Nontraumatic Medial Orbital Blowout Fracture
Applied Radiology — Vol. 55 , Issue 4
Published: January 29, 2026
1 Department of Radiology, Advent Health, Orlando, Florida
* Corresponding author: Chad Jones (chad.jones.md@adventhealth.com)
Categories
Case Summary
A healthy adult presented with progressive left eye swelling, left eye pain, and bloody mucus following forceful nose blowing. The physical exam was remarkable for significant edema and tenderness to palpation of the left upper eyelid and mild discomfort with upward gaze. Extraocular movements were intact. The exam was negative for skin erythema/ecchymosis, scleral erythema, subconjunctival hemorrhage, hypopyon/hyphema, and eye discharge.
Imaging Findings
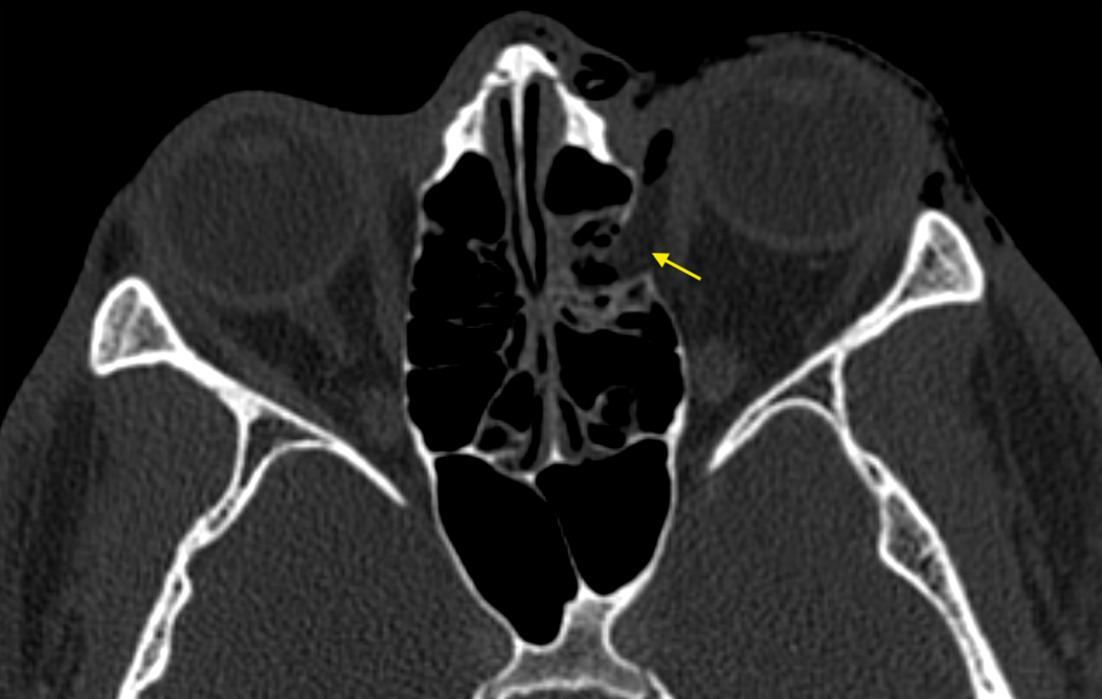
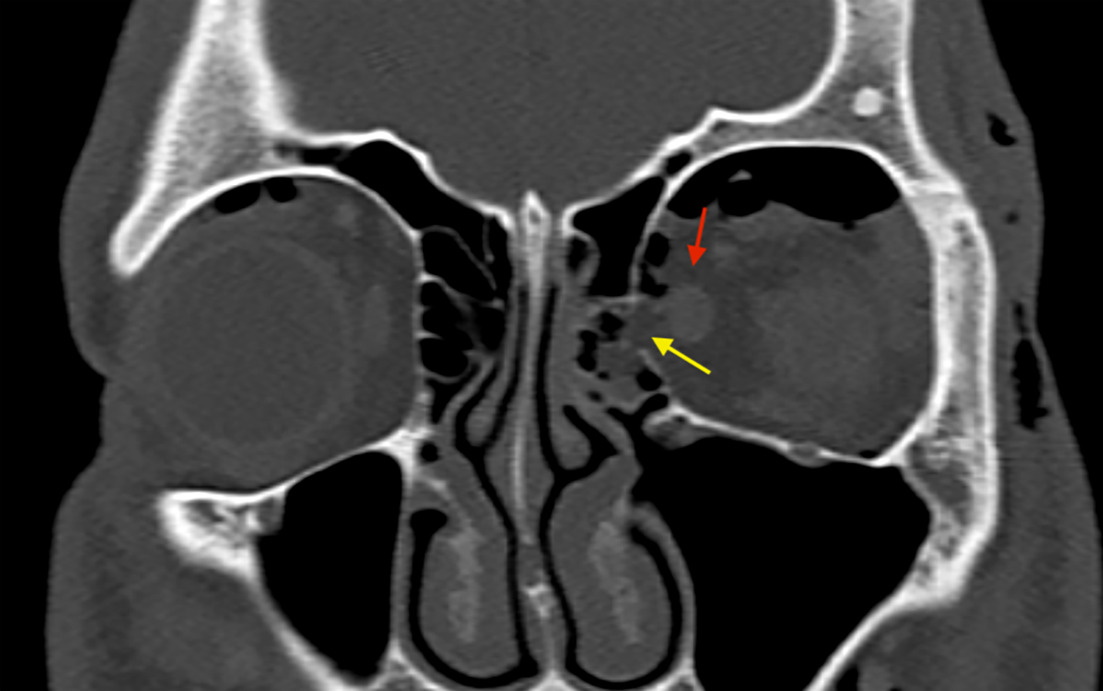
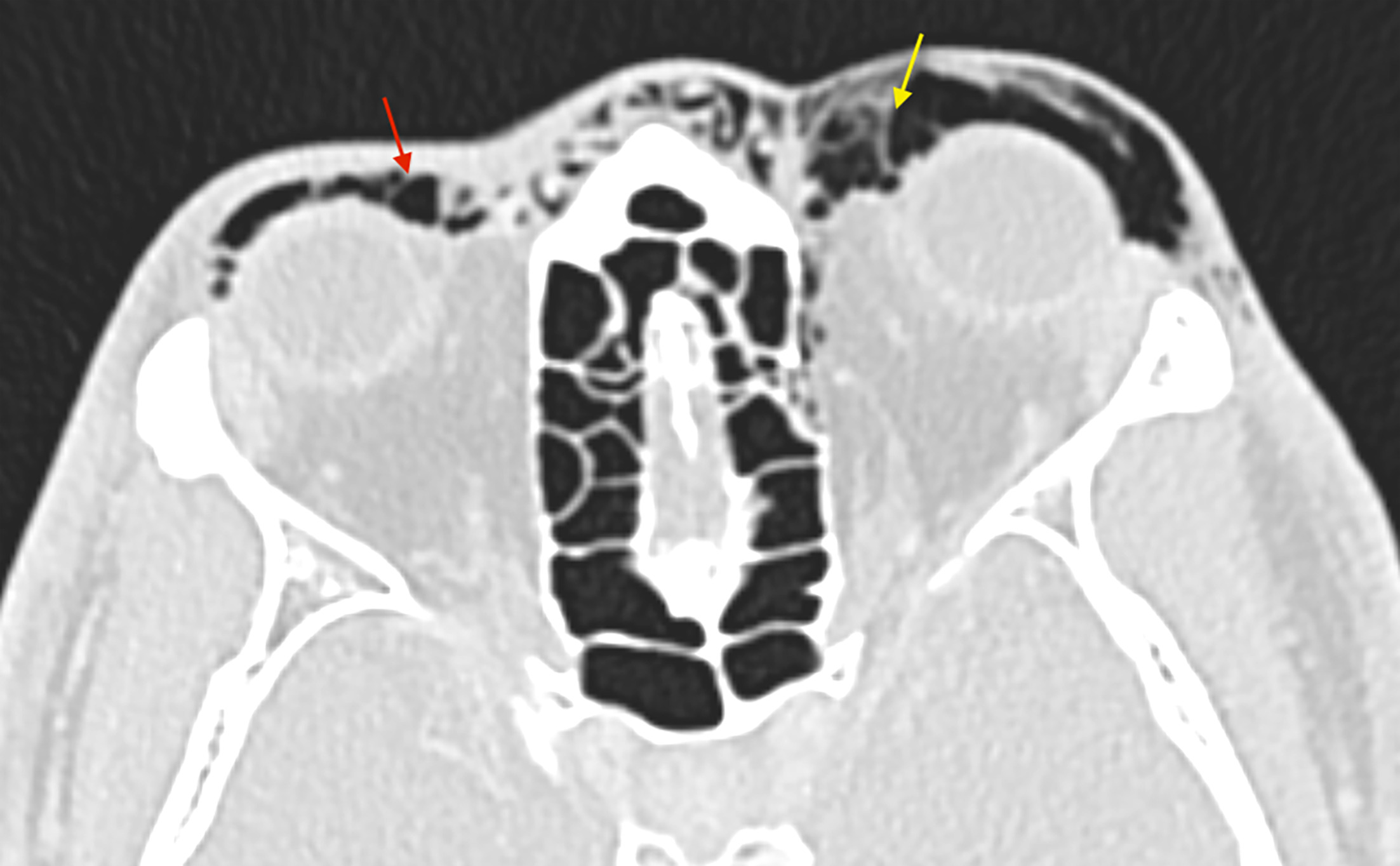
Contrast-enhanced thin-slice CT of the maxillofacial bones demonstrated a left medial orbital wall fracture with herniation of fat (Figure 1). There was mild left proptosis without evidence of extraocular muscle entrapment (Figure 2). A moderate amount of orbital and periorbital emphysema was visualized that tracked to the contralateral side (Figure 3).
Diagnosis
Nontraumatic medial orbital wall blowout fracture
Discussion
The orbit is a complex anatomic structure, and recognizing fracture patterns in this region is crucial to guide proper management. Pure orbital fractures are defined as those limited to the internal orbit, while impure orbital fractures involve the orbital rim and require realignment prior to surgical reconstruction.1 The majority of pure internal orbital fractures are blowout fractures involving the orbital floor or medial orbital wall.1 The mechanism of these fractures is most commonly secondary to direct trauma, whereby the increase in intraorbital pressure overcomes the structural integrity of the orbital bones.
Orbital blowout fracture in the absence of trauma, as presented here, is rare. A review of the literature reveals just a few other cases of orbital blowout fractures from nose blowing2-7; however, the fractures in this case occurred at the orbital floor rather than at the medial orbital wall. A similar case of atraumatic medial orbital wall fracture was found in our review,8 but in that case the orbital emphysema was unilateral.
We believe our case is a unique presentation where the less-common atraumatic medial orbital fracture caused orbital emphysema, which tracked from the side of injury to the contralateral orbit.
Increased intrasinus pressure would ordinarily be expected to cause a blow-in fracture, displacing the bone fragment into the intraconal space. In all the reviewed cases of blowout fractures, including ours, the fragment was displaced into the sinus. We hypothesize that these types of fractures initially occur as blow-in fractures secondary to increased intrasinus pressure. However, once sinus pressure is normalized, the pressure gradient is reversed, and the fracture fragment is displaced into the sinus, giving the appearance of a blowout fracture.
Most reported cases of atraumatic orbital blowout fracture did not require surgical intervention. Only antibiotic prophylaxis was necessary to protect against sinus pathogens, which may enter the orbit through the fracture defect.
Owing to a large fracture defect causing significant risk of hypophthalmos, orbital floor reconstruction was performed in one reviewed case.4 While no cases of atraumatic medial orbital wall fractures requiring surgical intervention were found, scrutinizing the medial rectus muscle, medial canthal ligament, and the lacrimal duct system to evaluate for emergent pathology is important. Injury to these structures can present clinically as restricted and painful ocular abduction, diplopia, and enophthalmos, all of which may warrant surgical exploration.9
Moreover, while most cases of orbital emphysema resolve spontaneously, rapidly increasing burden of emphysema can lead to acute orbital compartment syndrome, leading to permanent vision loss from optic nerve stretching or vascular compromise. Short-term follow-up and strict return precautions should be implemented in these cases to prevent these adverse patient outcomes.
Conclusion
While orbital blowout fractures and orbital emphysema are most commonly caused by direct trauma, these entities should not be ruled out in atraumatic patients. Those with chronic sinusitis/rhinitis or congenitally thin sinus bones are at increased risk of barotrauma-induced fracture. Awareness of atraumatic orbital fractures can reduce unnecessary medical investigations and potentially shorten hospitalization. A careful examination of the orbital bones and surrounding structures with dedicated thin-slice orbital CT should always be performed in the presence of clinical signs of orbital injury.
References
- Dreizin D, Nam A, Diaconu S. Multidetector CT of midfacial fractures: classification systems, principles of reduction, and common complications. Radiographics. 2018;38(1):248-274. doi:10.1148/rg.2018170074.
- Mohebbi M, Shea C. Orbital blowout fracture from nose blowing. Clin Pract Cases Emerg Med. 2017;1(1):74-75. doi:10.5811/cpcem.2016.11.30820.
- Jawaid M. Orbital emphysema: nose blowing leading to a blown orbit. BMJ Case Rep. 2015;2015. doi:10.1136/bcr-2015-212554.
- Sandhu R, Shah A. Nontraumatic orbital floor fracture after nose blowing. Radiol Case Rep. 2016;11(1):1-3. doi:10.1016/j.radcr.2015.12.006.
- Oluwole M, White P. Orbital floor fracture following nose blowing. Ear Nose Throat J. 1996;75(3):169-170. doi:10.1177/01455613960750031.
- Watanabe T, Kawano T, Kodama S, Suzuki M. Orbital blowout fracture caused by nose blowing. Ear Nose Throat J. 2012;91(1):24-25. doi:10.1177/014556131209100108.
- Rahmel B, Scott C, Lynham A. Comminuted orbital blowout fracture after vigorous nose blowing that required repair. Br J Oral Maxillofac Surg. 2010;48(4). doi:10.1016/j.bjoms.2010.02.004.
- Ariyoshi Y, Naito H, Yumoto T. Orbital emphysema as a consequence of forceful nose-blowing: report of a case. Case Rep Emerg Med. 2019;2019. doi:10.1155/2019/4383086.
- Segrest D, Dortzbach R. Medial orbital wall fractures: complications and management. Ophthalmic Plast Reconstr Surg. 1989;5(2):75-80. doi:10.1097/00002341-198906000-00001.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Nontraumatic Medial Orbital Blowout Fracture. Applied Radiology. 2026;55(4). doi:10.37549/AR-D-25-0130.