1 California Health Sciences University College of Osteopathic Medicine, Clovis, California
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Ovarian torsion is a surgical emergency that occurs when the ovary twists around its adnexal ligaments, leading to possible ischemia and necrosis. It often presents with a sudden onset of unilateral lower abdominal pain and nausea/vomiting. Prompt and accurate diagnosis is crucial to save the ovary. Imaging is not specific. However, either US or MRI is often performed to help make the diagnosis and exclude other entities in the differential diagnosis. Laparoscopic detorsion is currently the preferred therapy.
Keywords
genitourinary, medical emergency, ovarian
Categories
Case Summary
An adolescent, postpubertal girl with a history of prior right ovarian torsion presented to the emergency room with 2 weeks of intermittent left-sided abdominal pain. On the day of admission, she had a sudden worsening of the pain with associated emesis.
Imaging Findings
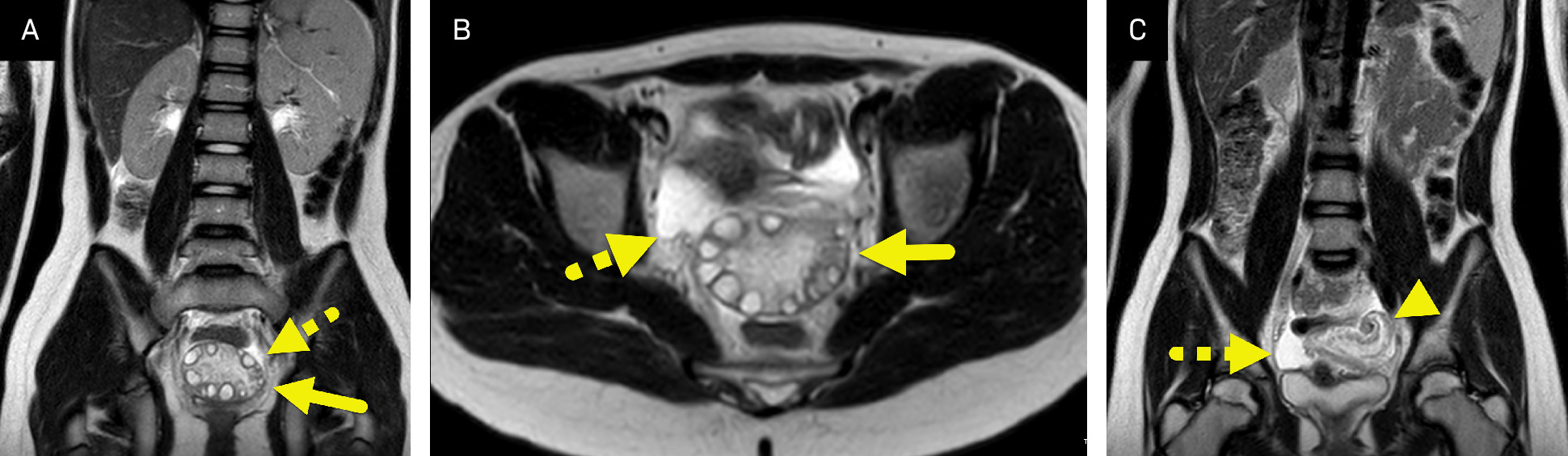
MRI of the abdomen and pelvis (Figure 1) showed an enlarged, edematous left ovary. Follicles were prominent and located at the periphery of the ovary. The infundibulopelvic ligament was twisted.
Diagnosis
Ovarian torsion.
The differential diagnosis for lower abdominal pain in an adolescent girl includes appendicitis, hemorrhagic or ruptured ovarian cyst, ectopic pregnancy, and tubo-ovarian abscess.
Discussion
Ovarian torsion is a medical emergency caused by an ovary twisting around the adnexal ligaments, mainly the infundibulopelvic ligament and utero-ovarian ligament. 1 It leads to venous congestion and edema followed by ischemia and necrosis of the ovary and fallopian tube if left untreated. 1 While ovarian torsion can affect any female with ovaries, 15% of cases occur in pediatric patients; it accounts for 2.7-4% of acute abdominal pain in girls. 1
In children, ovarian torsion is more likely to occur in a normal ovary, while in adults there is a higher incidence of an associated ovarian mass. In addition, pediatric ovarian torsion is more likely to result in a delayed diagnosis due to unrecognized or nonspecific symptoms. Salvage of the involved ovary is now reported to be as high as 86-97% due to increased clinical awareness and detorsion operative procedures.
In adults, ovarian torsion is often associated with a mass that serves as a lead point; it can also occur spontaneously. Spontaneous ovarian torsion accounts for 25% of pediatric cases and only 3% of adults. 1,2 This tendency for spontaneous torsion in pediatric patients may be due to the small anatomical size of the uterus and the relatively long ovarian ligaments. 1 This hypothesis is supported by the fact that right-sided ovarian torsion is more frequent due to longer mesosalpinx and utero-ovarian ligament. 1 The risk of torsion is increased when the mass is benign since malignant lesions are often anchored to nearby tissues, limiting their mobility. 1 Common masses that can serve as a lead point for torsion include teratomas, dominant follicles, and hemorrhagic cysts. 1
Ovarian torsion is a surgical emergency and requires a prompt diagnosis to prevent impaired or loss of fertility. 3 However, due to its nonspecific presentation combined with variable imaging findings, diagnosis is difficult to make. 1 Patients most commonly present with an acute onset of pelvic or lower abdominal pain that is localized to one side. 1 Other symptoms include low-grade fever, mild tachycardia, nausea, and vomiting. 1 The presence of nausea and vomiting are key features helping differentiate adnexal torsion from other causes of acute abdominal pain. While most laboratory tests are normal, slight leukocytosis and an elevated C-reactive protein (CRP) can be seen. 1 This is important because leukocytosis combined with vomiting and elevated CRP has been shown to increase the risk of ovarian ischemia. 4 The protean symptoms and the lack of specific laboratory tests lead to a broad differential diagnosis, which can delay diagnosis and treatment. 2
Imaging can play a complementary role in the diagnosis of torsion and can help exclude other causes of abdominal pain. Transabdominal US is the most widely used initial imaging modality to diagnose ovarian torsion in girls. 1 The transabdominal approach is used to avoid the pain and potential psychologic trauma associated with the transvaginal approach. The criterion for transvaginal imaging varies by institution but may be dependent on patient age, prior gynecologic examination, or prior sexual activity. On US, the most specific finding is a unilateral enlarged ovary. Studies in postmenarchal girls have reported that an adnexal ratio (defined as the volume of the affected ovary/volume of the unaffected ovary) >15-20 is predictive of torsion. 5,6 A more recent study has stated that an ovarian volume ratio of >2.5 demonstrates the best predictive accuracy for the diagnosis of torsion in premenarchal girls with a sensitivity of 100%, specificity of 94%, and an area under the curve of 0.991. 7 Other potential findings include a heterogeneous appearance of the ovary due to edema and peripherally located follicles from stromal edema. 1 A “Whirlpool sign” may be present, showing the twisting vascular pedicle. 6 Doppler flow information is of limited value because the ovary has a dual arterial blood supply from the ovarian and uterine arteries. Even though Doppler interrogation is often performed, the presence or absence of Doppler flow cannot help rule in or rule out torsion. 8,9
While US is considered the first-line imaging test, its reported performance is middling. A systematic review in adult women showed US to have a sensitivity of 79% and specificity of 76. 10 One systematic review of pediatric patients showed that its overall sensitivity was 79%. 11 This is better than a more recent single institution study that reported a sensitivity of 34%, specificity of 72%, positive predictive value of 49% and negative predictive value of 87%. 12 Other pediatric-based studies have discordant results. One study described the sensitivity of US as 51% while another described a sensitivity of 90.9% and specificity of 68.7%.
Recently, MRI has been used as the primary modality to diagnose ovarian torsion at some institutions. This shift has occurred for several reasons. First, adolescent girls with abdominal pain wait significantly longer in the emergency room due to the need to fill the urinary bladder for the transabdominal approach. Second, the excess wait time, coupled with the cost of performing multiple US studies to exclude all the items in the differential diagnosis of an adolescent girl with lower abdominal pain, has made MRI a more cost-effective modality. Finally, the time required to perform an MRI for acute abdominal pain has decreased dramatically over the past decade. This decreased time for imaging has helped improve access for MRI, allowing patients to be imaged in between patients already on the MRI schedule. 13 Findings of ovarian torsion on MRI include an enlarged ovary, surrounding edema, the presence of an ovarian mass, and engorgement and twisting of the ovarian pedicle. Deviation of the uterus and adnexa toward the side of torsion has been described as a finding. However, studies have shown that this finding is neither sensitive nor specific. Several studies have been performed comparing the diagnostic accuracy of US and MRI in the diagnosis of ovarian torsion. One systematic review showed that for adult women US had a pooled sensitivity and specificity of 79% and 76% while MRI had a sensitivity and specificity of 81% and 91%. 10 In one study performed in children who had already received an inconclusive US, MRI was able to diagnose adnexal torsion with a sensitivity of 100%, specificity of 94%, and accuracy of 96%. 14
CT can be used as part of the diagnostic workup of a girl with abdominal pain. While findings of ovarian torsion may be present on CT, this modality is less accurate than US or MRI. A different pediatric-based meta-analysis found that CT has a sensitivity of only 42% in diagnosing ovarian torsion. 11 Findings of ovarian torsion on CT are like those on MRI.
Ovarian torsion is typically treated with laparoscopic detorsion. 1 In the past, oophorectomy was performed if the torsed ovary showed any sign of necrosis. 1 This was mainly due to the belief that the necrotic tissue was nonviable. 15 However, studies have shown that necrotic-appearing ovaries may show normal blood flow and follicular development 6 weeks after surgery. 1 Other studies have demonstrated that patients can become pregnant following ovarian detorsion. 16 These findings have led to current guidelines advocating for detorsion instead of oophorectomy. 16
Conclusion
Ovarian torsion is a surgical emergency that occurs when the ovary twists around its adnexal ligaments, leading to possible ischemia and necrosis. It often presents with a sudden onset of unilateral lower abdominal pain and nausea/vomiting. Prompt and accurate diagnosis is crucial to save the ovary. Imaging is not specific. However, either US or MRI is often performed to help make the diagnosis and exclude other entities in the differential diagnosis. Laparoscopic detorsion is currently the preferred therapy.
References
- Childress K, Dietrich J. Pediatric ovarian torsion. Surg Clin North Am. 2017;97(1):209-221. doi:10.1016/j.suc.2016.08.008.
- Tielli A, Scala A, Alison M. Ovarian torsion: diagnosis, surgery, and fertility preservation in the pediatric population. Eur J Pediatr. 2022;181(4):1405-1411. doi:10.1007/s00431-021-04352-0.
- Sintim-Damoa A, Majmudar A, Cohen H, Parvey L. Pediatric ovarian torsion: spectrum of imaging findings. Radiographics. 2017;37(6):1892-1908. doi:10.1148/rg.2017170026.
- Tsai J, Lai J, Lin Y. Characteristics and risk factors for ischemic ovary torsion in children. Children. 2022;9(2). doi:10.3390/children9020206.
- Linam L, Darolia R, Naffaa L. US findings of adnexal torsion in children and adolescents: size really does matter. Pediatr Radiol. 2007;37(10):1013-1019. doi:10.1007/s00247-007-0599-6.
- Servaes S, Zurakowski D, Laufer M, Feins N, Chow J. Sonographic findings of ovarian torsion in children. Pediatr Radiol. 2007;37(5):446-451. doi:10.1007/s00247-007-0429-x.
- Hartman S, Prieto J, Naheedy J. Ovarian volume ratio is a reliable predictor of ovarian torsion in girls without an adnexal mass. J Pediatr Surg. 2021;56(1):180-182. doi:10.1016/j.jpedsurg.2020.09.031.
- Ngo A, Otjen J, Parisi M. Pediatric ovarian torsion: a pictorial review. Pediatr Radiol. 2015;45(12):1845-1855. doi:10.1007/s00247-015-3385-x.
- Gounder S, Strudwick M. Multimodality imaging review for suspected ovarian torsion cases in children. Radiography. 2021;27(1):236-242. doi:10.1016/j.radi.2020.07.006.
- Wattar B, Rimmer M, Rogozinska E. Accuracy of imaging modalities for adnexal torsion: a systematic review and meta-analysis. BJOG. 2021;128(1):37-44. doi:10.1111/1471-0528.16371.
- Rey-Bellet Gasser C, Gehri M, Joseph J, Pauchard J. Is it ovarian torsion? A systematic literature review and evaluation of prediction signs. Pediatr Emerg Care. 2016;32(4):256-261. doi:10.1097/PEC.0000000000000621.
- Lawrence A, Fallat M, Hewitt G. Factors associated with torsion in pediatric patients with ovarian masses. J Surg Res. 2021;263:110-115. doi:10.1016/j.jss.2020.12.058.
- Epstein K, Trout A, Debnath P. Rapid, free-breathing non-contrast MRI for first-line imaging evaluation of ovarian torsion in the emergency department. Pediatr Radiol. 2024;54(2):228-235. doi:10.1007/s00247-023-05827-y.
- Rougier E, Mar W, Della Valle V. Added value of MRI for the diagnosis of adnexal torsion in children and adolescents after inconclusive ultrasound examination. Diagn Interv Imaging. 2020;101(11):747-756. doi:10.1016/j.diii.2020.04.015.
- Santos X, Cass D, Dietrich J. Outcome following detorsion of torsed adnexa in children. J Pediatr Adolesc Gynecol. 2015;28(3):136-138. doi:10.1016/j.jpag.2014.04.002.
- Dasgupta R, Renaud E, Goldin A. Ovarian torsion in pediatric and adolescent patients: a systematic review. J Pediatr Surg. 2018;53(7):1387-1391. doi:10.1016/j.jpedsurg.2017.10.053.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Ovarian Torsion. Applied Radiology. 2025. doi:10.37549/JPCR-25-0045.