Modified Davis Intubated Ureterotomy
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 1, 2026
1 University of Missouri Kansas City, Kansas City, Missouri
2 Phoenix Children’s Hospital, Phoenix, Arizona
3 Children’s Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Patients with ureteral injuries who lack enough tissue to perform reanastomosis or a transureteroureterostomy are candidates for a modified Davis ureterotomy. The minimally invasive Davis ureterotomy can effectively bridge large and small ureteral defects.
Keywords
genitourinary tract, ureter, IR procedure
Categories
Case Summary
A teenager with a malignant left retroperitoneal paraganglioma, with bone metastases including vertebrae and skull, ultimately underwent surgical resection of the retroperitoneal mass. Then, 6 weeks post resection, on a follow-up US, there had been interval development of left hydronephrosis and a large left retroperitoneal fluid collection, confirmed to be a urinoma on a CT of the abdomen and pelvis. A percutaneous left nephrostomy tube was placed, as well as a percutaneous drainage catheter in the retroperitoneal urinoma. There was an inability to traverse the ureteral defect via a retrograde approach, and a modified percutaneous Davis intubated ureterotomy (DIU) was successfully performed to traverse the ureteral defect from an antegrade and retrograde approach.
Imaging Findings
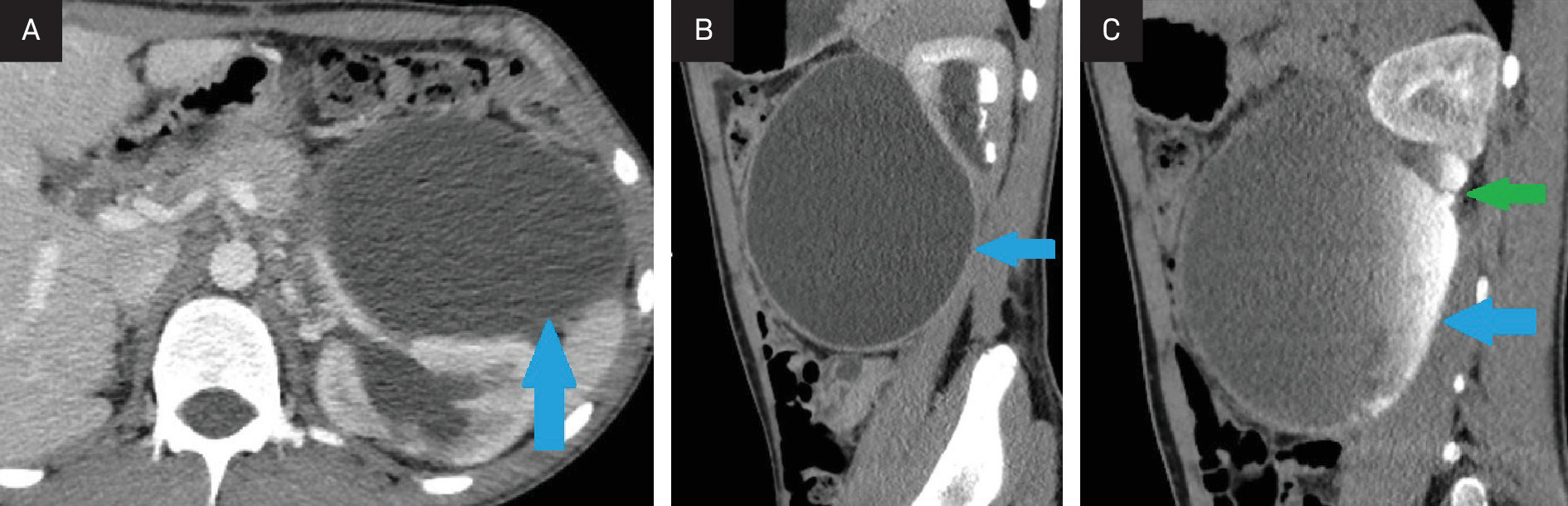
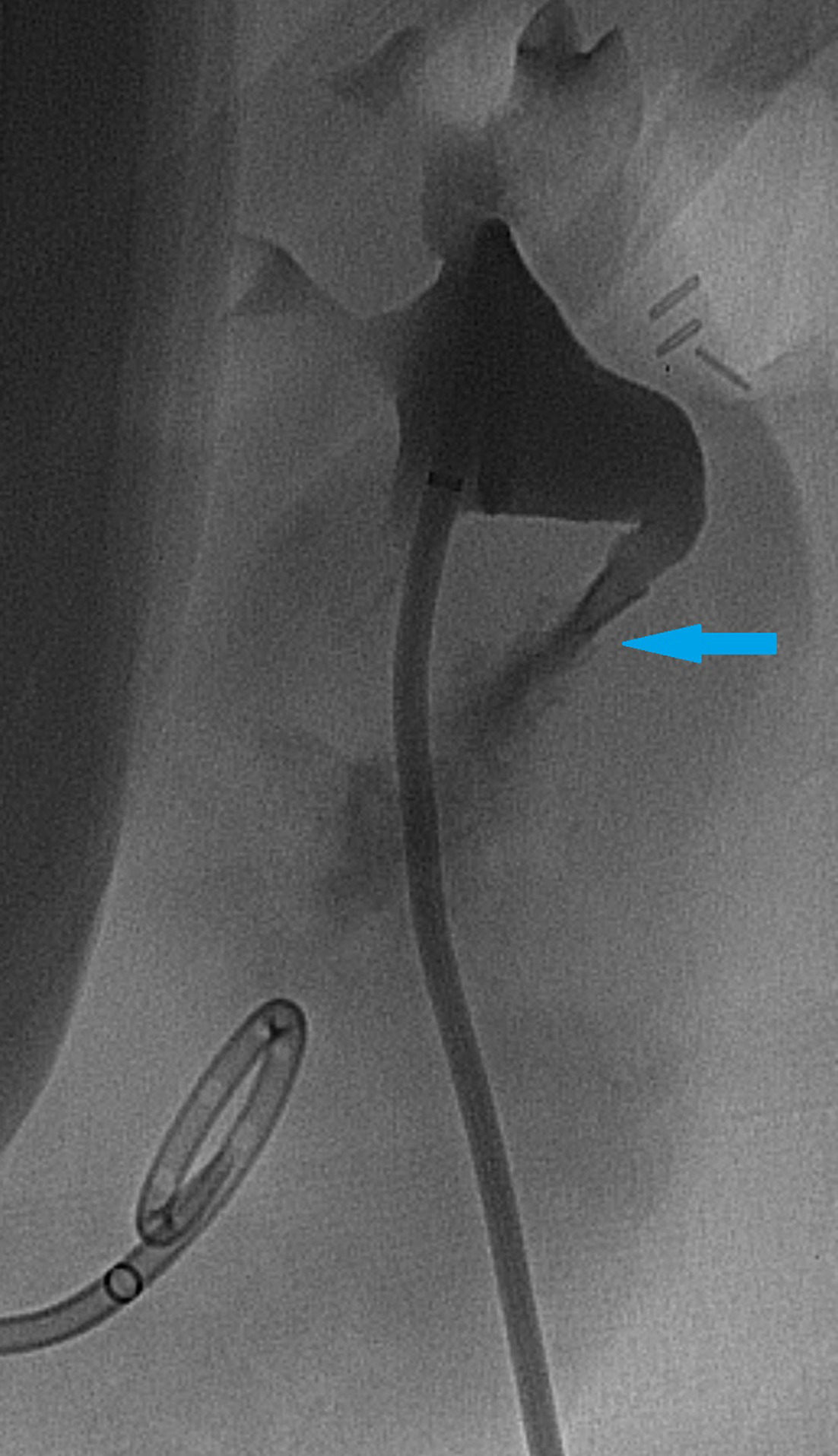
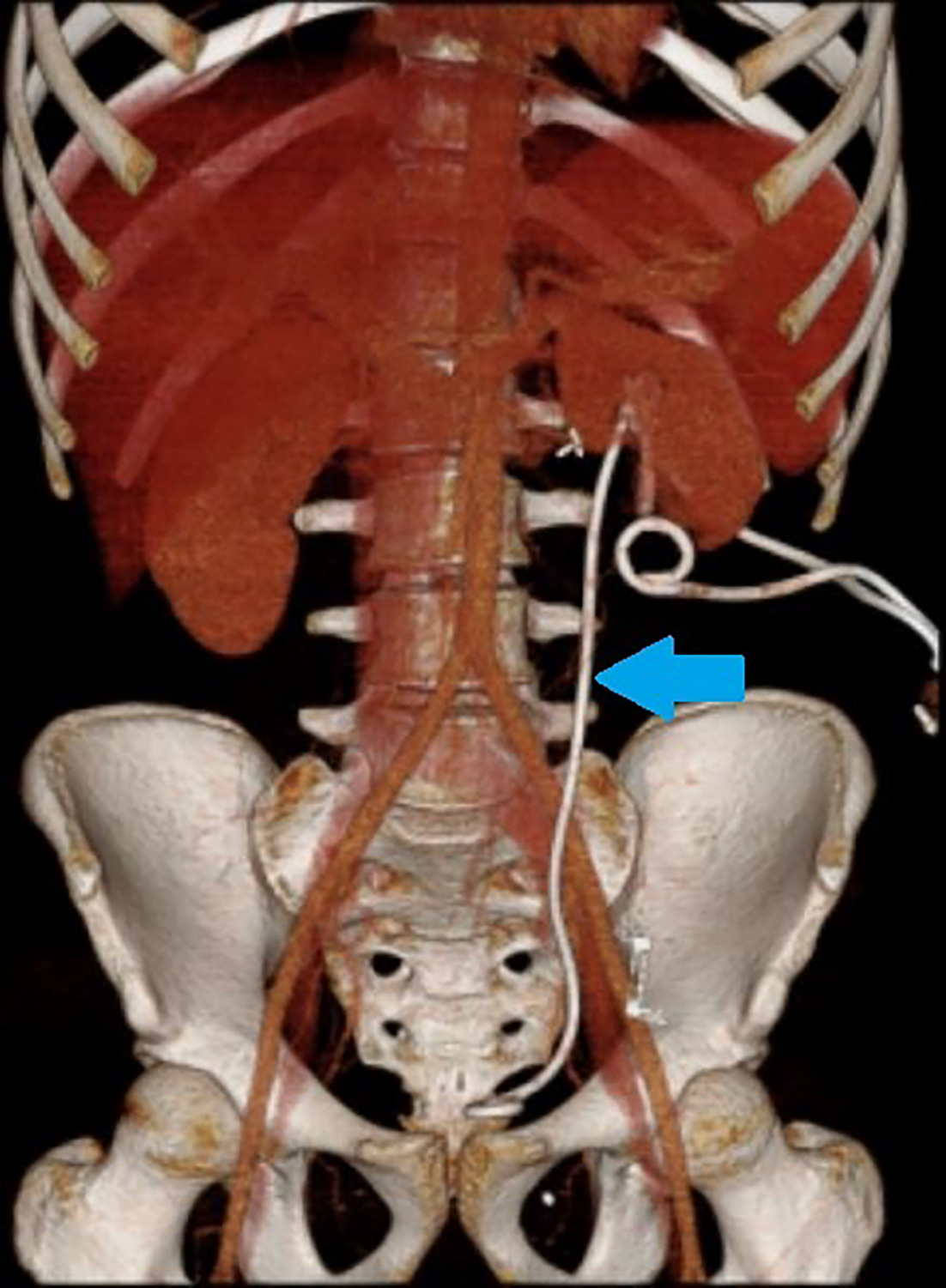
A multiphase contrast-enhanced CT of the abdomen and pelvis obtained 6 weeks post-left retroperitoneal mass resection demonstrated moderate left hydronephrosis and extravasation of contrast from the proximal left ureter into a large left retroperitoneal urinoma on delayed images (Figure 1A-C). There was no opacification of the distal ureter. A percutaneous left nephrostomy tube was then placed as well as a percutaneous drainage catheter into the urinoma (Figure 2). Subsequently, a percutaneous DIU was performed, with placement of a double-J ureteral stent traversing the ureteral defect, allowing for antegrade flow of urine from the renal pelvis into the bladder and healing of the proximal ureteral defect (Figures 3A-C, 4).
Diagnosis
Laceration/discontinuity of the ureter post resection of a retroperitoneal paraganglioma
Discussion
Historically, the DIU was performed to treat ureteral strictures.1 In this case, there was injury of the proximal ureter at the time of resection of the retroperitoneal mass, resulting in a urinoma and discontinuity of the proximal ureter with an approximate 3-cm gap. Thus, a historical surgical procedure to treat ureteropelvic junction strictures, the DIU, was modified to create a percutaneous solution. In the literature, there are 2 separate cases of ureteral intubation procedures for the treatment of iatrogenic injury and/or a traumatic injury of the ureter.2,3 However, this appears to be the first case using a modified percutaneous DIU to treat a segmental ureteral injury at the time of resection of a retroperitoneal malignancy. This discussion will review both the original procedural steps of the DIU and the histopathology of the healing ureter.
The DIU was introduced in 1943.1 The procedure was used primarily to treat obstructive ureteral strictures, more commonly in patients in whom the ureter was not long enough to resect the stricture and repair the ureteral defect. In the original DIU, surgical exposure of the kidney and ureter was accomplished.1 An incision was made in the renal pelvis above and through the ureteral stricture below, and a stent was positioned across the stricture and ureteral defect. It was then left in place for 4-6 weeks.1,2 Once the stent was removed, the healed ureter would ideally have a lumen diameter more comparable to that of a healthy ureter.
Since its introduction, the intubated ureterotomy has been modified to a percutaneous procedure using a ureteroscope. Hibi describes performing percutaneous intubated ureterotomy procedures by accessing the ureter via a nephrostomy and inserting a ureteroscope. A holmium laser is used to make incisions through the stricture enabling passage of a ureteral stent into the distal normal ureter to be left in place for 6 weeks.3 Other options for incising the ureter stricture are also utilized, including an Acucise balloon (Applied Medical, Rancho Santa Margarita, California), cold knife, and electrocautery.3,4 A percutaneous approach decreases the risks of an open procedure, but it can also often be easier for the patient and interventional radiologist and surgeon.3 This is especially relevant for patients who have strictures secondary to radiation therapy or surrounding fibrosis and adhesions would complicate exposing the ureter in an open surgery.3 In this case, the DIU procedure was further modified by Towbin and colleagues5 using invasive, image-guided techniques that can be adapted to treat ureteropelvic junction strictures as well as ureteral injuries ranging from tears to short segment resections.5 In 2014, Liu and colleagues described an alternative procedure using an endoscope.6
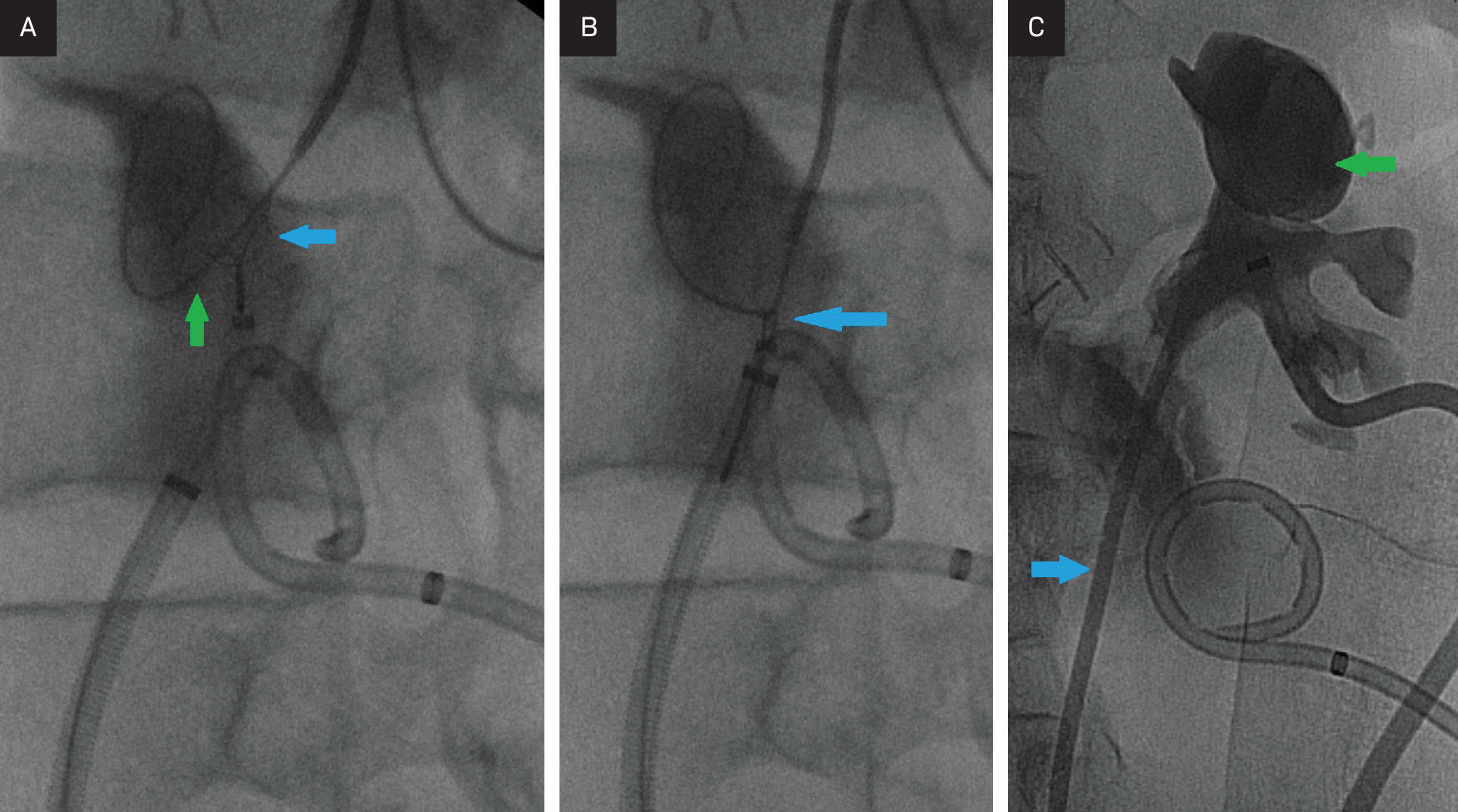
In this situation, the ureteral repair was approached antegrade and retrograde, with urology accessing the distal ureter from a retrograde urethral approach. Sheaths and directional catheters over wires were utilized antegrade and retrograde, and the catheters positioned at the junction of the proximal ureter and urinoma from an antegrade approach, and the cephalad aspect of the distal ureteral segment from a retrograde approach, under fluoroscopy. A loop snare was deployed into the urinoma from the retrograde approach, and an angled guidewire advanced into the loop snare from the antegrade approach (Figure 3A,B). Once the wire was snared, the glidewire was withdrawn into and out of the retrograde sheath, thus the wire extended outside of the antegrade and retrograde placed sheaths (a body floss). Subsequently, a double-J ureteral stent was advanced over the wire through the retrograde sheath, through the ureteral defect, and the proximal loop of the stent positioned in the left upper pole calyx, the caudad double-J ureteral stent loop positioned in the urinary bladder (Figure 3C). Additionally, the left nephrostomy tube was replaced.
Thirteen days following double-J ureteral stent placement, contrast injection of the nephrostomy tube demonstrated that contrast traversed the stent lumen with opacification of the urinary bladder, and there was not extravasation of contrast into the urinoma. The nephrostomy tube was removed 15 days following placement of the ureteral stent. A retrograde pyelogram was performed 6 weeks following ureteral stent placement, demonstrating opacification of an intact ureter and nondilated intrarenal collecting system. A proximal ureteral stricture was identified 2 months following the initial stent placement on a retrograde pyelogram, and interval ureteral stent exchanges were performed out to at least 12 months.
A minimally invasive, image-guided approach for repair of segmental ureteral gaps is an increasingly important topic. Since the introduction of laparoscopic surgery, the rate of ureteral injury has increased, and most injuries are identified postoperatively.7 The most common urologic structure injured during pelvic surgery is the ureter, with risk factors including obesity, excessive bleeding, enlarged uterus, and adhesions from prior surgeries.8
The intubated ureterotomy is successful because of the unique healing process and regeneration capabilities of the ureter. Research into the regeneration process raised the question of whether the smooth muscle can completely regenerate either by muscle cell hypertrophy or true replication.9 Some studies found that smooth muscle cells did not completely regenerate around the circumference of the ureter; instead, the gap was filled with connective tissue.2,10 Current research has shown that there is a more complete understanding of how ureteral healing occurs. Uroepithelial regeneration is the initial step in ureter healing, which usually occurs within the first 3 weeks.11 The stent acts as a guide to direct the epithelial growth so that the gap is closed in an organized manner.9 Once the epithelium has regenerated, this serves as a foundation for the rest of the ureteral layers to grow. It is believed that stent removal after 3 weeks results in normal healing of the ureter because the epithelium has grown back at that point.10 Next, the wound begins contracting and the gap is filled with connective tissue.11,12 Lastly, the fibroblasts in the connective tissue are replaced by smooth muscle cells.12 This regeneration process is the foundation for why intubation and stenting work well in patients with ureteral injuries.
The reported success rate for a DIU approaches 89%.1 The rate of success using minimally invasive techniques is likely similar; however, no large series are available for guidance. Complications include irregular regeneration, diverticulum formation, and obstruction secondary to strictures or scarring. Other problems that can be identified are infection, urinoma formation, and loss of renal function.
Conclusion
Patients with ureteral injuries who lack enough tissue to perform reanastomosis or a transureteroureterostomy are candidates for a modified Davis ureterotomy. The minimally invasive Davis ureterotomy can effectively bridge large and small ureteral defects.
References
- Davis D, Strong G, Drake W. Intubated ureterotomy; experimental work and clinical results. J Urol. 1948;59(5):851-862. doi:10.1016/S0022-5347(17)69449-7.
- Smart W. An evaluation of intubation ureterotomy with a description of surgical technique. J Urol. 1961;85(4):512-524. doi:10.1016/S0022-5347(17)65372-2.
- Hibi H, Yamada Y, Nonomura H. Percutaneous ureteral incision with a small-caliber flexible ureteroscope. JSLS. 2003;7(2):107-110.
- Arabi M, Mat’hami A, Said M. Image-guided ureteral reconstruction using rendezvous technique for complex ureteric transection after gunshot injuries. Avicenna J Med. 2016;6(1):28-30. doi:10.4103/2231-0770.173581.
- Towbin R, Wacksman J, Ball W. Percutaneous pyeloplasty in children: experience in three patients. Radiology. 1987;163(2):381-384. doi:10.1148/radiology.163.2.3562817.
- Liu C, Zhang X, Xue D, Liu Y, Wang P. Endoscopic realignment in the management of complete transected ureter. Int Urol Nephrol. 2014;46(2):335-340. doi:10.1007/s11255-013-0535-7.
- Pastore A, Palleschi G, Silvestri L. Endoscopic rendezvous procedure for ureteral iatrogenic detachment: report of a case series with long-term outcomes. J Endourol. 2015;29(4):415-420. doi:10.1089/end.2014.0474.
- Lapides J, Caffery E. Observations on healing of ureteral muscle: relationship to intubated ureterotomy. J Urol. 2017;73:47-52. doi:10.1016/S0022-5347(17)67365-8.
- Duque O, Boyarsky S. Ureteral regeneration in dogs: an experimental study bearing on the davis intubated ureterotomy. J Urol. 2017;73:53-61. doi:10.1016/S0022-5347(17)67366-X.
- McDonald J, Calams J. Experimental ureteral stricture: ureteral regrowth following ureterotomy with and without intubation. J Urol. 2017;84:52-59. doi:10.1016/S0022-5347(17)65486-7.
- Trautner K, Raaschou F. Histological examination of the regeneration of urotherthe ureter in dogs after intubated ureterotomy. J Urol. 2017;71:274-286. doi:10.1016/S0022-5347(17)67788-7.
- Velardo J, Bergman H. The ureter. 1981. doi:10.1007/978-1-4612-5907-7_2.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Modified Davis Intubated Ureterotomy. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0080.