Neutropenic Colitis
Journal of Pediatric Case Reports — Vol. 1 , Issue 2
Published: April 10, 2026
1 School of Medicine, Wayne State University, Detroit, Michigan
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Neutropenic colitis is an uncommon but life-threatening complication that occurs in patients receiving cytotoxic chemotherapy, particularly for hematologic malignancies. Early recognition of symptoms, such as abdominal pain, fever, and diarrhea, is critical. Prompt diagnostic imaging plays a pivotal role in confirming the diagnosis and excluding other potential causes of abdominal symptoms. Early detection enables the timely initiation of appropriate treatment, including broad-spectrum antibiotics and supportive care, which is essential to reduce morbidity and mortality associated with this condition. It is identified clinically or radiographically.
Keywords
gastrointestinal, intestines, oncology, immune suppression
Categories
Case Summary
An infant with B-cell acute lymphoblastic leukemia treated with chemotherapy was neutropenic. The patient developed worsening tachypnea, abdominal distention, abdominal wall erythema and edema, and lactic acidosis.
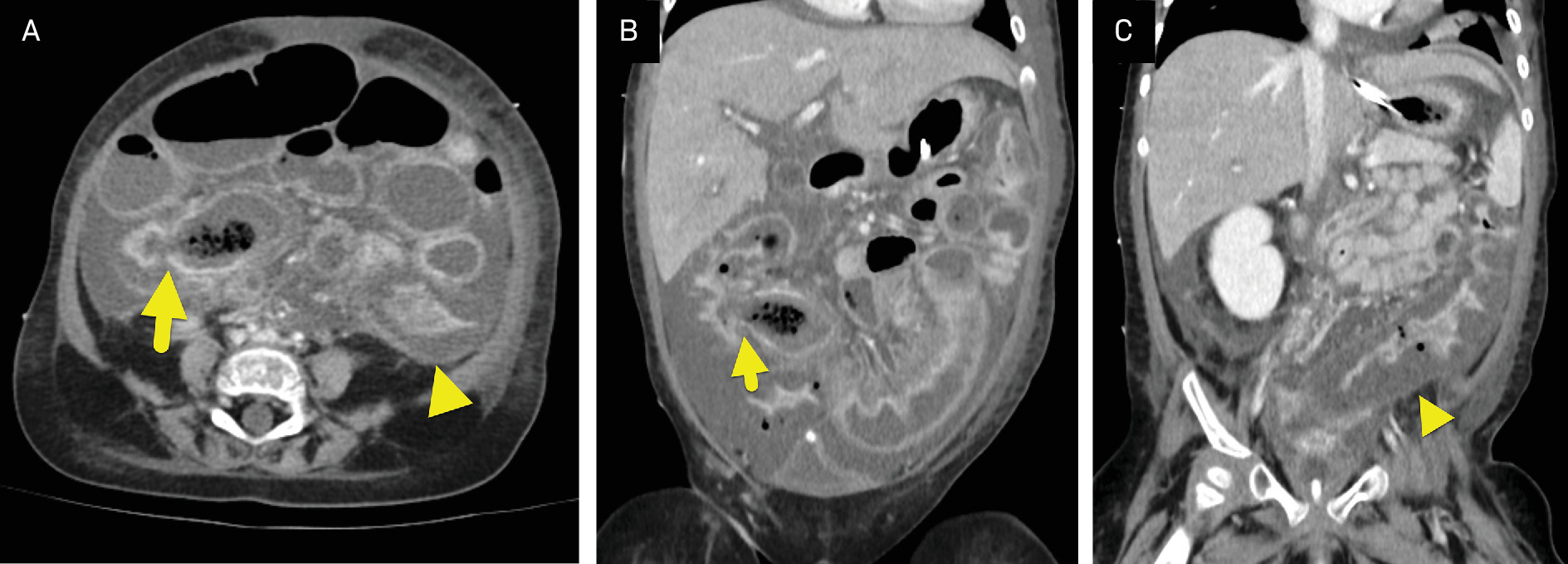
Imaging Findings
Abdominal CT (Figure 1) showed dilated bowel loops with diffuse colonic wall thickening, wall edema, and moderate ascites.
Diagnosis
Neutropenic colitis
The clinical differential diagnosis includes infectious colitis, ischemic colitis, appendicitis, inflammatory bowel disease, graft-versus-host disease, and cytomegalovirus colitis.
Discussion
Neutropenic colitis, also known as typhlitis, is a life-threatening inflammatory condition of the bowel, typically involving the cecum, ascending colon, and terminal ileum in immunocompromised patients. 1 The condition is characterized by mucosal injury, bowel wall edema, and inflammation, compounded by profound neutropenia that compromises the body’s ability to mount an effective immune response.
It most commonly occurs in patients undergoing cytotoxic chemotherapy for hematologic malignancies, particularly acute leukemia. 2,3 However, it has also been reported in patients treated for lymphoma, multiple myeloma, and solid tumors, as well as in individuals with nonmalignant causes of neutropenia, including aplastic anemia, cyclic neutropenia, agranulocytosis, Felty syndrome, thalassemia minor, systemic lupus erythematosus, and HIV infection. 3,4 In hospitalized patients with hematologic malignancies, the reported prevalence of neutropenic colitis is approximately 2.6%. 4
Neutropenic colitis is thought to result from chemotherapy-induced mucosal injury combined with profound neutropenia, which predisposes patients to bacterial invasion of the bowel wall. 2,5 Symptoms typically develop within 2 weeks after completing chemotherapy and include abdominal pain, fever, and diarrhea. 2,5 When neutropenia is identified during laboratory monitoring and clinical symptoms are present, diagnostic imaging should be performed to evaluate for neutropenic colitis.
The diagnostic criteria for neutropenic colitis include the presence of neutropenia (absolute neutrophil count < 500 × 10⁶ cells/L), bowel wall thickening greater than 4 mm on imaging, and exclusion of alternative diagnoses. 3 CT and/or abdominal US is the initial imaging of choice for diagnosis, as it not only confirms bowel wall thickening but also evaluates for other causes of abdominal pain, such as appendicitis or gastroenteritis. 4,6 In addition to wall thickening, imaging findings may include cecal or colonic dilation, an inflammatory mass, pericolic inflammation/abscess, pneumatosis intestinalis, or perforation. 2,6
Abdominal radiographs in neutropenic colitis may demonstrate a dilated, atonic cecum and ascending colon filled with liquid or gas. 6 US findings supportive of the diagnosis include bowel wall thickening, pericolic fluid collections, increased echogenicity of the bowel wall or mesenteric fat, the presence of 3 or more enlarged mesenteric lymph nodes greater than 5 mm in short axis, hyperemia on Doppler or contrast-enhanced US, and abnormal peristalsis. 6,7 US is commonly utilized in pediatric populations and can be as accurate as CT in detecting bowel wall thickening and increased vascularity of the bowel wall and mesentery, thereby aiding in the diagnosis of neutropenic colitis. 6
Major complications and causes of mortality in neutropenic colitis include necrotizing bowel perforation, gastrointestinal bleeding, and sepsis. 5,8 Even with appropriate management, mortality rates range from 23% to 31%. 8 Prompt imaging is critical at the onset of symptoms to reduce morbidity and mortality. Early detection is possible through careful adherence to chemotherapy surveillance and laboratory monitoring protocols.
Treatment for neutropenic colitis includes broad-spectrum antibiotics to address potential pathogens. 2,8 Supportive care is equally important, with interventions such as fluid resuscitation, correction of electrolyte imbalances, and bowel rest to protect and promote healing of the intestinal mucosa. 2,8 These measures aim to stabilize the patient and allow for mucosal recovery while minimizing the risk of further complications.
Conclusion
Neutropenic colitis is an uncommon but life-threatening complication that occurs in patients receiving cytotoxic chemotherapy, particularly for hematologic malignancies. Early recognition of symptoms, such as abdominal pain, fever, and diarrhea, is critical. Prompt diagnostic imaging plays a pivotal role in confirming the diagnosis and excluding other potential causes of abdominal symptoms. Early detection enables the timely initiation of appropriate treatment, including broad-spectrum antibiotics and supportive care, which is essential to reduce morbidity and mortality associated with this condition.
References
- Bertozzi G, Maiese A, Passaro G. Neutropenic enterocolitis and sepsis: towards the definition of a pathologic profile. Medicina (Kaunas). 2021;57(6):638. doi:10.3390/medicina57060638.
- Rodrigues F, Dasilva G, Wexner S. Neutropenic enterocolitis. World J Gastroenterol. 2017;23(1):42-47. doi:10.3748/wjg.v23.i1.42.
- Nesher L, Rolston K. Neutropenic enterocolitis, a growing concern in the era of widespread use of aggressive chemotherapy. Clin Infect Dis. 2013;56(5):711-717. doi:10.1093/cid/cis998.
- McCarville M, Adelman C, Li C. Typhlitis in childhood cancer. Cancer. 2005;104(2):380-387. doi:10.1002/cncr.21134.
- Benedetti E, Traverso G, Pucci G. Impact of different chemotherapy regimens on intestinal mucosal injury assessed with bedside ultrasound: a study in 213 AML patients. Front Oncol. 2023;13. doi:10.3389/fonc.2023.1272072.
- Tamburrini S, Setola F, Belfiore M. Ultrasound diagnosis of typhlitis. J Ultrasound. 2019;22(1):103-106. doi:10.1007/s40477-018-0333-2.
- Hwang J. Emergency ultrasonography of the gastrointestinal tract of children. Ultrasonography. 2017;36(3):204-221. doi:10.14366/usg.16052.
- Machado N. Neutropenic enterocolitis: a continuing medical and surgical challenge. N Am J Med Sci. 2010;2(7):293-300.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Neutropenic Colitis. Journal of Pediatric Case Reports. 2026;1(2). doi:10.37549/JPCR-26-0084.