1 NY Institute of Technology, School of Osteopathic Medicine, Old Westbury, New York
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 University of Cincinnati College of Medicine, Cincinnati, Ohio
4 Department of Radiology, Cincinnati Children’s Hospital, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Moyamoya is an uncommon but important cause of cerebrovascular events in children. Cerebral angiography has been the gold standard for diagnosis. However, with the evolution of CTA and MR angiogram, these noninvasive modalities have become the preferred initial examinations. Although both imaging modalities can diagnose moyamoya, MRI is preferred because it is more sensitive to the detection of brain injury such as stroke. Further research is needed to better understand the role of genetics in the development and progression of the disease, as well as to increase treatment options.
Keywords
moyamoya disease, brain, arterial occlusions, strokes
Categories
Case Summary
A Caucasian infant with an optic nerve glioma and neurofibromatosis type 1 underwent MR angiogram (MRA) for suspected moyamoya.
Imaging Findings
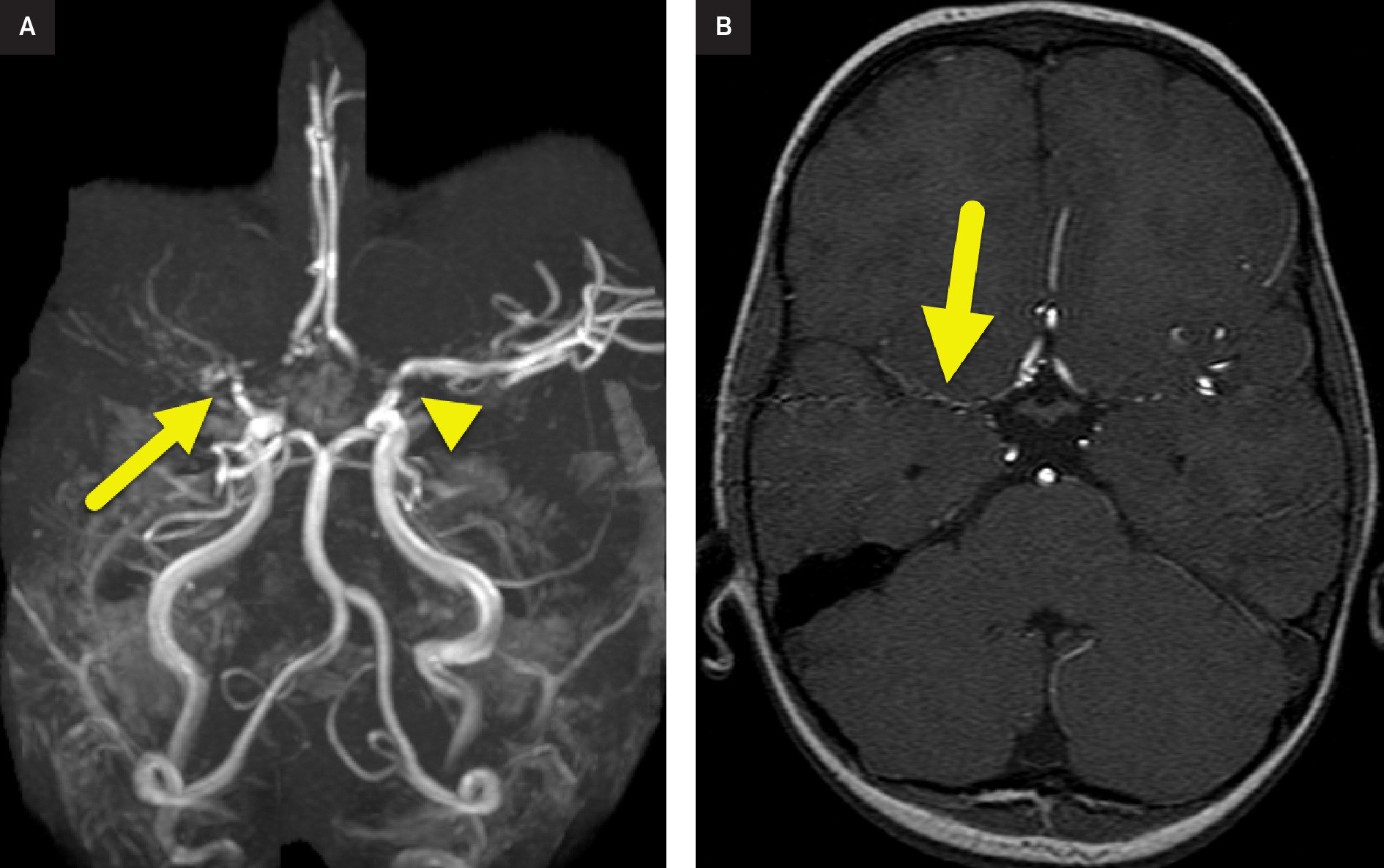
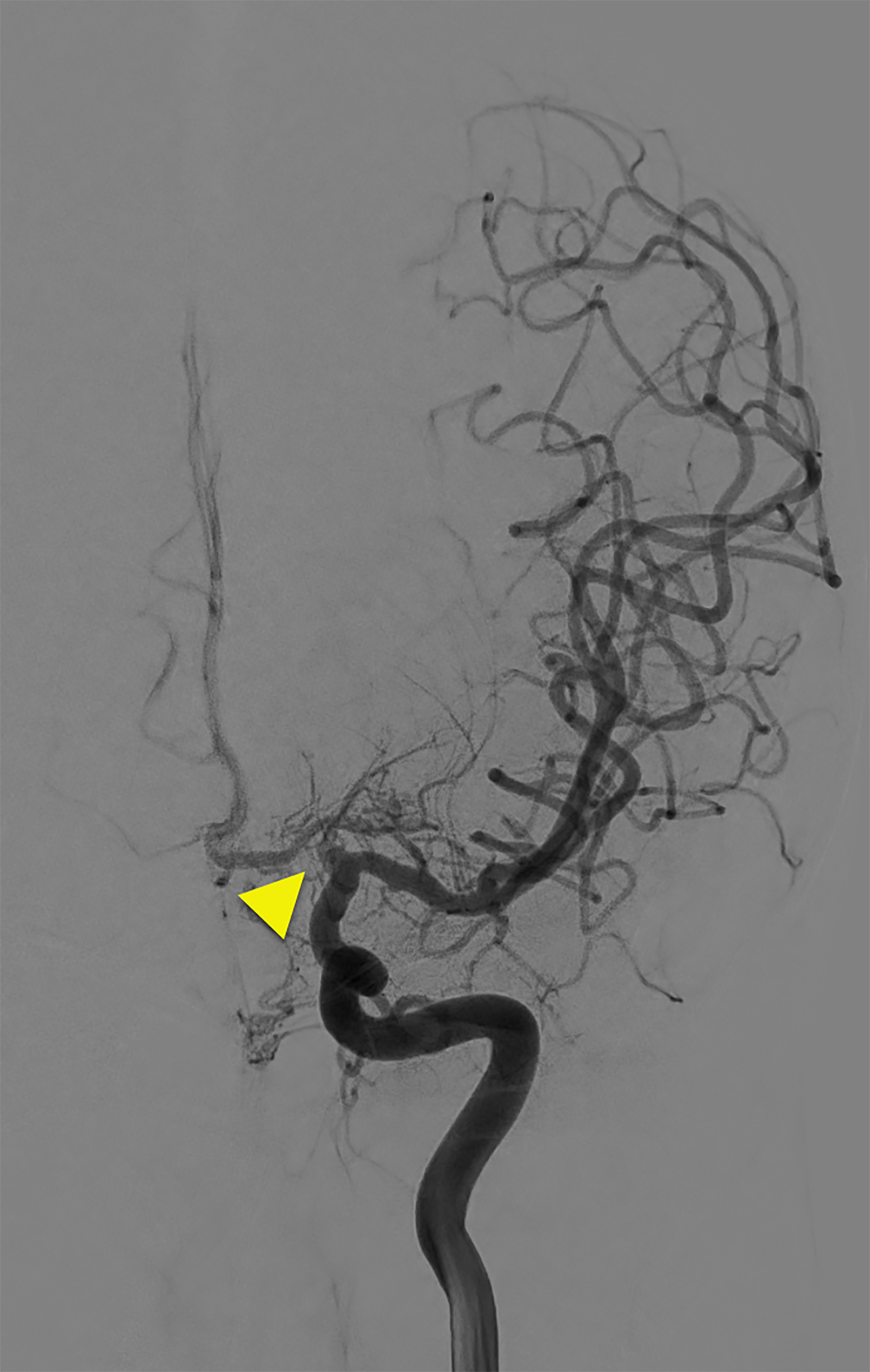
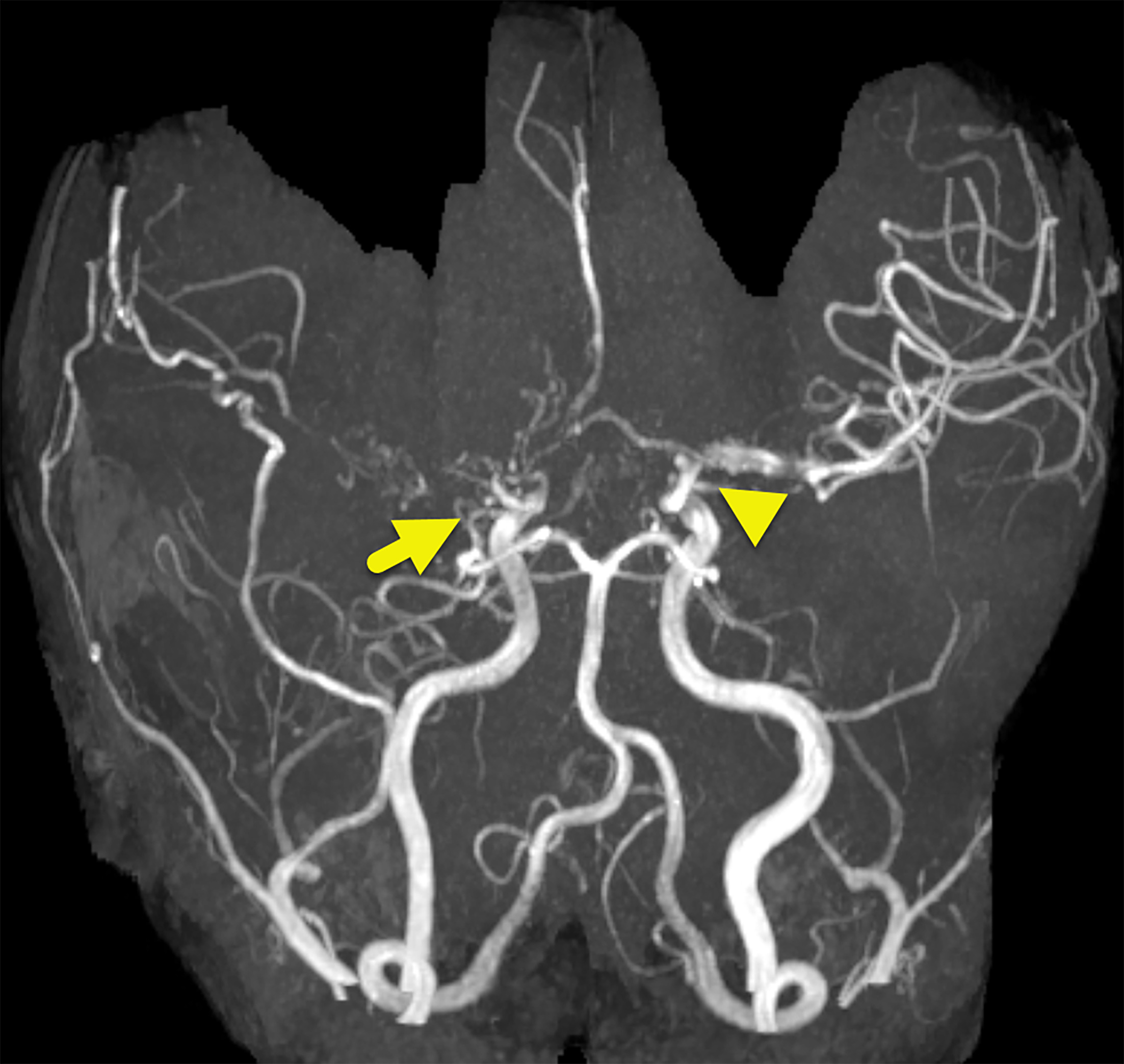
MRA showed high-grade stenosis at the bifurcation of the right internal carotid artery and moderate stenosis at the bifurcation of the left internal carotid artery (Figure 1). The patient was eventually treated with bilateral cerebral bypass with parietal superficial temporal artery pial synangiosis and dural inversion using the middle meningeal artery. Follow-up imaging was obtained (Figures 2, 3).
Diagnosis
Moyamoya disease.
The differential diagnosis of moyamoya includes cerebrovascular events such as anterior circulation stroke, intracranial hemorrhage, cavernous sinus syndromes, cerebral aneurysms (although it can be caused by rupture of moyamoya vessels), blood dyscrasias, dissection syndromes, fibromuscular dystrophies, homocysteinemia, and hyper/hypoglycemia. The diagnosis of moyamoya should be made by exclusion of the above conditions and imaging criteria according to the revised 2021 diagnostic criteria for moyamoya disease (MMD). 1
Discussion
Moyamoya is a term that describes specific angiographic findings demonstrating unilateral or bilateral stenoses, or occlusion resulting from progressive narrowing of arteries near the circle of Willis with associated small vessel collaterals. The term moyamoya disease is used when referring to an idiopathic origin of disease, and moyamoya syndrome (MMS) refers to these vascular findings in the presence of an associated condition, such as sickle cell disease, neurofibromatosis type I (NF1), Down syndrome, and autoimmune diseases. 2 MMS is a vasculopathy associated with NF1 and is an underrecognized complication of the disease. NF1 vasculopathy occurs in 3-5% of children who have imaging studies and is estimated to affect 2.5-7.5% of children with NF1.
Moyamoya has a bimodal age distribution, affecting children between the ages of 5-9 and adults in their mid-40s. MMD is more common in patients of Asian heritage, with the highest incidence occurring in the Japanese population. Moyamoya is the most common pediatric cerebrovascular disease in Japan, with a prevalence of 3 per 100,000 children. In the United States, the prevalence is lower, affecting 0.086 per 100,000 children. 3
The increased incidence in the people of Japanese descent is caused by genetic predisposition. Approximately 10-15% of Japanese patients with MMD have a family history of the disease. Evidence indicates familial MMD is an autosomal-dominant disease with incomplete penetrance, caused by the RNF213 gene on chromosome 17q25.3. 2
In MMD, the main pathological features of moyamoya include fibrocellular thickening and vessel occlusion from a combination of hyperplasia of smooth-muscle cells and luminal thrombosis. Vascular changes may be a consequence of impaired response to inflammation or defects regarding cellular repair mechanisms. This leads to a cascade of angiogenesis-related factors, including endothelial colony-forming cells, various cytokines, vascular endothelial growth factor, and basic fibroblast growth factor. 4 Angiogenesis and the formation of collateral vessels contribute to irregularly placed lamina and thinned media, which leads to microaneurysms with potential for hemorrhage. 5 Increased and dilated cortical microvascularization has been suggested as a specific finding in MMD and may compensate for slow blood flow. This process occurs before hemodynamic impairment, demonstrating an active process and not just a consequence of occlusion. 2 In MMS due to NF1, the vasculopathy is thought to be due to the dysfunction of the protein neuroformin. Neuroformin is a negative regulator of the Ras pathway that regulates cell growth, differentiation, and survival. The dysregulation of the pathway leads to dysfunction of vascular cells, resulting in abnormal vessel formation and exaggerated response to injury that can result in intimal thickening and inflammation. In patients with sickle cell anemia (SSA), the vessel injury is due to polymerization of hemoglobin S. This leads to rigid, crescent-shaped cells that cause vaso-occlusive events. This exaggerated process is caused by low nitric oxide bioavailability due to multiple factors, including hemolysis, ischemia-reperfusion, inflammation, oxidative stress hypercoagulability, and other factors. This complex interaction leads to vessel injury, occlusion, and collateral vessel development.
The presentation of MMS can vary based on its association. Children with Down syndrome are more likely to present with a stroke and bilateral disease, while children with SSA and NF1 are more likely to be asymptomatic and have unilateral disease.2 Children less than 2 years are also more likely to have a stroke at presentation. Often, MMD will present as a migraine-like headache that can persist despite treatment and revascularization. Another rare association is the “morning glory disk anomaly,” an enlarged optic disc with concomitant retinovascular abnormalities. 3 The cause of a morning glory optic disc is poorly understood.
The diagnosis of moyamoya is made by identifying the characteristic angiographic appearance of stenoses and occlusions affecting the distal internal carotid arteries or other proximal circle of Willis vessels. Vascular imaging should be considered in children/young adults with signs and symptoms of ischemic attacks and unexplained cerebral hemorrhage. 5
The gold standard for diagnosis of moyamoya is cerebral angiography. This method allows for visualization of the vascular stenoses, occlusions, and collateral vessels from the terminal portion of the internal carotid artery. 6 Cerebral angiography typically demonstrates stenosis or occlusion of the supraclinoid carotid artery, proximal anterior and middle cerebral arteries with associated numerous small vessel collateral vessels most often involving the lenticulostriate and thalamoperforators, mimicking a “puff of smoke.” However, since catheter angiography is invasive, CTA or MRA are preferred as initial imaging.
CTA can demonstrate vascular abnormality as well as brain hemorrhage, stroke, and intracranial stenoses and offers the advantages of speed and accessibility. However, CTA is limited since it cannot visualize small-caliber collateral arteries and has a high radiation dose. 7
MRI with MRA is increasingly used as the primary imaging modality. It can demonstrate acute infarcts, diminished cortical blood flow, large vessel occlusion, and collateral blood flow. The ivy sign may be present on FLAIR and T1 post-contrast sequences. This sign represents slow flow in pial collateral vessels and appears as a linear high signal following a leptomeningeal and sulcal pattern. 7 The ivy sign has been correlated with later stages of disease progression.
Currently, there is no known treatment that will reverse the primary disease process. Thus, current management is aimed toward improving cerebral blood flow and preventing future strokes. Surgical revascularization is the most successful way to improve cerebral hemodynamics and provides the added benefit of reducing the risk of future stroke. 8 Most procedures involve some type of bypass, with the most common being a direct bypass graft (extracranial to intracranial) via a superficial temporal artery to middle cerebral artery anastomosis. Indirect bypass techniques, which normally induce spontaneous angiogenesis between the surface of the brain and donor tissues, may be utilized. However, recovery is longer with this approach as it takes 3-4 months to see the benefits of the added collateral circulation. Newer techniques combine both direct and indirect bypass. 8
Conclusion
Moyamoya is an uncommon but important cause of cerebrovascular events in children. Cerebral angiography has been the gold standard for diagnosis. However, with the evolution of CTA and MRA, these noninvasive modalities have become the preferred initial examinations. Although both imaging modalities can diagnose moyamoya, MRI is preferred because it is more sensitive to the detection of brain injury such as stroke. Further research is needed to better understand the role of genetics in the development and progression of the disease, as well as to increase treatment options.
References
- Kuroda S, Fujimura M, Takahashi J. Diagnostic criteria for moyamoya disease - 2021 revised version. Neurol Med Chir. 2022;62(7):307-312. doi:10.2176/jns-nmc.2022-0072.
- Ihara M, Yamamoto Y, Hattori Y. Moyamoya disease: diagnosis and interventions. Lancet Neurol. 2022;21(8):747-758. doi:10.1016/S1474-4422(22)00165-X.
- Smith E, Scott R. Moyamoya disease and moyamoya syndrome. N Engl J Med. 2009;361(1):97-98. doi:10.1056/nejmc090780.
- Fang Y, Wei L, Hu C, Tu Y. Pathological circulating factors in moyamoya disease. Int J Mol Sci. 2021;22(4). doi:10.3390/ijms22041696.
- Li J, Jin M, Sun X. Imaging of moyamoya disease and moyamoya syndrome: current status. J Comput Assist Tomogr. 2019;43(2):257-263. doi:10.1097/RCT.0000000000000834.
- Filimonova E, Ovsiannikov K, Rzaev J. Neuroimaging in moyamoya angiopathy: updated review. Clin Neurol Neurosurg. 2022;222:107471. doi:10.1016/j.clineuro.2022.107471.
- Sivrioglu A, Saglam M, Yildiz B, Anagnostakou V, Kizilkilic O. Ivy sign in moyamoya disease. Eurasian J Med. 2016;48(1):58-61. doi:10.5152/eurasianjmed.2015.14142.
- Arias E, Derdeyn C, Dacey R, Zipfel G. Advances and surgical considerations in the treatment of moyamoya disease. Neurosurgery. 2014;74(suppl 1):S116-S125. doi:10.1227/NEU.0000000000000229.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Moyamoya Disease. Applied Radiology. 2026. doi:10.37549/JPCR-25-0018.