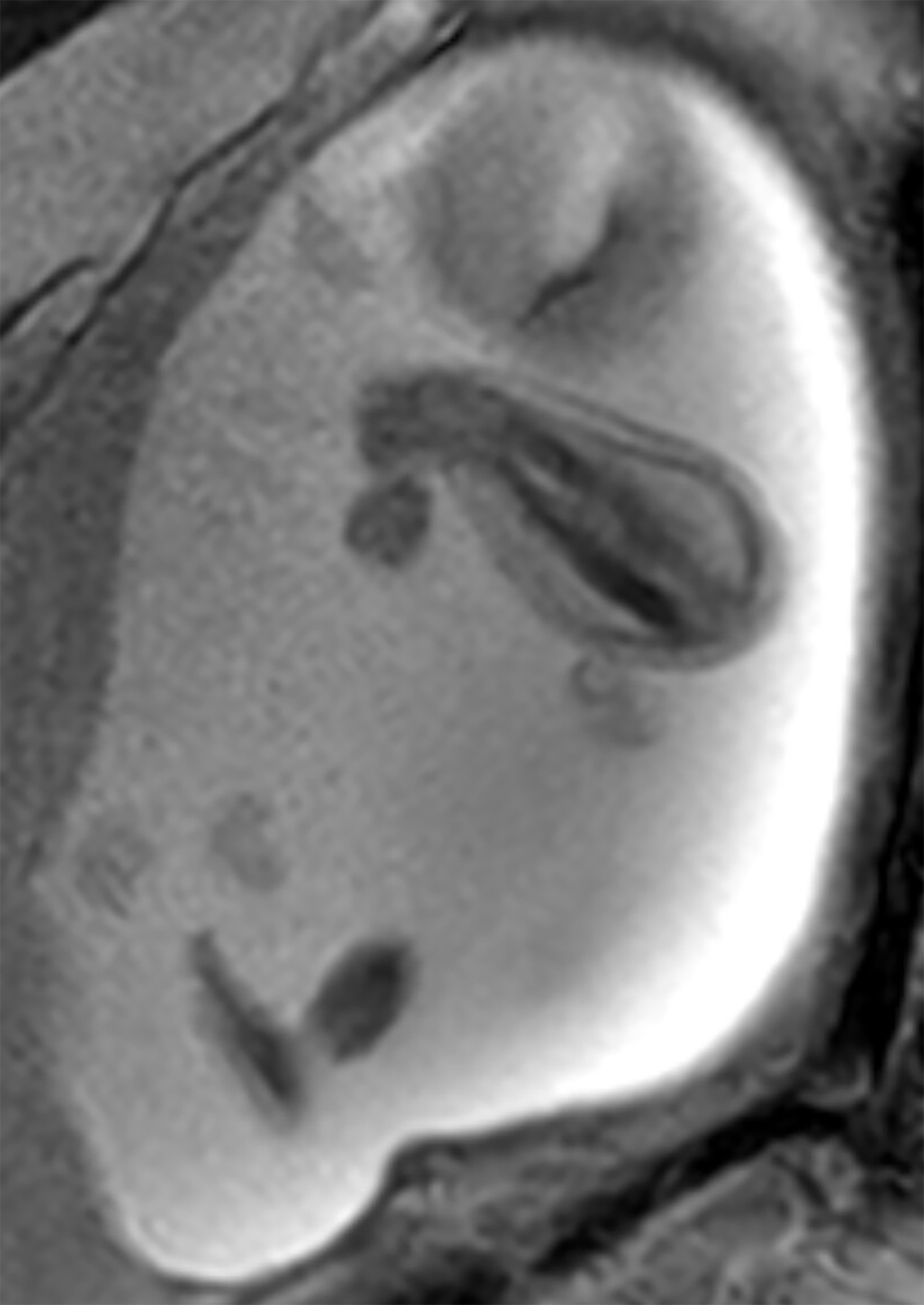
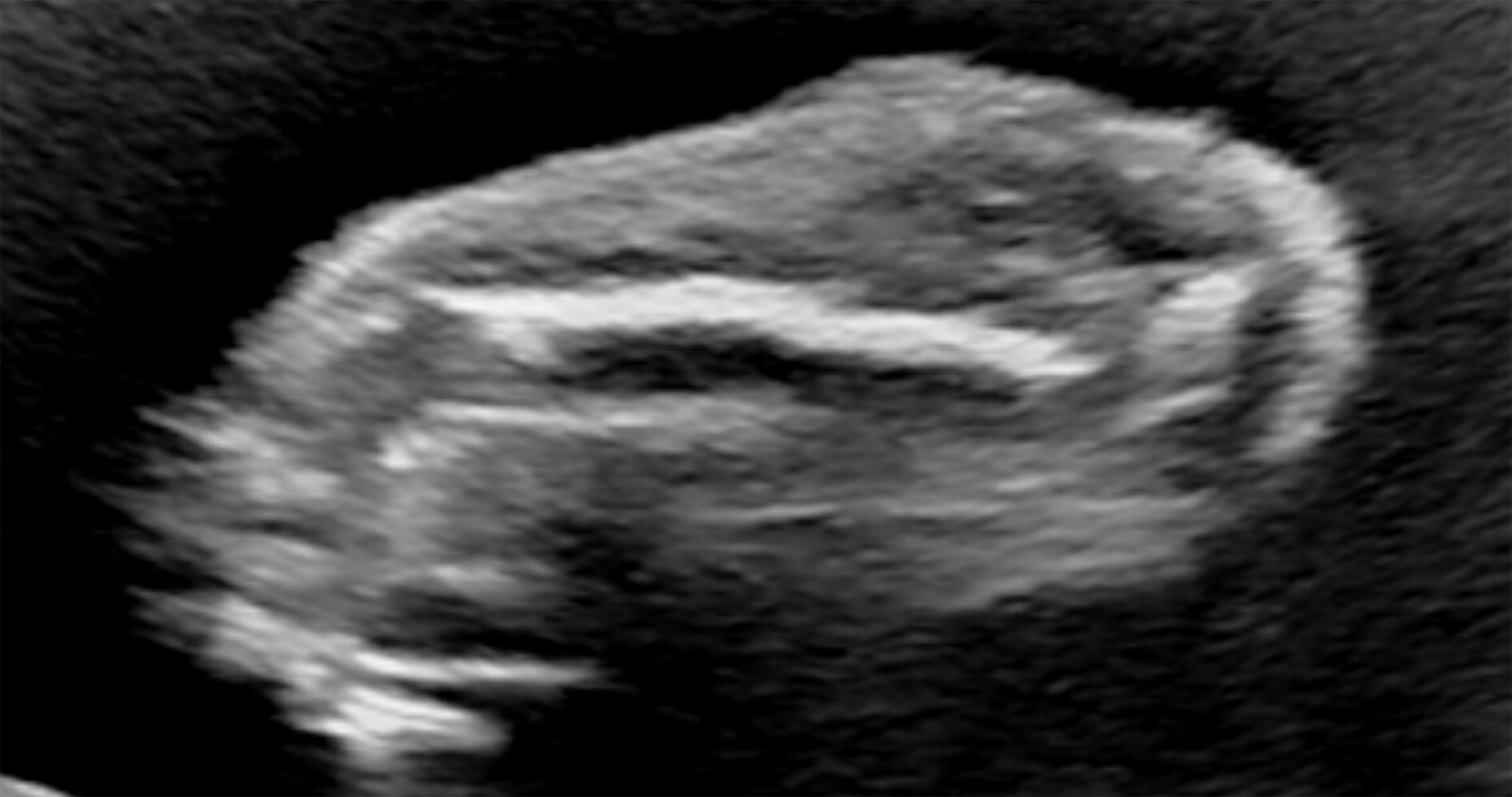
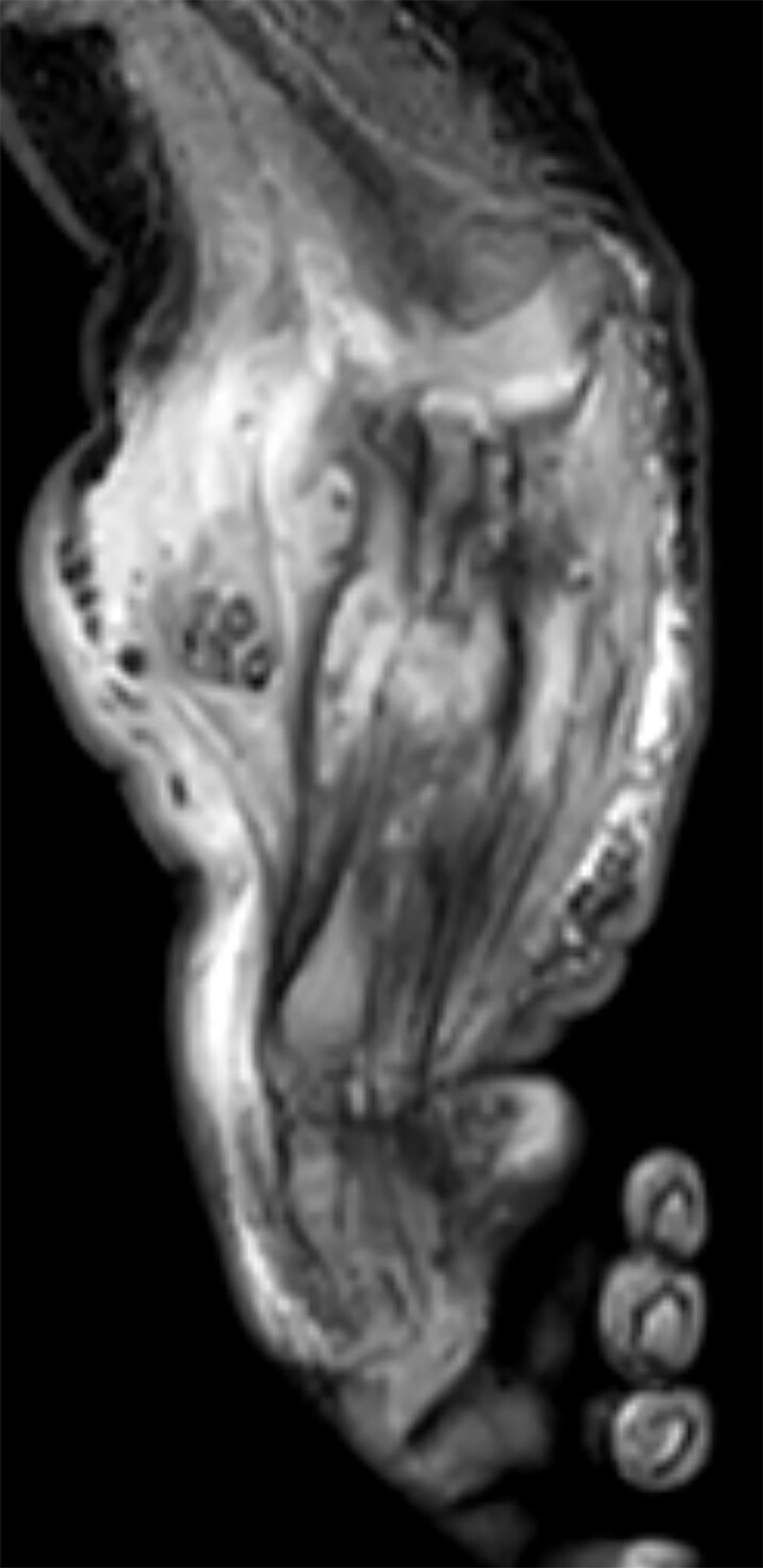
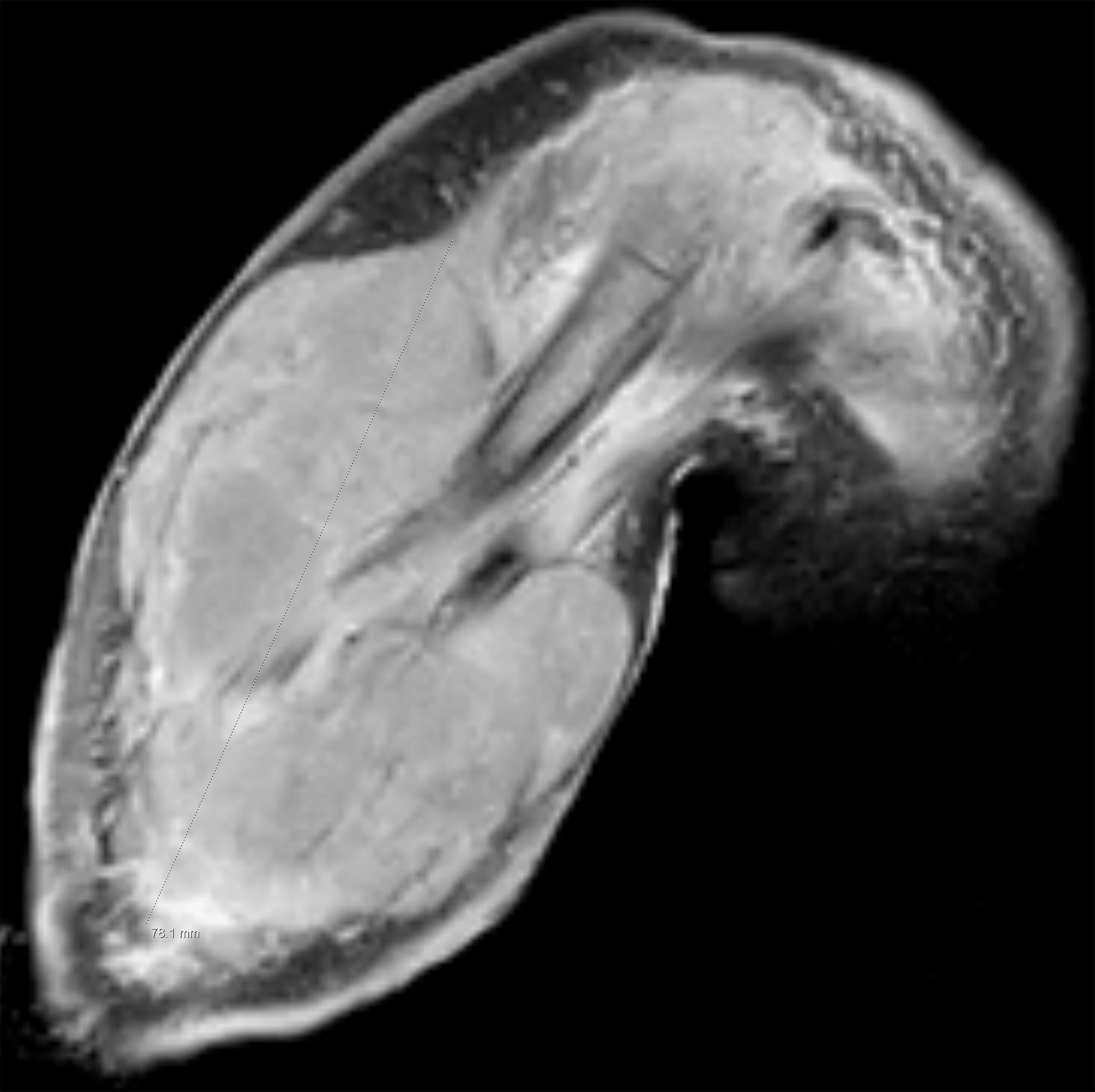
A pregnant adult patient was referred at 20 weeks’ gestation following abnormal anatomy US that revealed an enlarged right arm with clenched fingers. Fetal MRI and US confirmed right forearm enlargement, thickening of the radius and ulna, and dystrophic soft tissue calcifications. The remainder of the exam was unremarkable. At birth via cesarean section, a firm, nodular mass was noted on the right forearm. MRI 4 days after delivery revealed bone remodeling and a hyperintense, heterogeneous soft tissue mass with calcifications and patchy enhancement. An excisional biopsy performed at 6 weeks yielded a diagnosis of infantile myofibroma, and the patient was observed over the next few months. By 4 months, the mass had enlarged and was causing pain and loss of function, necessitating transhumeral amputation. Final pathology demonstrated high-grade undifferentiated sarcoma. At 5 months, the patient developed a recurrence of the mass requiring shoulder disarticulation and is currently undergoing chemotherapy.
Imaging Findings
Fetal MRI (Figure 1) and US (Figure 2) at 22 weeks’ gestation showed enlargement of the right forearm with thickened radius and ulna. The mass appeared hyperintense on T2-weighted sequences. Postnatal MRI on day 4 (Figure 3) demonstrated deformity of the forearm bones and a hyperintense, heterogeneously enhancing mass with calcifications on T2-weighted sequences. At 5 months, MRI (Figure 4) revealed a lobulated, enhancing soft tissue mass surrounding the mid humerus without obvious proximal bony involvement.
Diagnosis
High-grade undifferentiated sarcoma.
Differential diagnoses: venous malformation with phleboliths, macrodystrophia lipomatosa, constriction ring from amniotic band sequence, kaposiform hemangioendothelioma, myofibroma, fibrosarcoma, rhabdomyosarcoma, and osteogenesis imperfecta type V.
Discussion
Diagnosis of prenatal masses presents significant challenges due to variability in presentation, limited imaging modalities (US and non-contrast MRI), and differences between fetal and pediatric tumors.1 Prenatal imaging can guide postnatal management but cannot provide a definitive diagnosis, as fetal tumors differ from pediatric tumors in their biology, growth kinetics, and prognosis.1,2 In this case, prenatal US first identified the abnormality, and fetal MRI was instrumental in further characterizing the lesion, narrowing the differential to entities such as infantile myofibroma, fibrosarcoma, and vascular malformations. Prenatal imaging also guided delivery planning, prompting transfer to a specialized hospital for postnatal MRI and further evaluation of the lesion. Sarcomas, rare in the prenatal period, are malignant connective tissue tumors accounting for about 5% of childhood tumors.3 Undifferentiated sarcoma—a poorly differentiated subtype—is a diagnosis of exclusion and commonly occurs in individuals over 50 and in the lower extremities.4 Prenatal and initial postnatal findings suggested a benign mass due to a lack of invasive features, the presence of dystrophic calcifications, and slow growth.5,6 Initial biopsy findings were consistent with infantile myofibroma, possibly due to overlapping histopathological features with sarcomas such as hypercellularity and infiltrative growth.7,8 Sampling error may also have contributed to the initial misdiagnosis due to the well-documented phenomenon of intratumoral heterogeneity and the dynamic nature of pediatric tissues, which are characterized by ongoing growth and high cellular turnover.9,10 Postnatal progression, including rapid growth and pain, suggested malignancy.
Venous malformation with phleboliths may also present with soft tissue calcifications but typically demonstrates well-delineated phleboliths without associated skeletal anomalies, which were not observed in this case.6 The absence of additional lesions and the localized nature of the mass also lowered suspicion for multifocal or syndromic pathology. Ultimately, the worsening clinical course—marked by increasing pain, functional limitation, and mass progression—necessitated transhumeral amputation.
The diagnosis was confirmed after resection and recurrence, illustrating the limitations of both imaging and single-site biopsies in heterogeneous tumors. Early consideration of malignancy could have prompted earlier definitive treatment and potentially reduced the extent of surgical morbidity.
This case highlights the importance of maintaining malignancy in the differential diagnosis for fetal soft tissue masses, even when imaging and initial pathology appear benign. Improved outcomes rely on advanced imaging techniques, such as diffusion-weighted MRI, magnetic resonance spectroscopy, and total-body MRI, alongside careful multidisciplinary evaluation and clinicopathologic correlation, which together enhance lesion characterization, detect multifocal disease, and guide biopsy to the most diagnostically relevant areas.11-13
Conclusion
This case demonstrates the challenges in diagnosing fetal soft tissue masses and emphasizes the potential for misdiagnosis, particularly when biopsy and imaging findings appear benign. Maintaining a broad differential and monitoring for clinical progression are crucial. Advances in imaging and multidisciplinary collaboration may improve early and accurate diagnosis.
References
- Kamil D, Tepelmann J, Berg C. Spectrum and outcome of prenatally diagnosed fetal tumors. Ultrasound Obstet Gynecol. 2008;31(3):296-302. doi:10.1002/uog.5260.
- Cho J, Lee Y. Fetal tumors: prenatal ultrasonographic findings and clinical characteristics. Ultrasonography. 2014;33(4):240-251. doi:10.14366/usg.14019.
- Miser J, Pizzo P. Soft tissue sarcomas in childhood. Pediatr Clin North Am. 1985;32(3):779-800. doi:10.1016/s0031-3955(16)34836-2.
- Steele C, Pillay N. The genomics of undifferentiated sarcoma of soft tissue: progress, challenges and opportunities. Semin Cancer Biol. 2020;61:42-55. doi:10.1016/j.semcancer.2019.11.009.
- Patel A. Benign vs malignant tumors. JAMA Oncol. 2020;6(9):1488. doi:10.1001/jamaoncol.2020.2592.
- Freire V, Moser T, Lepage-Saucier M. Radiological identification and analysis of soft tissue musculoskeletal calcifications. Insights Imaging. 2018;9(4):477-492. doi:10.1007/s13244-018-0619-0.
- Linos K, Carter J, Gardner J. Myofibromas with atypical features: expanding the morphologic spectrum of a benign entity. Am J Surg Pathol. 2014;38(12):1649-1654. doi:10.1097/PAS.0000000000000270.
- Alaggio R, Bisogno G, Rosato A, Ninfo V, Coffin C. Undifferentiated sarcoma: does it exist? A clinicopathologic study of 7 pediatric cases and review of literature. Hum Pathol. 2009;40(11):1600-1610. doi:10.1016/j.humpath.2009.04.013.
- Palmerini E, Picci P, Reichardt P, Downey G. Malignancy in giant cell tumor of bone: a review of the literature. Technol Cancer Res Treat. 2019;18:1533033819840000. doi:10.1177/1533033819840000.
- Schmelz K, Toedling J, Huska M. Spatial and temporal intratumour heterogeneity has potential consequences for single biopsy-based neuroblastoma treatment decisions. Nat Commun. 2021;12(1):6804. doi:10.1038/s41467-021-26870-z.
- Manisterski M, Benish M, Levin D. Diverse presentation and tailored treatment of infantile myofibromatosis: a single-center experience. Pediatr Blood Cancer. 2021;68(2). doi:10.1002/pbc.28769.
- Masselli G, Vaccaro Notte M, Zacharzewska-Gondek A. Fetal MRI of CNS abnormalities. Clin Radiol. 2020;75(8):640. doi:10.1016/j.crad.2020.03.035.
- Rubesova E, Barth R. Advances in fetal imaging. Am J Perinatol. 2014;31(7):567-576. doi:10.1055/s-0034-1371712.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript, and no part of this article has been previously published elsewhere.
Acknowledgments
Patient confidentiality was maintained according to institutional policy. Written informed consent was not obtained but is encouraged in future similar cases.
Citation
. Misdiagnosed High-Grade Undifferentiated Sarcoma Mimicking Infantile Myofibroma: A Case Report. Applied Radiology. 2026. doi:10.37549/AR-D-25-0096.