Morgagni Hernia: An Adult with a Congenital Anomaly
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 1, 2026
1 Lewis University, Romeoville, Illinois
2 Department of Radiology, Conemaugh Memorial Medical Center, Johnstown, Pennsylvania
3 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
4 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Although Morgagni hernia is the rarest type of congenital diaphragmatic hernia, it is clinically important due to the potential for delayed diagnosis and associated complications. Its bimodal age distribution underscores the importance of recognizing this condition in both pediatric and adult populations, where symptoms can range from asymptomatic findings to severe pulmonary or gastrointestinal issues. Accurate diagnosis depends on imaging, with lateral chest x-rays often identifying initial signs, while advanced modalities like CT or MRI may provide definitive confirmation.
Keywords
gastrointestinal, stomach, adult with a congenital anomaly
Categories
Case Summary
A 40-year-old woman presented with shortness of breath and chest pain.
Imaging Findings
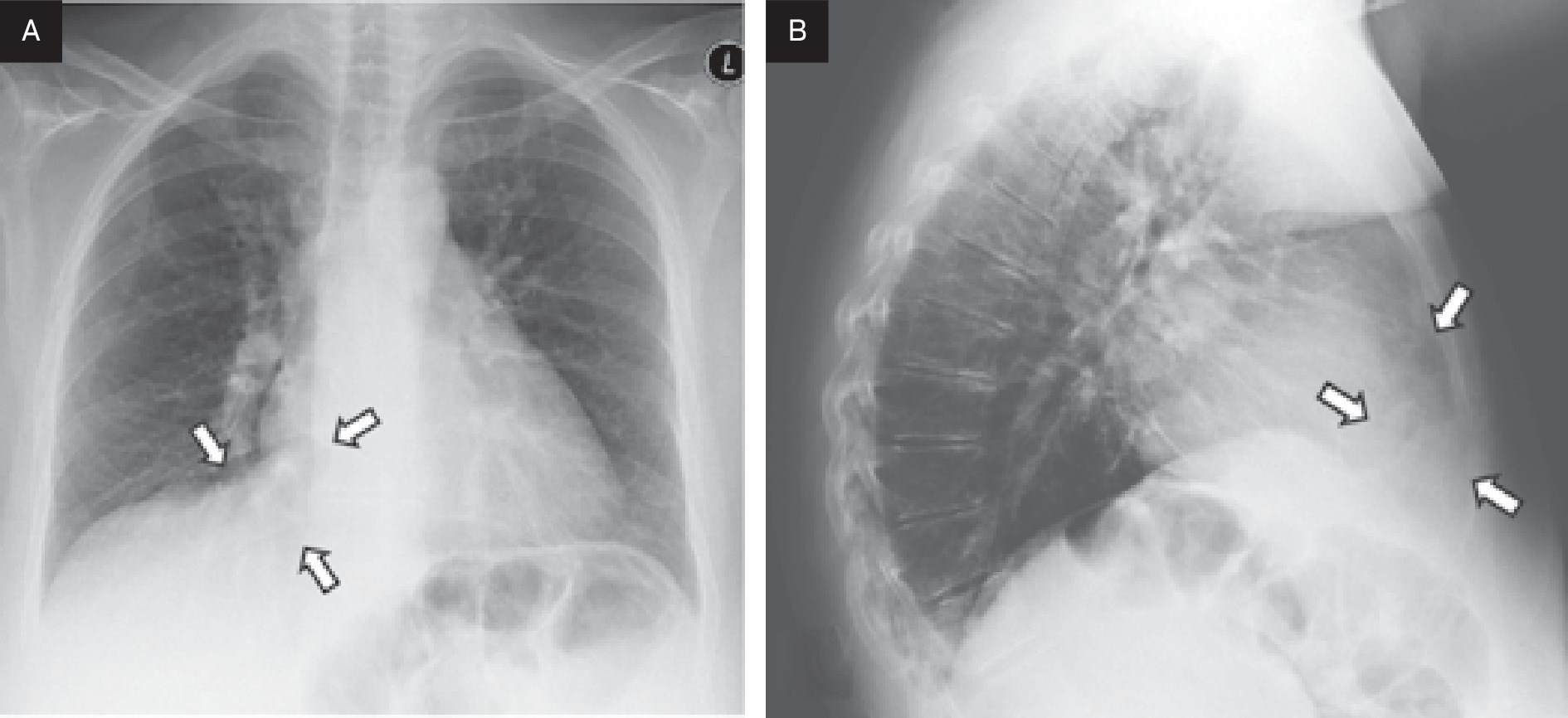
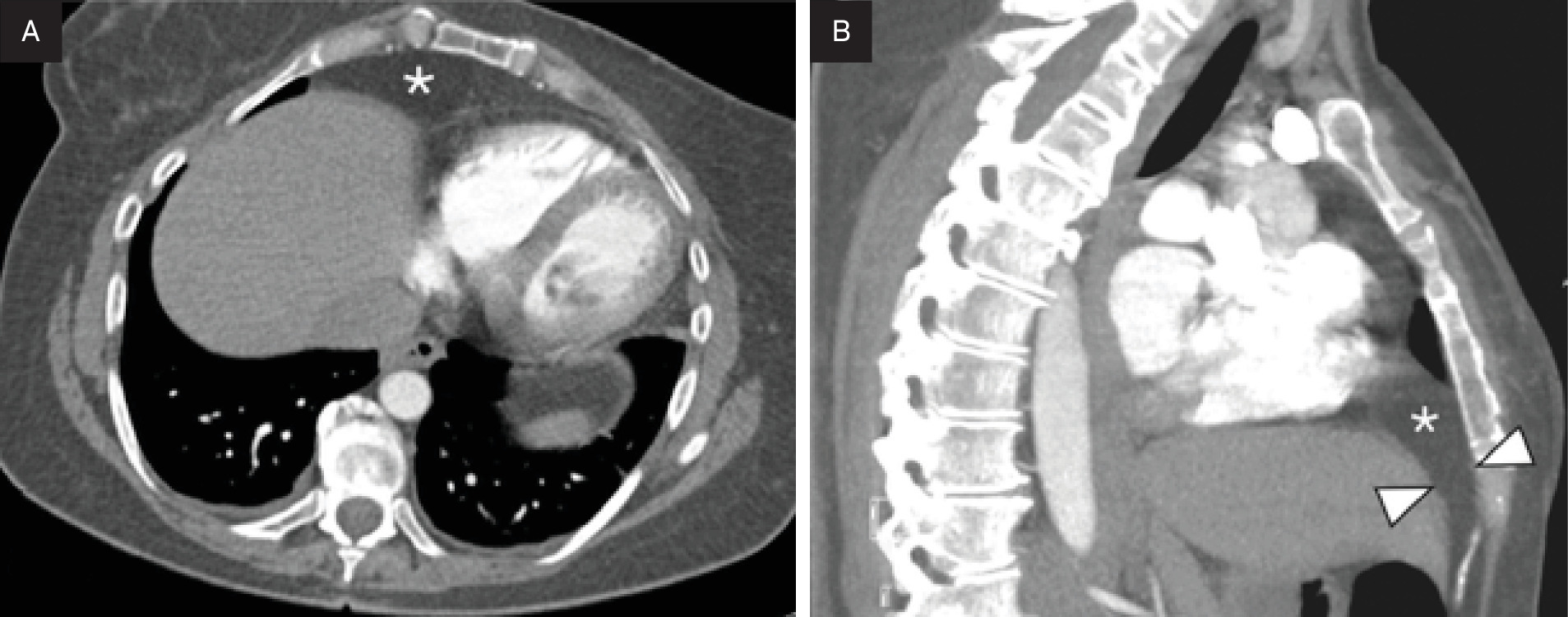
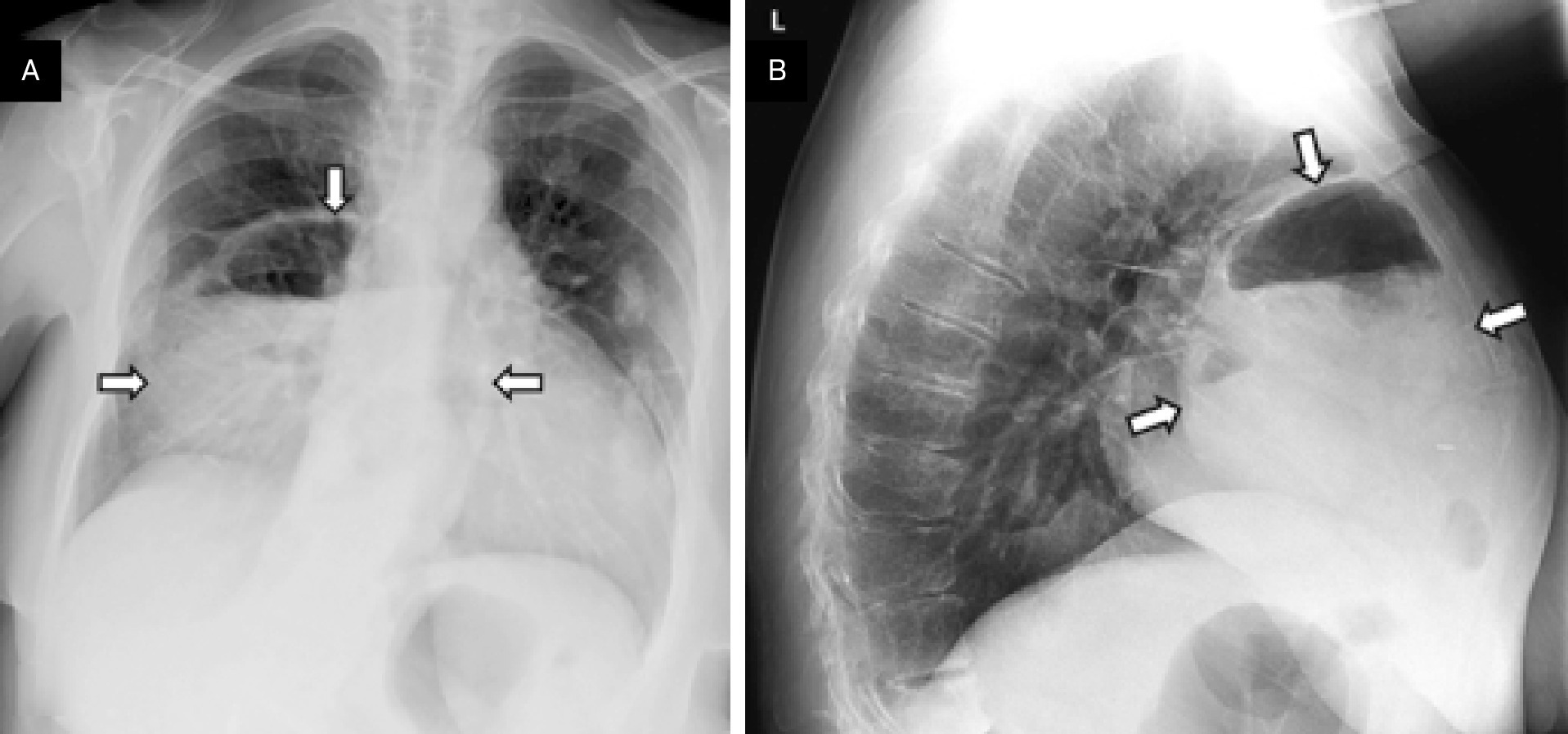
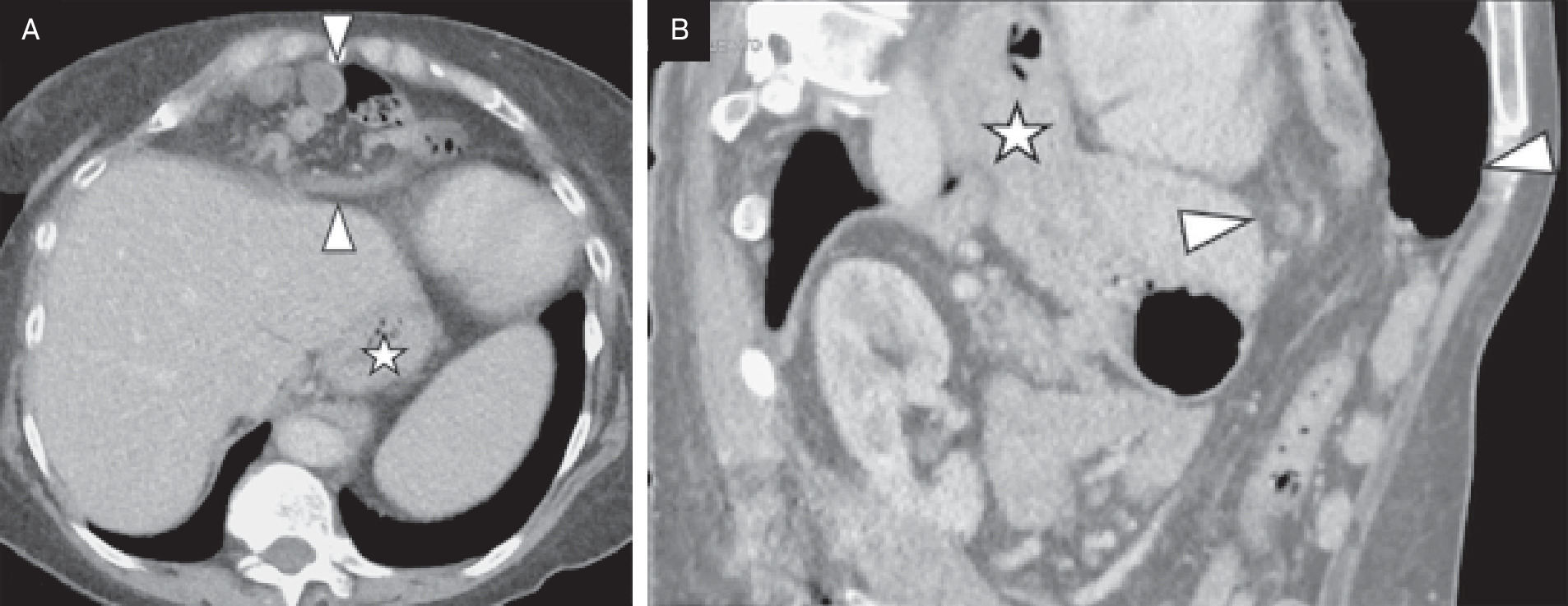
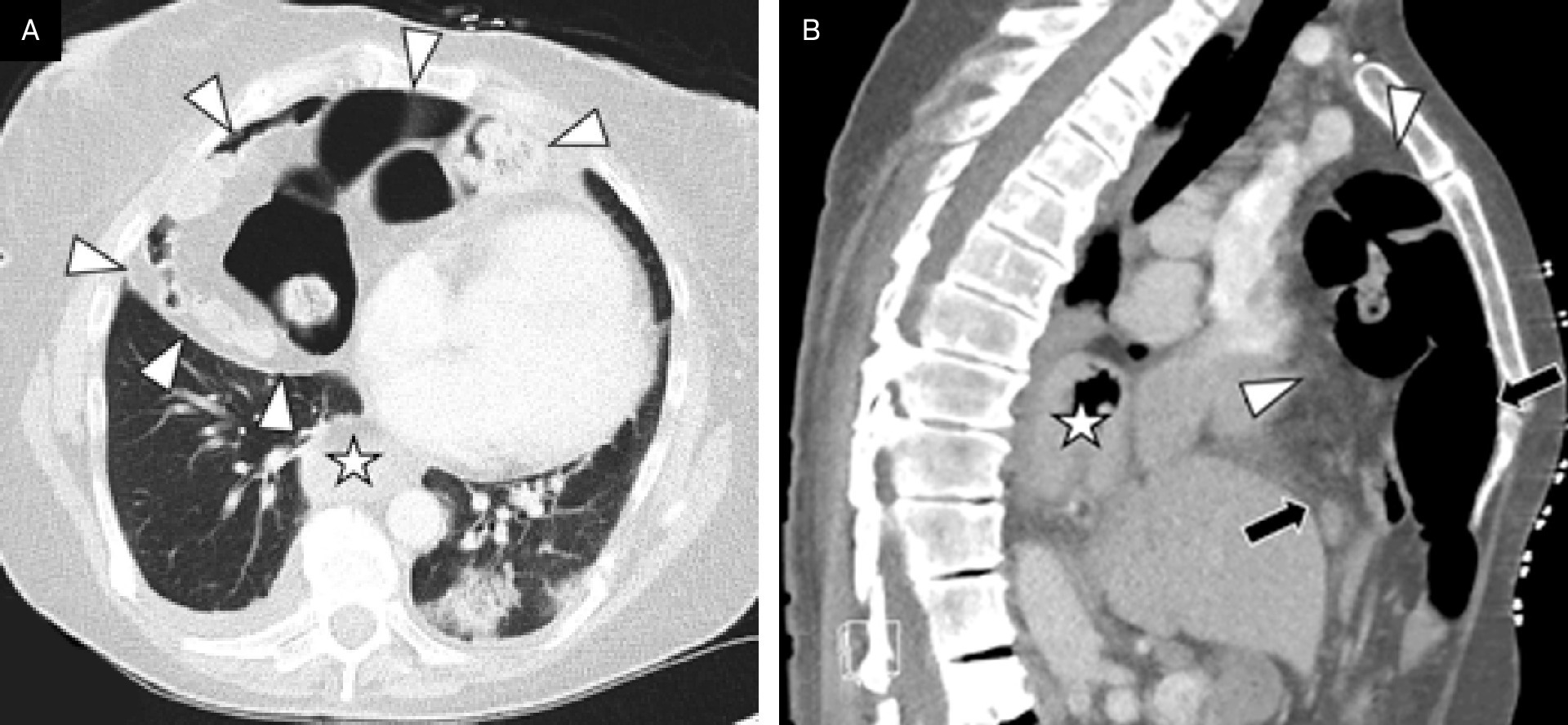
In retrospect, a chest radiograph at initial presentation (Figure 1) and subsequent chest CT (Figure 2) showed a small anterior diaphragmatic hernia containing only omental fat. She continued to experience recurrent chest pain, shortness of breath, and abdominal symptoms without a definitive diagnosis. Comorbidities in this patient included severe degenerative disk disease, asthma, and partially reversible anteroseptal cardiac ischemia. Nine years later, a chest radiograph obtained for difficulty breathing and chest pain demonstrated an enlarged anterior diaphragmatic hernia misdiagnosed as a hiatal hernia at the time. Six months later, she reported worsening chest and back pain, nausea, vomiting, and diarrhea. Retrospective review of an abdominal US from this period showed herniating omental fat in the anterior thorax that was not recognized. Ten years from her initial presentation, after a 60-pound weight loss and recurring symptoms, the patient was admitted to the hospital. A chest x-ray confirmed an enlarging Morgagni hernia (Figure 3). Abdominopelvic CT on the same date (Figure 4) demonstrated the anterior Morgagni hernia and posteriorly a large paraesophageal hernia. Concurrent chest CT imaging (Figure 5) showed the intrathoracic extent of the hernias.
Diagnosis
Morgagni hernia.
Differential diagnosis includes hiatal hernia, cardiophrenic fat pad, pericardial cyst, diaphragmatic eventration, loculated pneumothorax, lower lobe lung collapse or consolidation, lymphoma, or thymic tumor.
Discussion
A Morgagni hernia is the rarest subtype of congenital diaphragmatic hernia (CDH), representing 2-4% of all cases.1 It results from an anteromedial sub-costosternal diaphragmatic defect defined by the failure of the pars tendinalis of the costochondral arches to fuse with the pars sternalis during embryonic development. Morgagni hernia exhibits a bimodal age distribution, typically presenting in infants and young children, predominantly males, within the first year of life. The estimated incidence is between 1 in 2000 and 1 in 5000 live births. In children, it is often asymptomatic but may present with nonspecific findings such as respiratory distress, failure to thrive, recurrent pulmonary infections, poor feeding, or choking during feeding. In pediatric patients, it is often associated with other congenital abnormalities such as cardiac anomalies and Trisomy 21.1 In general, those presenting after 8 weeks of life in the pediatric population have a benign course and respond well to surgical repair.2 In rare cases, Morgagni hernia may present in adulthood, with a mean age at diagnosis of 57 years and a higher prevalence observed in females.3 Presentation in adults is often (72%) symptomatic, most commonly with pulmonary symptoms.4 Acute complications, such as intestinal ischemia due to bowel strangulation or gastric volvulus, may also occur.5
These hernias are most frequently located on the right side and are characterized by the herniation of abdominal contents into the thoracic cavity.4 While they most commonly contain omental fat, herniation of the transverse colon, small bowel, stomach, or liver can also occur. Differential considerations on plain chest x-ray include cardiophrenic fat pad, diaphragmatic eventration, pericardial cyst, loculated pneumothorax, lower lobe lung collapse or consolidation, lymphoma, or thymic tumor. Diagnosis is often made incidentally on lateral chest x-ray, especially when bowel is visible anteriorly within the thoracic cavity.1 If suspected, the diagnosis may be confirmed when abdominal CT or MRI demonstrates intrathoracic herniation of omental fat or air-filled viscera anteriorly,6 with loss of continuity between the diaphragm and the lower sternum, especially on a sagittal view. A barium study or US may support the diagnosis.7
Conclusion
Although Morgagni hernia is the rarest type of CDH, it is clinically important due to the potential for delayed diagnosis and associated complications. Its bimodal age distribution underscores the importance of recognizing this condition in both pediatric and adult populations, where symptoms can range from asymptomatic findings to severe pulmonary or gastrointestinal issues. Accurate diagnosis depends on imaging, with lateral chest x-rays often identifying initial signs, while advanced modalities like CT or MRI may provide definitive confirmation.
References
- Svetanoff W, Sharma S, Rentea R. In: StatPearls [Internet]. 2025.
- Berman L, Stringer D, Ein S, Shandling B. The late-presenting pediatric morgagni hernia: a benign condition. J Pediatr Surg. 1989;24(10):970-972. doi:10.1016/s0022-3468(89)80193-9.
- Archer J, Williams N. Non-operative management of a large morgagni hernia-an alternative approach?. J Surg Case Rep. 2023;2023(1). doi:10.1093/jscr/rjac614.
- Horton J, Hofmann L, Hetz S. Presentation and management of morgagni hernias in adults: a review of 298 cases. Surg Endosc. 2008;22(6):1413-1420. doi:10.1007/s00464-008-9754-x.
- Sonthalia N, Ray S, Khanra D. Gastric volvulus through morgagni hernia: an easily overlooked emergency. J Emerg Med. 2013;44(6):1092-1096. doi:10.1016/j.jemermed.2012.11.103.
- Kuikel S, Shrestha S, Thapa S. Morgagni hernia in adult: a case report. Int J Surg Case Rep. 2021;85. doi:10.1016/j.ijscr.2021.106286.
- Shi H, Chen W, Yin Q, Zhang X. Ultrasound diagnosis of congenital morgagni hernias: ten years of experience at two chinese centers. World J Clin Cases. 2024;12(3):495-502. doi:10.12998/wjcc.v12.i3.495.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Morgagni Hernia: An Adult with a Congenital Anomaly. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0081.