MR of spinal trauma: Part II
Applied Radiology — Vol. 6 , Issue 1 , pp. 25 -29
DOI: 10.37549/AR1005
Published: June 1, 2001
Categories
The conclusion of this two-part series will discuss the MR findings in distraction trauma involving the spine. It is understood that there will be some overlap between the various categories of trauma. Therefore, some of the findings discussed in the first section of this series (Appl Radiol 30(4):36-44) may also be found in some of the cases found here. Nevertheless, the main factor considered in this category is the type of injury that results from the spatially deforming nature of many types of spinal trauma.
Distraction spinal trauma
Distraction trauma to the spine is defined as that which causes a spatial distortion of the bony elements of the spine as well as of the related neural and non-neural soft tissues. This type of trauma includes spinal dislocations and avulsion trauma to neural tissue, the meninges, the spinal ligaments, and the spinal blood vessels.
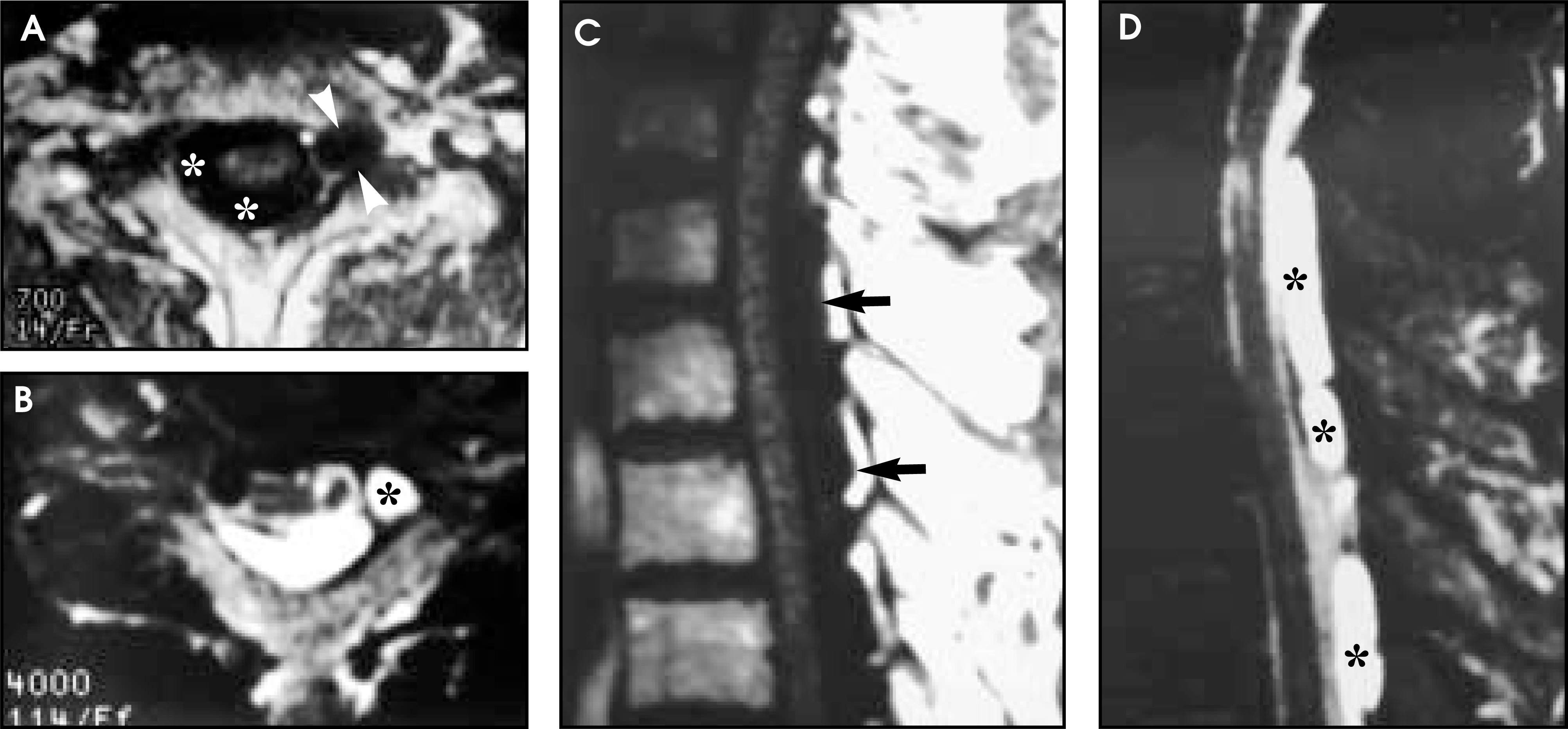
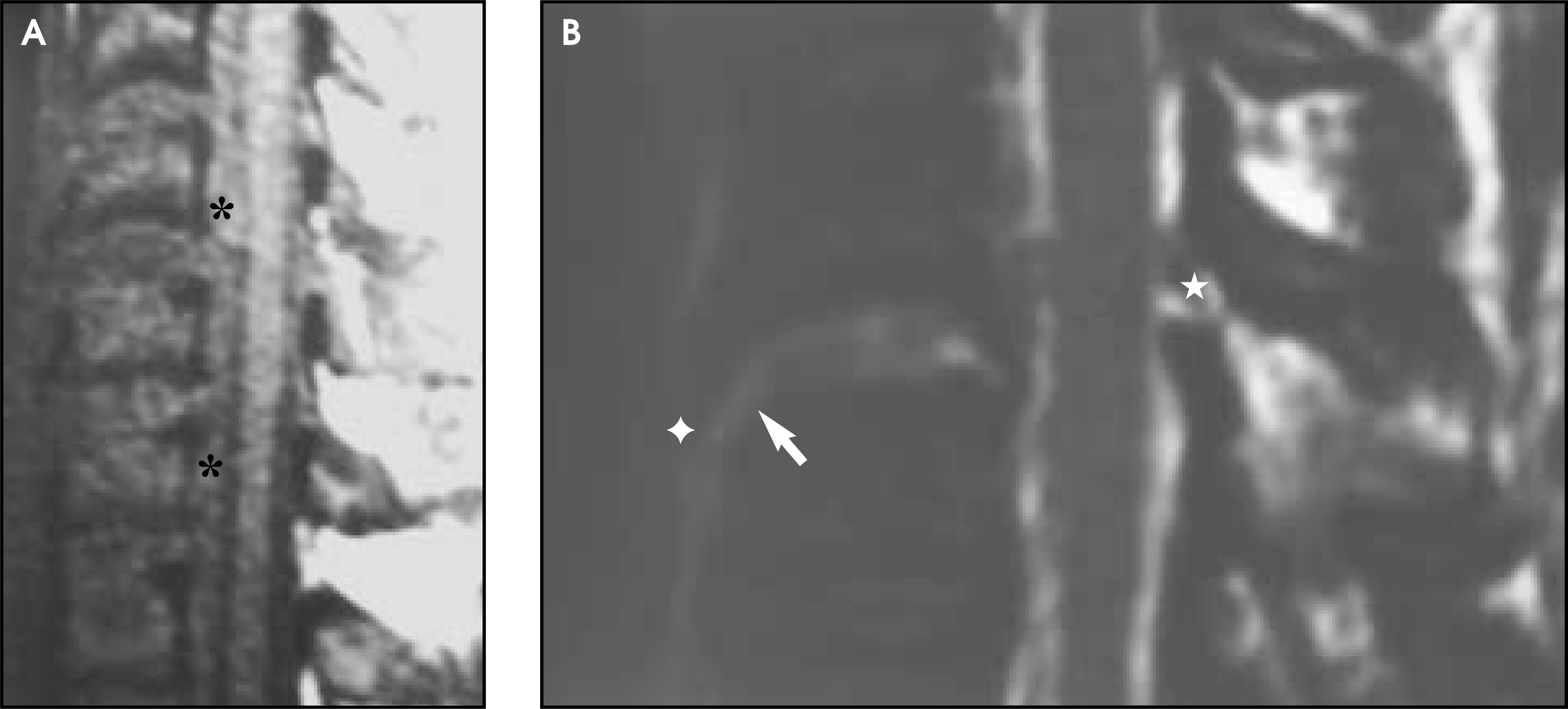
Upper extremity overextension such as that occuring during falls from moving vehicles (e.g., motorcycle injury) may result in brachial plexus avulsion. Major pelvic trauma, on the other hand, may cause avulsion of lumbar and sacral nerve roots. In this injury, varying numbers of spinal nerve roots may be avulsed from their insertions into the spinal cord and/or the thecal sac. At the same time, the regional meninges also tear, resulting in extravasation of cerebrospinal fluid (CSF) into the surrounding soft tissues in the area(s) of the nerve root sleeve(s). Eventually this extravasation walls off, resulting in a cystic area that communicates directly with the spinal subarachnoid space. Because it does not have a true meningeal lining, the term posttraumatic pseudomeningocele is used. On conventional myelography, the subarachnoid space will be seen to communicate with the pseudomeningocele(s). On magnetic resonance (MR) T1-weighted imaging (T1WI) the pseudomeningocele appears hypointense and round, oval, or multilobulated (figure 1). These pseudomeningoceles may also occur at more than one level, and there may be an intraspinal component that compresses the spinal cord away from the side of the pseudomeningoceles (figure 2). They become hyperintense on T2-weighted imaging (T2WI) acquisitions, paralleling CSF intensity. Usually little or no peripheral enhancement can be identified in chronic lesions following IV gadolinium (Gd) administration.1-8 If the goal is only the diagnosis of pseudomeningocele, MR may be all that is needed for the diagnostic evaluation. However, MR has proven inadequate for cervical nerve root visualization at the levels of injury prior to undertaking surgical neural repair. In this circumstance, water-soluble contrast myelography followed by high-resolution, thin-section computed tomography (CT) is the best imaging modality to employ at the present time.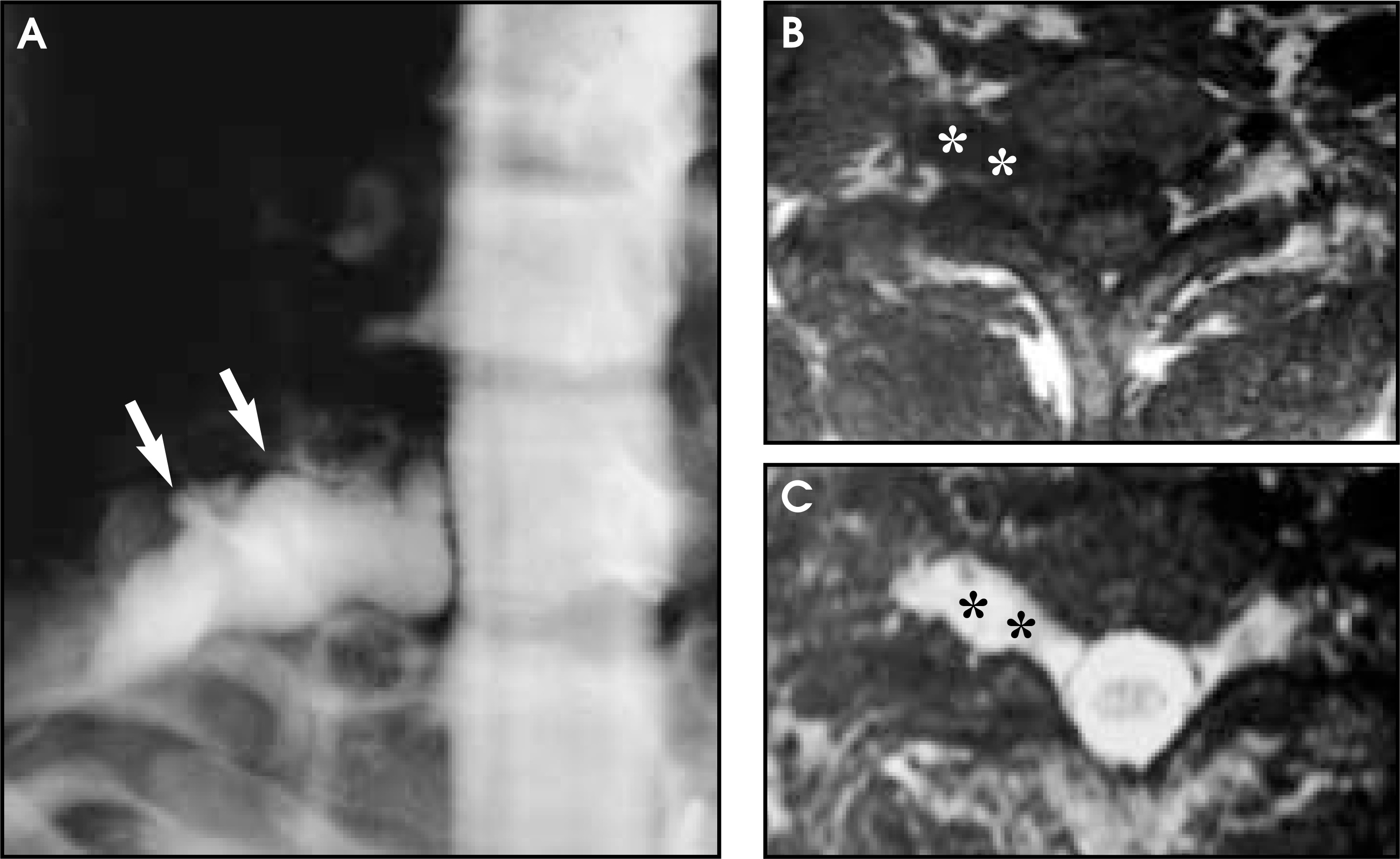
If sufficiently severe, flexion injuries of the spine may cause posterior spinal facet joint dislocation. This is most commonly seen in the cervical spine where the orientation of the facet surfaces is more horizontal and the facet surface area is smallest, thereby predisposing to this type of injury. The inferior aspect of the suprajacent facet may partially dislocate anterosuperiorly to lie at the junction of the superior aspect of the subjacent facet (i.e., incomplete dislocation or "perched" facet); or alternatively, the facet may completely dislocate anteriorly (i.e., complete dislocation or "jumped" facet). Posterior spinal facet joint dislocation may be unilateral or bilateral and is often associated with contusion to the spinal cord. In the cervical region, facet dislocations may be seen together with direct injuries to the vertebral arteries travelling within the foramina transversaria of the cervical vertebrae.
On MR, the abnormal relationships between the partially or completely dislocated facet joints can be clearly assessed on the far lateral parasagittal images (figures 3 and 4). This abnormal facet orientation is best seen on T1WI or intermediate-weighted MR acquisitions. The presence or absence of associated cord contusion is well assessed on sagittal T2WI. Possible vertebral artery injury can be evaluated on axial MR acquisitions as an absence of flow void within the affected vertebral artery(ies) (figure 4). However, because of the normal asymmetry in size of the vertebral arteries and the flow through them, MR angiography can be helpful in the evaluation of suspected cases of traumatic dissection(s) of the vertebral arteries with regard to lateralization and extent of involvement.9-17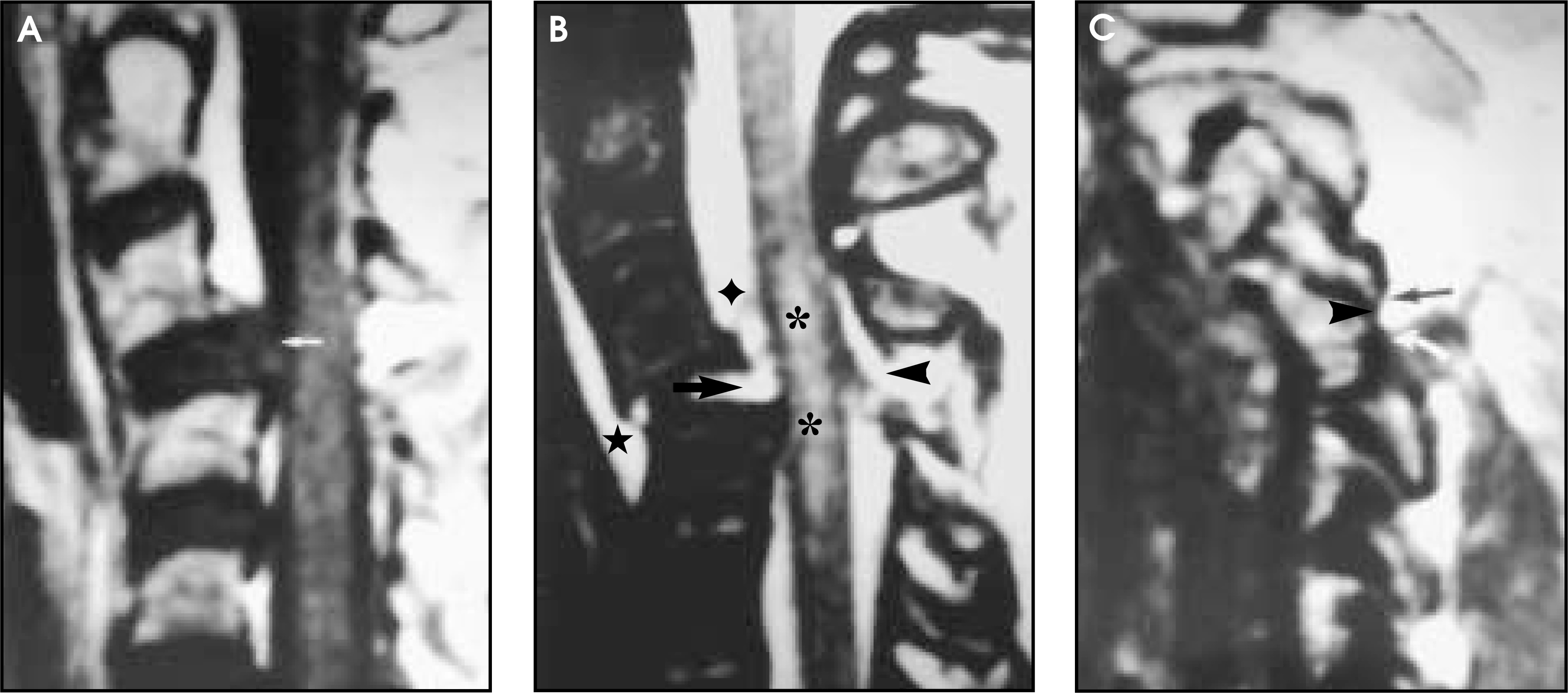
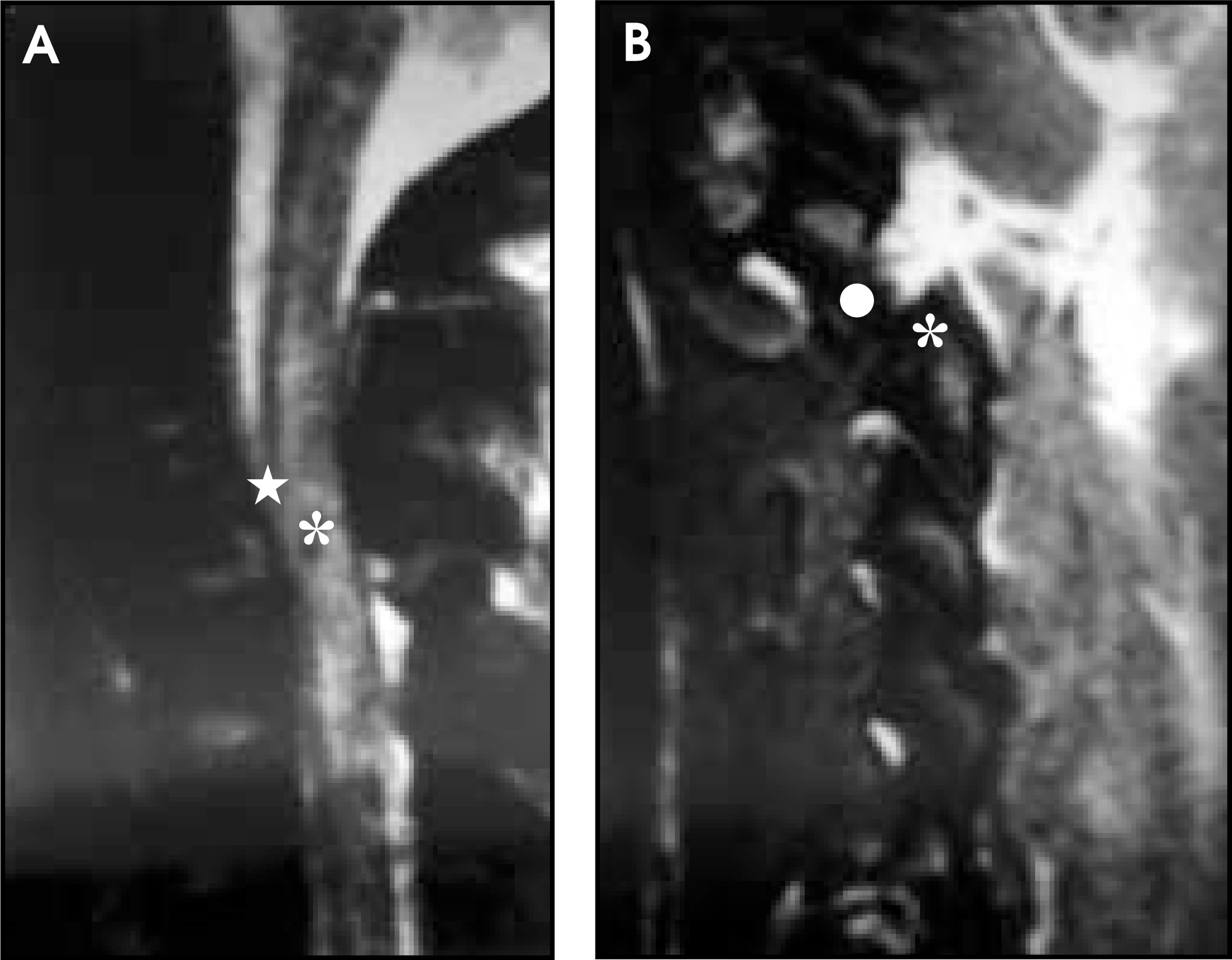
The integrity of the spinal ligaments is a critical component of stability of the spinal column. While dynamic flexion-extension conventional radiography and CT reconstructions can show intrinsic bony abnormalities and abnormal bony relationships, at present, direct imaging information concerning the status of the spinal ligaments can be gained only by MR. Fast spin echo T2WI is very helpful in the analysis of the spinal ligaments when coupled with fat suppression. In the normal patient, the CSF is hyperintense on fat-suppressed fast spin echo T2WI, while almost all other tissues are relatively hypointense. Therefore, when spinal ligaments are disrupted and/or are edematous or hemorrhagic, as may happen with trauma, these ligaments become uncharacteristically hyperintense on these acquisitions (figure 5). Frank spinal ligamentous disruptions can thereby be visualized, such as in cases of tears of the longitudinal spinal ligaments, the anulus fibrosus and the ligamenta flava (figures 3, 5, and 6). As noted above, this is important because these ligaments act as significant structural bridges between adjacent vertebral bodies. Therefore, traumatic disruption of these ligaments usually leads to segmental spinal instability requiring surgical repair.18,19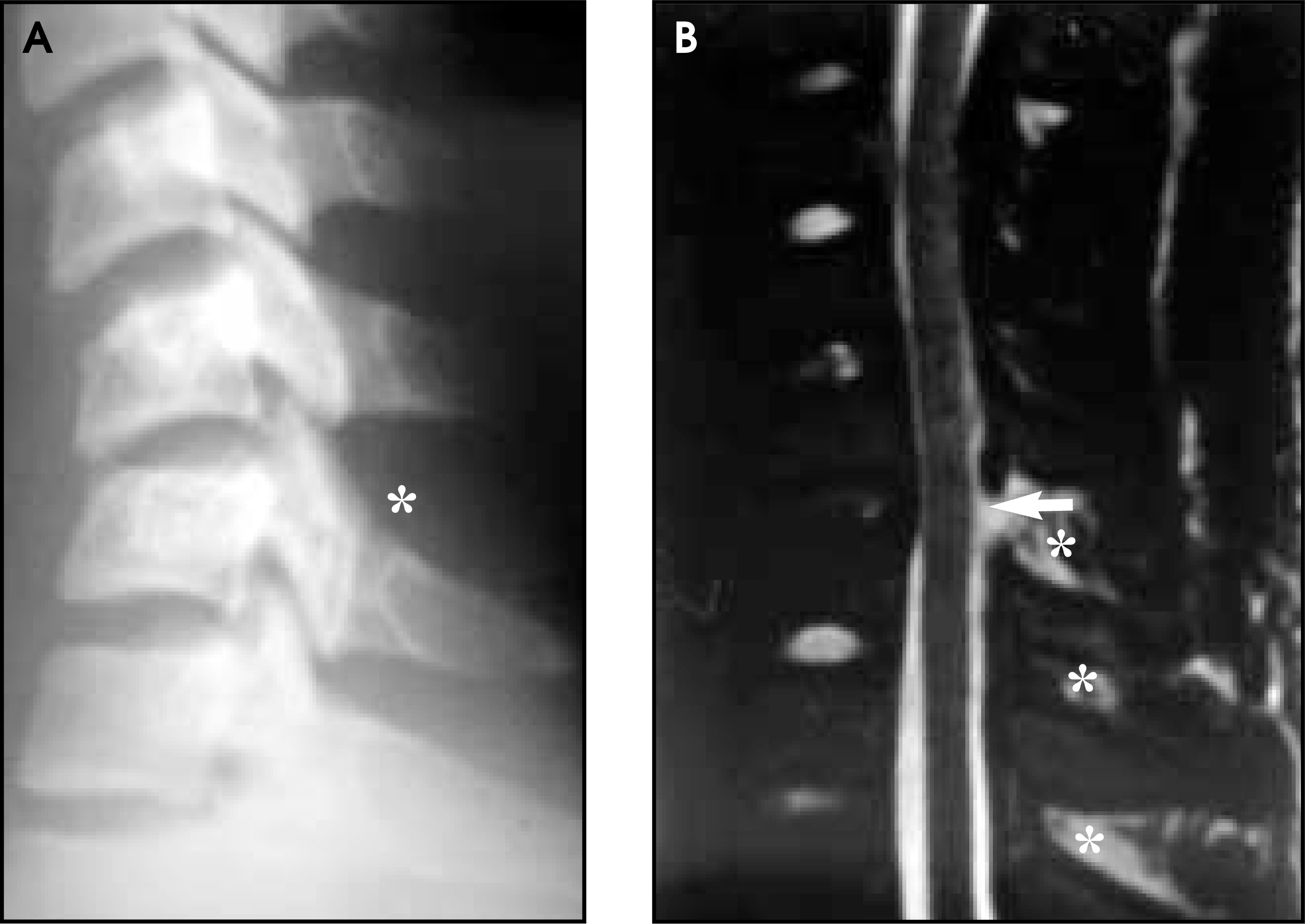
With more severe trauma, complete disjunction of the spinal column may occur with associated transection of the spinal cord. On MR, the disjoined spinal column can be identified clearly along with the transected spinal cord as it floats more or less freely within the CSF (figure 7). Since nothing can be done at present to substantially improve the neurologic status of a transected spinal cord, noninvasive assessment and confirmation of this condition by MR may be sufficient to conclude the diagnostic imaging evaluation in such cases.20-22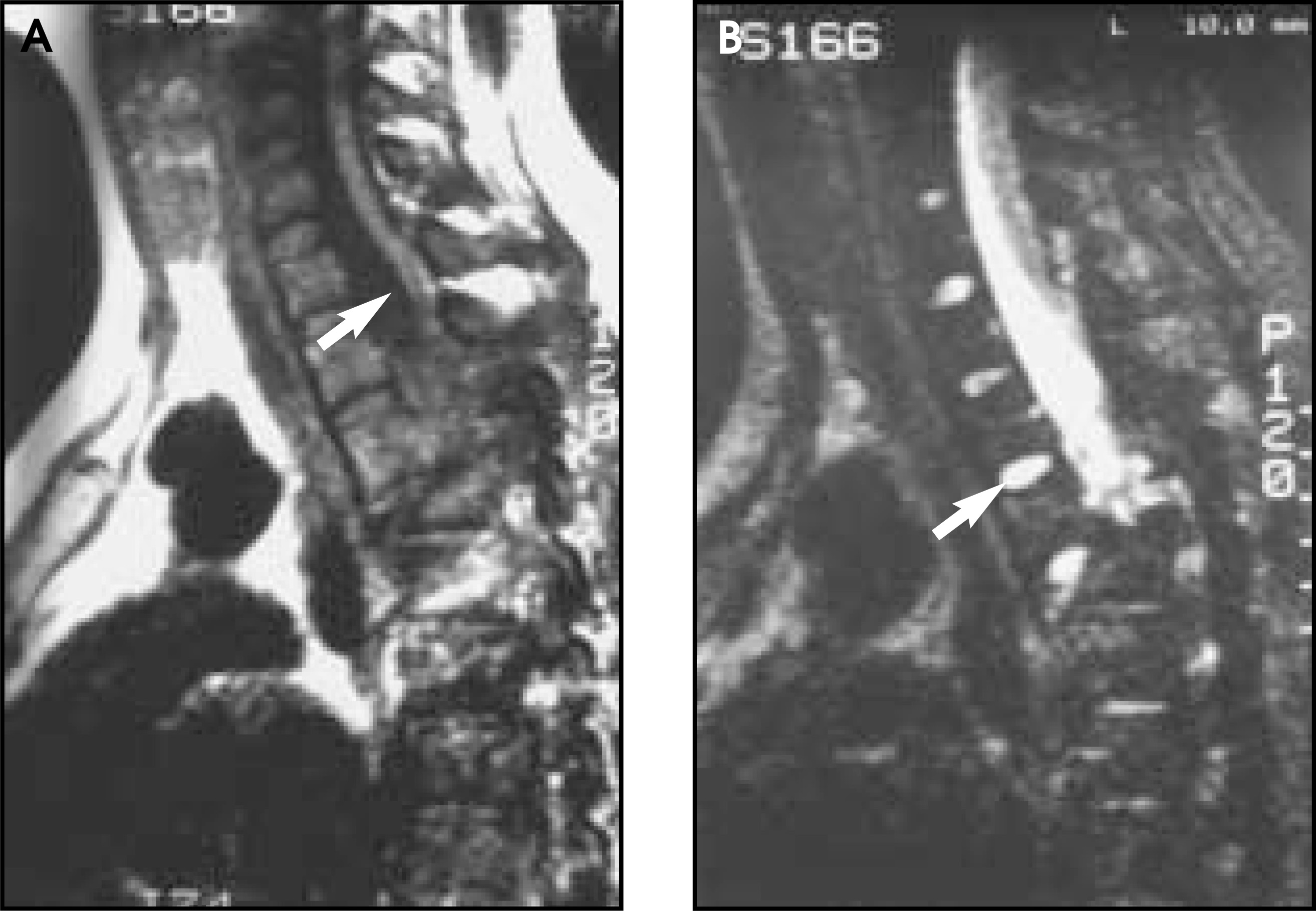
Conclusion
Trauma to the spine resulting in distraction and spatial distortion injury can be evaluated excellently with MR imaging, for the most part. However, although MR can frequently show indirect signs (e.g., ligamentous disruption) of posttraumatic spinal instability, dynamic flexion-extension MR to analyze for true spinal instability is at present not widely available. In a critical situation, dynamic conventional radiography performed by the radiologist and clinician under fluoroscopic control remains the most sensitive and clinically judicious method of analysis in this subset of patients. A second limitation of MR is its present insensitivity in visualizing remnants of cervical nerve roots in cases of brachial plexus avulsion under consideration for surgical repair. While MR clearly demonstrates the posttraumatic pseudomeningocele, remnants of surviving spinal nerve roots are best visualized by water-soluble contrast myelography coupled with thin-section, high-resolution CT. Intrathecal MR contrast agents may someday soon perform similarly in such situations. Barring these considerations, MR imaging, including MR angiography, is an excellent modality to employ for the noninvasive work-up of patients presenting with acute distraction trauma to the spine associated with neurologic signs and symptoms. In these cases, MR may reveal dramatic alterations not visible on conventional radiography, myelography, or CT. AR
References
- Cobby M, Leslie J, Watt I. Cervical myelography of nerve root avulsion injuries using water-soluble contrast media. Br J Radiol. 1988;61:673-678.
- Freedy R, Miller K, Eick J, Granke D. Traumatic lumbosacral nerve root avulsion: Evaluation by MR imaging. J Comput Assist Tomogr. 1989;13:1052-1057.
- Gupta R, Mehta V, Banerji A, Jain R. MR evaluation of brachial plexus injuries. Neuroradiology. 1989;31:377-381.
- Roger B, Travers V, Laval-Jeantet M. Imaging of posttraumatic brachial plexus injury. Clin Orthopaed Rel Res. 1988;237:57-61.
- Petras A, Sobel D, Mani J, Lucas P. CT myelography in cervical nerve root avulsion. J Comput Assist Tomogr. 1985;9:275-279.
- Popovich M, Taylor F, Helmer E. MR imaging of birth-related brachial plexus avulsion. Am J Neuroradiol. 1989;10:S98.
- Volle E, Assheuer J, Hedde J, Gustorf-Aeckerle R. Radicular avulsion resulting from spinal injury: Assessment of diagnostic modalities. Neuroradiology. 1992;34:235-240.
- Hayashi N, Yamamoto S, Okubo T. Avulsion injury of cervical nerve roots: Enhanced intradural nerve roots at MR imaging. Radiology. 1988;206:817-822.
- Katirji M, Reinmuth O, Latchaw R. Stroke due to vertebral artery injury. Arch Neurol. 1985;42:242-248.
- Leite C, Escobar B, Bazan C, Jinkins J. MRI of cervical facet dislocation. Neuroradiology. 1997;39:583-588.
- Tracy P, Wright R, Hanigan W. Magnetic resonance imaging of spinal injury. Spine. 1989;14:292-301.
- Eismont F, Arena M, Green B. Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg. 1991;73A:1555-1560.
- Doran S, Papadopoulos S, Ducker T, Lillehei K. Magnetic resonance imaging documentation of coexistent traumatic locked facets of the cervical spine and disc herniation. J Neurosurg. 1993;79:341-345.
- Jabre A. Subintimal dissection of the vertebral artery in subluxation of the cervical spine. Neurosurgery. 1991;29:912-915.
- Louw J, Mafoyane N, Small B, Neser C. Occlusion of the vertebral artery in cervical spine dislocations. J Bone Joint Surg. 1990;72B:679-681.
- Friedman D, Flanders A, Thomas C, Millar W. Vertebral artery injury after acute cervical spine trauma: Rate of occurrence as detected by MR angiography and assessment of clinical consequences. AJR. 1995;164:443-447.
- Golueke P, Sclafani S, Phillips T, Goldstein A. Vertebral artery injury–Diagnosis and management. J Trauma. 1987;27:856-865.
- Emery S, Pathria M, Wilber R. Magnetic resonance imaging of posttraumatic spinal ligament injury. J Spinal Disorders. 1989;2:229-233.
- Kliewer M, Gray L, Paver J. Acute spinal ligament disruption: MR imaging with anatomic correlation. J Magn Reson Imaging. 1993;3:855-861.
- Castillo M, Quencer R, Green B. Cervical spinal cord injury after traumatic breech delivery. AJNR. 1989;10:S99.
- Mathis J, Wilson J, Barnard J, Zelenik M. MR imaging of spinal cord avulsion. Am J Neuroradiol. 1988;9:1232-1233.
- Mendolsohn D, Zollars L, Weatherall P, Girson M. MR of cord transection. J Comput Assist Tomogr. 1990;14:909-911.
Citation
. MR of spinal trauma: Part II. Applied Radiology. 2001;6(1):25-29. doi:10.37549/AR1005.