Multiple Cranial Nerve Palsies After Reirradiation With Proton Therapy in Nasopharyngeal Carcinoma: A Case Report
Applied Radiation Oncology
Published: May 1, 2026
1 Department of Radiation Oncology, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma, USA
* Corresponding author: Christina Henson (christina-henson@ouhsc.edu)
Abstract
Nasopharyngeal carcinoma (NPC) is a rare form of cancer that has a strong association with the Epstein-Barr virus. There is little consensus on treatment for recurrent NPC, and depending on the extent of the disease, options include surgery, reirradiation, or enrollment in a clinical trial. Reirradiation, although a common and accepted treatment for recurrent NPC, carries a risk of significant late toxicity. Here, we describe the case of a young patient who experienced multiple cranial neuropathies after reirradiation for NPC recurrent to an intraparotid lymph node. The patient, while disease-free, continues to have symptoms related to these neuropathies, with significant atrophy of the left side of the tongue, dysphonia, and a winged scapula, and the focus of care is now on improving his overall quality of life. Further research is needed to explore the effects of systemic therapies on cranial nerves, as well as strategies to reduce the risk of damage to these structures.
Keywords
Nasopharyngeal carcinoma, cranial nerve palsy, proton therapy, case report, intensity-modulated radiation therapy, radiation therapy, Epstein-Barr virus
Categories
Case Summary
A 19-year-old patient with T2 N2 M0, stage III, nasopharyngeal carcinoma (NPC) and no significant medical history presented with progressive, left-ear pain presumed to be the result of an ear infection. He completed a course of antibiotics, but his symptoms did not improve, and he started to have associated epistaxis and nasal fullness, and developed a left neck mass. Physical examination revealed no signs of a tumor in the left external auditory canal. He had vague, palpable adenopathy in the left side of his neck, with no adenopathy in the posterior triangle.
Imaging Findings
Pretreatment imaging (PET/CT and MRI) revealed a 3.1 × 2.6 cm mass in the left fossa of Rosenmuller, as well as bilateral cervical lymphadenopathy, left greater than right, involving level 2 and retropharyngeal nodes bilaterally, as well as level 3 on the left.
Diagnoses and Treatment
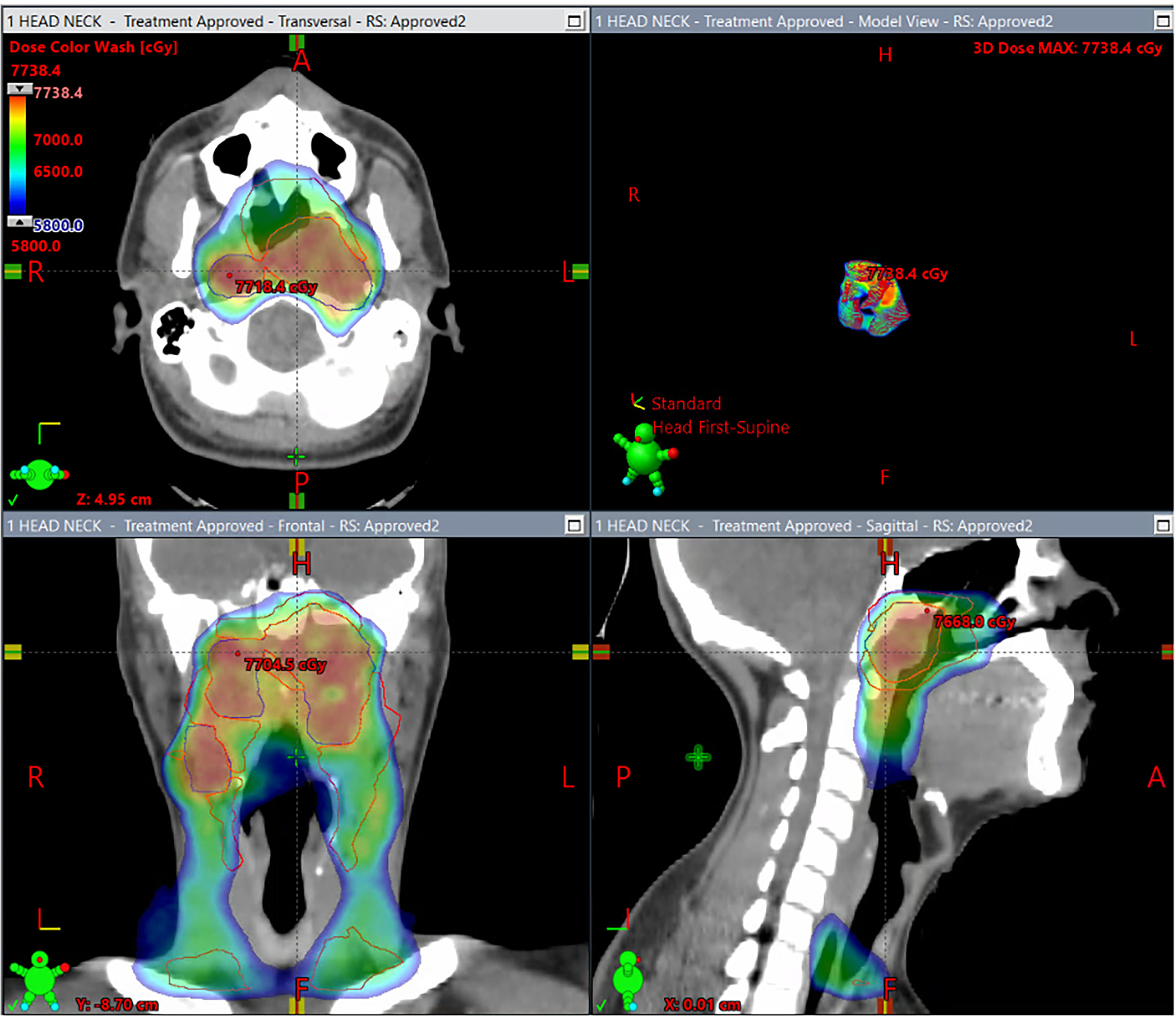
Biopsy revealed non-keratinizing squamous cell carcinoma, Epstein-Barr encoding region in situ hybridization (EBER-ISH) positive. The patient tolerated his initial chemoradiotherapy to 70 Gy in 33 fractions using proton therapy with concurrent cisplatin (100 mg/m²) every 3 weeks (Figure 1). Initial side effects included faint erythema of the skin of the neck bilaterally and grade 2 mucositis of his soft palate. The patient developed progressive dysgeusia and odynophagia during treatment, and his weight decreased overall by 9 kg (20 lbs). He had a G-tube placed, which stabilized his weight. He completed treatment with good recovery and an isolated episode of parotitis 3 weeks post-completion.
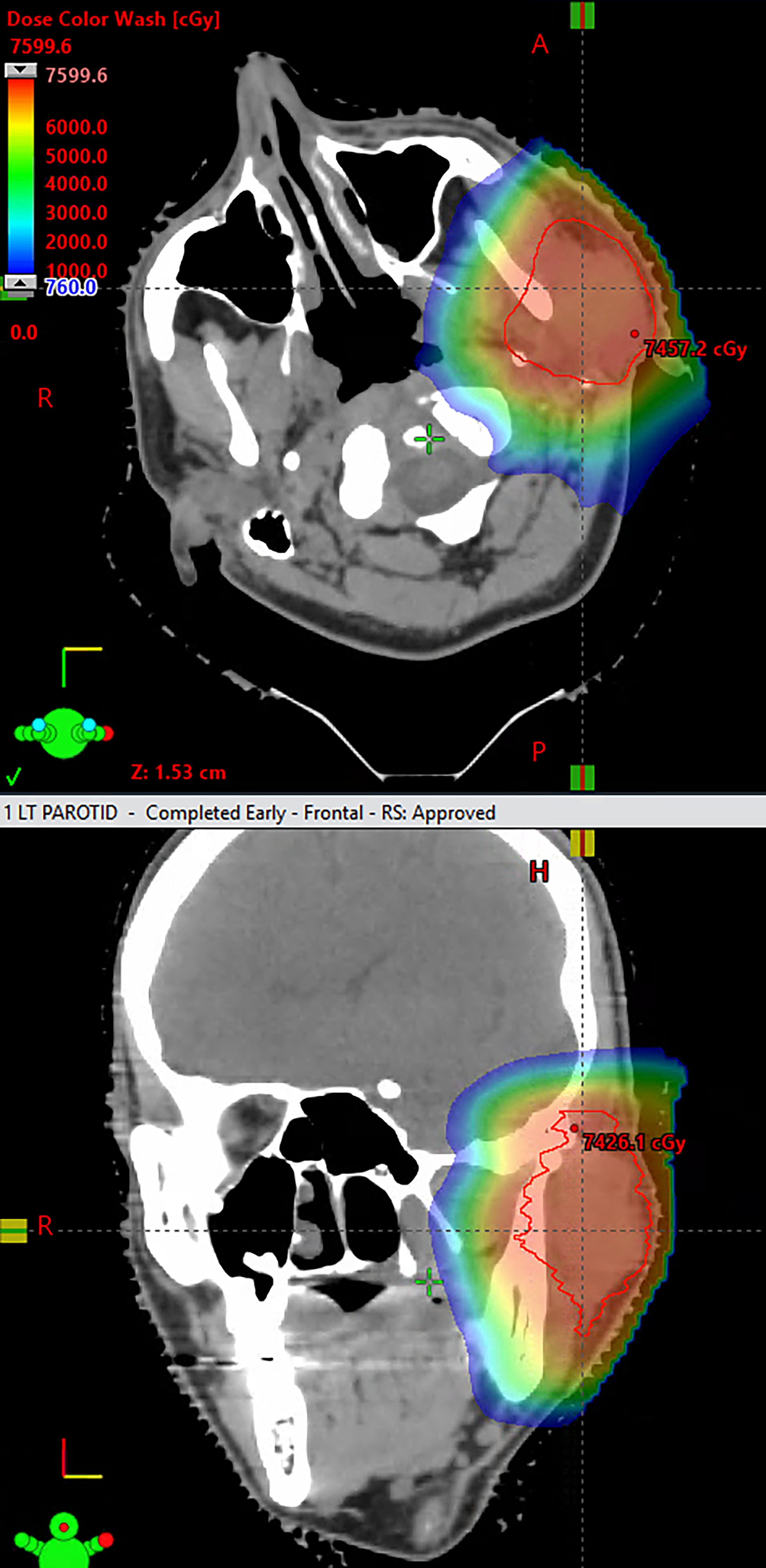
The patient presented 27 months later for mild dysphonia and left-ear discharge. MRI revealed a 2.5 cm mass in the left parotid gland, and fine needle aspiration confirmed recurrent non-keratinizing NPC that was CK5/6+, p40+, and Epstein-Barr virus-positive (EBV+). PET imaging showed a new hypermetabolic 3.9 × 3.4 cm lesion in the left deep parotid space with a standardized uptake value (SUV) of 14.0. Additionally, there was mild FDG uptake in a left cervical level 2 node measuring 0.7 × 0.6 cm with an SUV of 2.9. The case was discussed at tumor board, with a recommendation for salvage reirradiation. He was reirradiated with 70 Gy in 35 fractions using proton therapy (Figures 2, 3). After reirradiation, there was excellent clinical response, evidenced by decreased swelling on palpation with occasional production of exudate in his left external auditory canal.
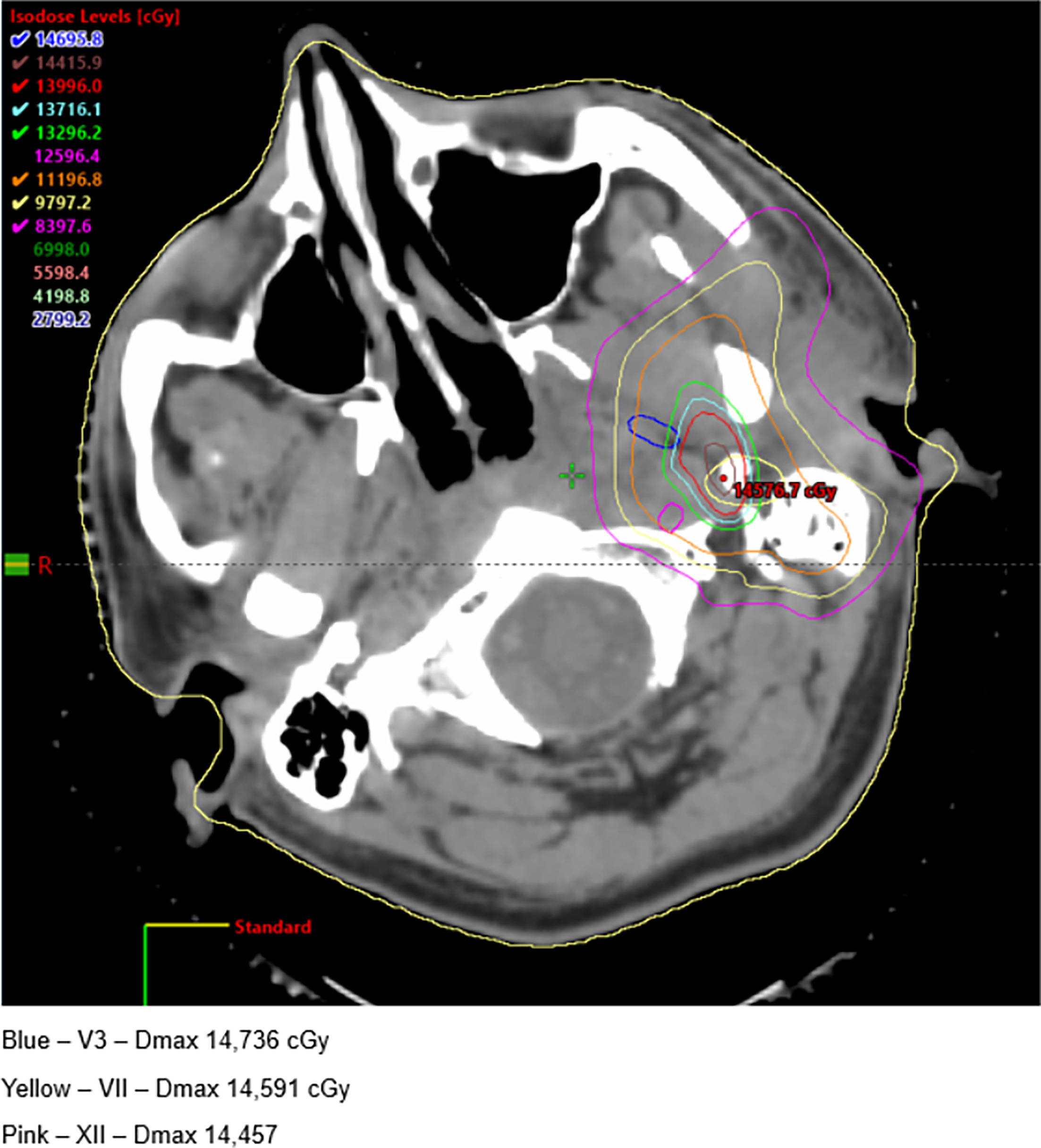
He began to experience hoarseness 3 months following the final dose of radiation. Laryngoscopy showed left vocal cord immobility with incomplete closure on phonation, deemed to be secondary to left cranial nerve X palsy. A month later, he presented with numbness of the left side of his tongue (left cranial nerve V3 palsy) and altered tongue mobility (L cranial nerve XII palsy), which was making it difficult to swallow. Following placement of a G-tube, the patient was referred to otolaryngology for vocal cord augmentation by injection medialization of the left vocal cord. A speech-language pathologist assisted with the patient’s care and recommended exercises to bolster oral/pharyngeal strength, swallow reflex, and voice control, with hopes to eventually wean from the G-tube. Then, 4 months later, he continued to have ongoing dysphonia and dysphagia, along with a new onset of palsies of nerves V3, VII, and XI, trismus, decreased sensation along the mandibular division of the trigeminal nerve, weakness of the left cervical division of the facial nerve, and atrophy of the left sternocleidomastoid and the left hemitongue. Radiation imaging confirmed radiation scarring of the left parapharyngeal and carotid spaces. MRI of his head and neck showed a loss of fat signal within the left parapharyngeal and left carotid fat space consistent with post-radiation scarring and a possible explanation of his left vocal-cord palsy. He continued to experience dysphonia and underwent left medialization thyroplasty of his left vocal cord. His voice improved, but with some weakness and reduced volume.
Discussion
Location vs Dose
The most common area of recurrence in NPC is locally (within the nasopharynx) or in cervical lymph nodes. In a retrospective study of 1852 patients, Xu et al. found that only 9 patients (4.9%) who were initially treated with intensity-modulated radiotherapy (IMRT) experienced intraparotid recurrence.1 Xiao et al. similarly found that the recurrence of NPC to the parotid gland was 6.9%.2 It is suspected that spread can occur through the lateral retropharyngeal lymph nodes and level 2 neck cervical lymph nodes through extracapsular spread. Our patient had left-sided positive nodes at levels 2B and 3 at initial diagnosis. During treatment planning, we did not include his left parotid. So, it is possible that parotid-sparing IMRT missed subclinical disease, even though the left parotid mean dose on this patient’s initial plan was 30 Gy (exceeding the goal constraint of <26 Gy mean dose). Perhaps an even higher dose was warranted, given the extent of this patient’s lymphadenopathy.
The patient’s cranial nerve palsies likely occurred due to high total doses of radiation to the skull base region and deep neck. Patients can be considered for reirradiation if they have a small volume of disease, but even the most “ideal” cases carry a risk of late toxicity.3 Dosing guidelines for reirradiation of the nasopharyngeal and head-and-neck regions do not account for cranial nerves and follow the recommendations applied to vital neurologic structures (brainstem, spinal cord, optic nerves).4,5 Given the proximity of recurrence to the carotid artery, we kept the dose below 125 Gy.
Proton vs Photon Therapy
Proton therapy has been shown to decrease radiation dose to at-risk organs.6 In a study of nonmetastatic NPC patients, Li et al. observed fewer acute and late side effects in participants who received proton therapy compared with photon therapy.7 In the reirradiation setting, Dionisi et al. evaluated 17 patients with recurrent NPC treated with protons and showed only one acute grade 1 and one late grade 2 cranial nerve palsy.8 In a larger, single-institution study, Lee et al. evaluated 242 patients with head and neck squamous cell carcinoma treated with protons in the reirradiation setting. Of those cases, 24 patients were diagnosed with cancer of the nasopharynx, nasal cavity, or sinuses. Although rates of 1 year overall survival (OS, 66.6%) and 2-year locoregional control (63.0%) were favorable, a considerable number of patients had grade 3, 4, and 5 late toxic effects.9 One explanation is that these patients are living longer, giving time for late effects to be realized.
Hyperfractionation vs Standard Fractionation
You et al. explored the role of hyperfractionation vs standard fractionation in recurrent NPC patients using IMRT in a multicenter, open-labeled, phase 3 trial. The hyperfractionation group received 65 Gy in 54 fractions with a minimum of 6 hours between fractions. The standard fractionation group received 60 Gy in 27 fractions. Hyperfractionation improved 3-year OS at 74.6% vs 55%, while decreasing grade 3 or worse radiation-induced toxicities.10 This new study makes a compelling case for the use of hyperfractionation in recurrent NPC.
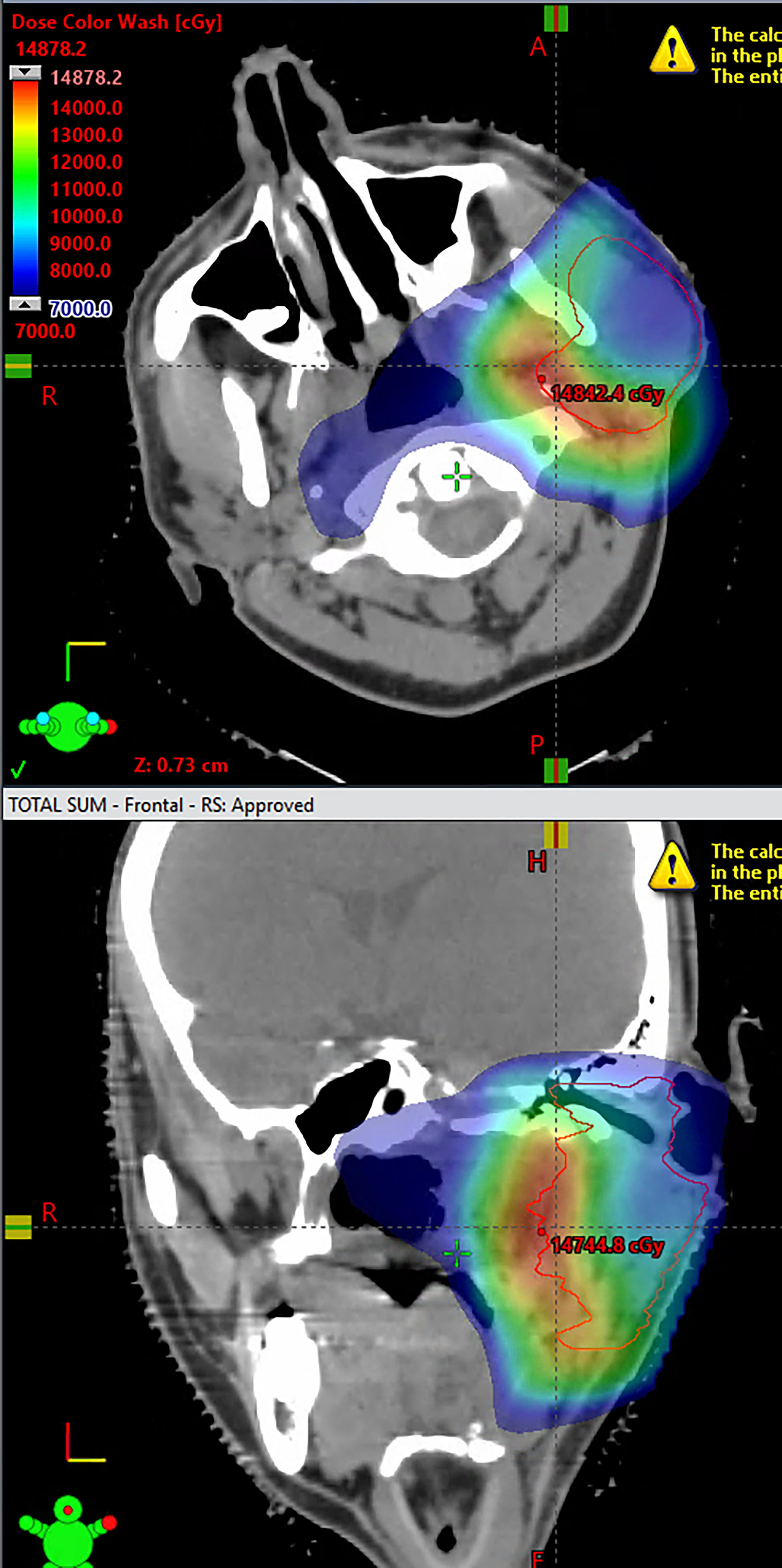
The cumulative dose to the area of overlap in our patient reached 140 Gy (Figure 4). This has proved successful from a local control standpoint, but the patient is now dealing with the late effects of having received 2 rounds of radiation, with the area of overlap existing primarily in the deep neck.
A recent, retrospective study found that radiation-induced hypoglossal nerve palsy occurs in 8.7% of nasopharyngeal cancer patients, with higher risks linked to high radiation doses and advanced T-stage.11 A D1cc constraint of <74 Gy could help limit this risk.12,13 A pre-IMRT review from a single institution reported a 14% rate of cranial nerve palsy after head and neck radiation, with a median onset of 7.7 years.14 While most studies show lower incidence rates, our patient continues to experience cranial nerve palsy, and full recovery seems unlikely given the extent of treatment. This underscores the importance of multidisciplinary survivorship care and highlights the complexity of balancing long-term disease control with its impact on quality of life.
Conclusion
NPC is a rare form of malignancy that remains treatable during primary presentation but becomes difficult to treat with recurrence. Here, we present a case of NPC in a 19-year-old patient, who, after receiving concurrent cisplatin and radiation therapy, developed recurrence in the left parotid gland. Salvage reirradiation was delivered using proton therapy. Afterward, the patient developed significant cranial nerve palsies. This case emphasizes the amount of attention that must be paid to fractionation scheme and dosage and also the fact that, even despite our meticulousness, late toxicities can and do occur. By optimizing the treatment plan and thoroughly assessing risks and benefits in conjunction with the patient, the treating radiation oncologist can best balance the chances of cure vs the risk of late side effects and optimize the patient’s quality of life.
References
- Xu Y, Zhang M, Yue Q. Analysis of rare periparotid recurrence after parotid gland-sparing intensity-modulated radiotherapy for nasopharyngeal carcinoma. Cancer/Radiothérapie. 2016;20(5):377-383. doi:10.1016/j.canrad.2016.05.012.
- Xiao X, Wu Y, Chen Y. Patterns and prognosis of regional recurrence in nasopharyngeal carcinoma after intensity-modulated radiotherapy. Cancer Med. 2023;12(2):1399-1408. doi:10.1002/cam4.5020.
- Simone C, Plastaras J, Jabbour S. Proton reirradiation: expert recommendations for reducing toxicities and offering new chances of cure in patients with challenging recurrence malignancies. Semin Radiat Oncol. 2020;30(3):253-261. doi:10.1016/j.semradonc.2020.02.007.
- Ward M, Koyfman S, Bakst R. Retreatment of recurrent or second primary head and neck cancer after prior radiation: executive summary of the american radium society appropriate use criteria. Int J Radiat Oncol Biol Phys. 2022;113(4):759-786. doi:10.1016/j.ijrobp.2022.03.034.
- Ng W, Soong Y, Ahn Y. International recommendations on reirradiation by intensity modulated radiation therapy for locally recurrent nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2021;110(3):682-695. doi:10.1016/j.ijrobp.2021.01.041.
- Lewis G, Holliday E, Kocak-Uzel E. Intensity-modulated proton therapy for nasopharyngeal carcinoma: decreased radiation dose to normal structures and encouraging clinical outcomes. Head Neck. 2016;38(suppl 1). doi:10.1002/hed.24341.
- Li X, Kitpanit S, Lee A. Toxicity profiles and survival outcomes among patients with nonmetastatic nasopharyngeal carcinoma treated with intensity-modulated proton therapy vs intensity-modulated radiation therapy. JAMA Netw Open. 2021;4(6). doi:10.1001/jamanetworkopen.2021.13205.
- Dionisi F, Croci S, Giacomelli I. Clinical results of proton therapy reirradiation for recurrent nasopharyngeal carcinoma. Acta Oncol. 2019;58(9):1238-1245. doi:10.1080/0284186X.2019.1622772.
- Lee A, Woods R, Mahfouz A. Evaluation of proton therapy reirradiation for patients with recurrent head and neck squamous cell carcinoma. JAMA Netw Open. 2023;6(1). doi:10.1001/jamanetworkopen.2022.50607.
- You R, Liu Y, Xie Y. Hyperfractionation compared with standard fractionation in intensity-modulated radiotherapy for patients with locally advanced recurrent nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet. 2023;401(10380):917-927. doi:10.1016/S0140-6736(23)00269-6.
- Au K, Ngan R, Ng A. Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in hong kong: a report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018;77:16-21. doi:10.1016/j.oraloncology.2017.12.004.
- Janssen S, Glanzmann C, Yousefi B. Radiation-induced lower cranial nerve palsy in patients with head and neck carcinoma. Mol Clin Oncol. 2015;3(4):811-816. doi:10.3892/mco.2015.558.
- Aggarwal P, Goepfert R, Garden A. Risk and clinical risk factors associated with late lower cranial neuropathy in long-term oropharyngeal squamous cell carcinoma survivors. JAMA Otolaryngol Head Neck Surg. 2021;147(5):469-478. doi:10.1001/jamaoto.2020.5269.
- Dong Y, Ridge J, Ebersole B. Incidence and outcomes of radiation-induced late cranial neuropathy in 10-year survivors of head and neck cancer. Oral Oncol. 2019;95:59-64. doi:10.1016/j.oraloncology.2019.05.014.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Acknowledgments
CH treated and managed the patient, and CH edited the manuscript. CB wrote the manuscript. All authors have read and approved the manuscript for publication.
Citation
. Multiple Cranial Nerve Palsies After Reirradiation With Proton Therapy in Nasopharyngeal Carcinoma: A Case Report. Applied Radiation Oncology. 2026. doi:10.37549/ARO-D-24-00030.