Pancreaticobiliary Maljunction
Applied Radiology
Published: December 24, 2025
1 University of São Paulo Medical School, São Paulo, São Paulo, Brazil
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pancreaticobiliary maljunction is a rare congenital anomaly occurring when the junction of the pancreatic and biliary ducts occurs outside of the duodenal wall. Patients with this anomaly have a higher risk of acute pancreatitis and biliary tract cancer. Therefore, patients ultimately undergo prophylactic surgery.
Keywords
abdomen, congenital, pancreaticobiliary maljunction, pancreatitis, biliary tract cancer
Categories
Case Summary
An infant presented with acute onset of abdominal pain, worse after eating. On laboratory examination, liver and pancreatic enzymes were elevated.
Imaging Findings
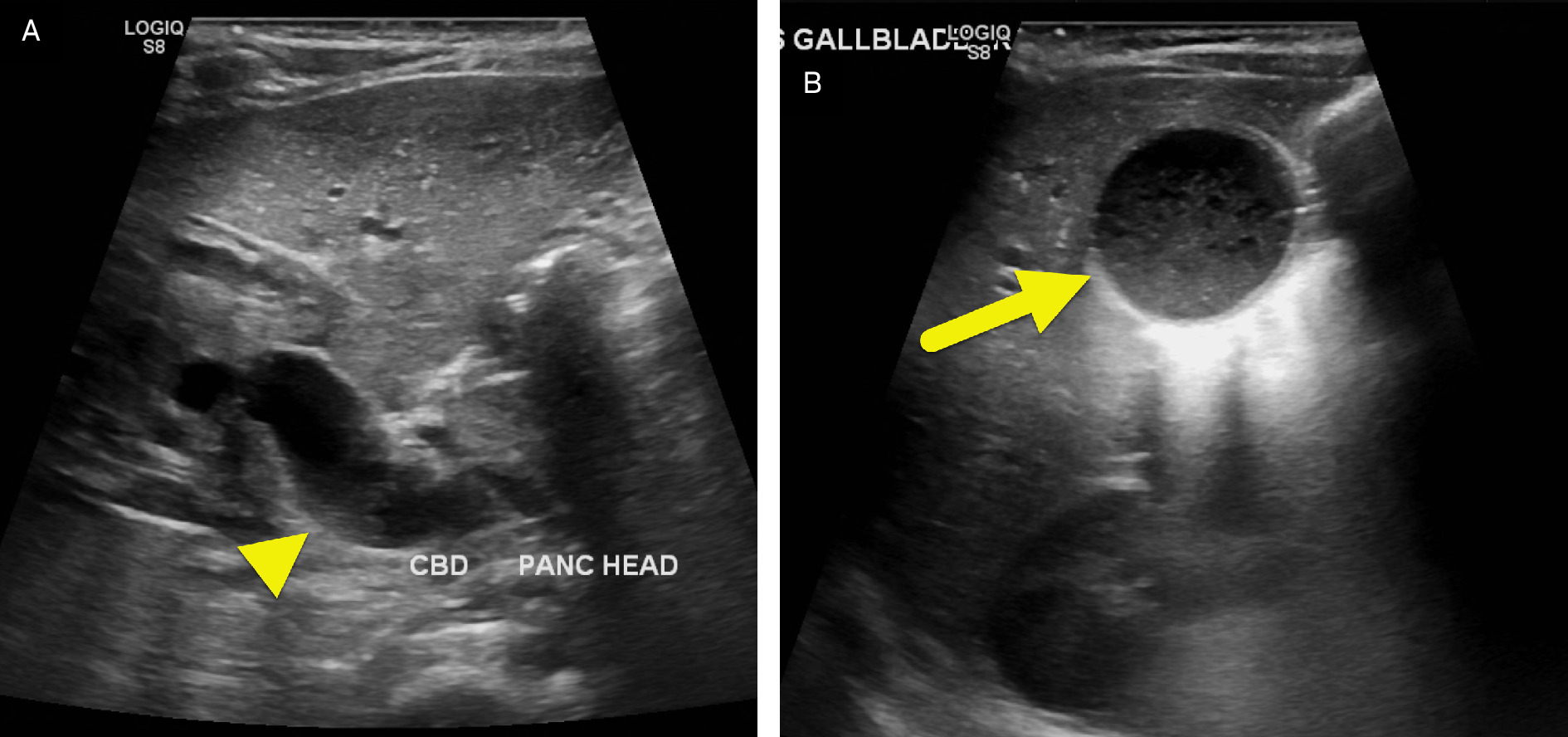
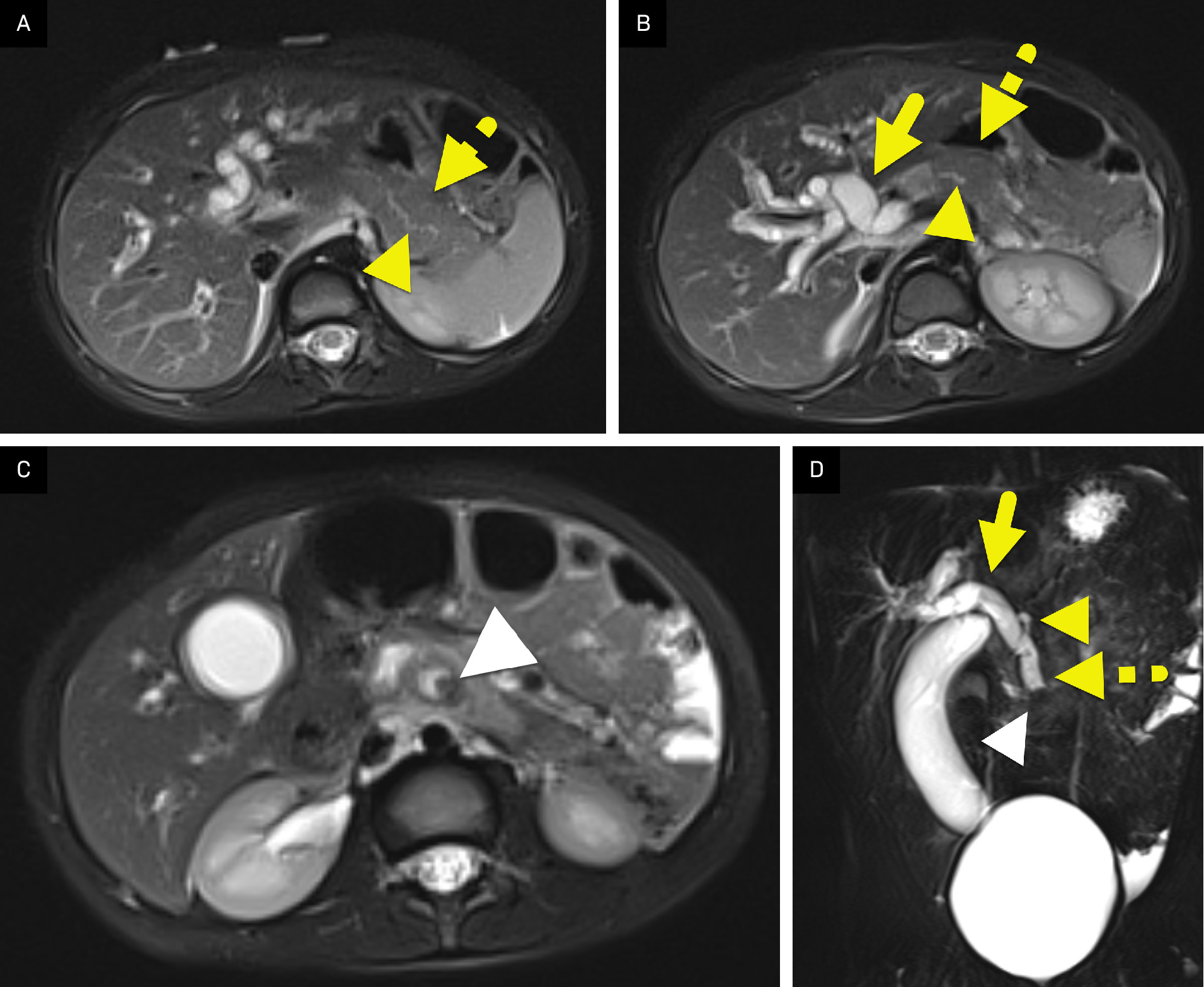
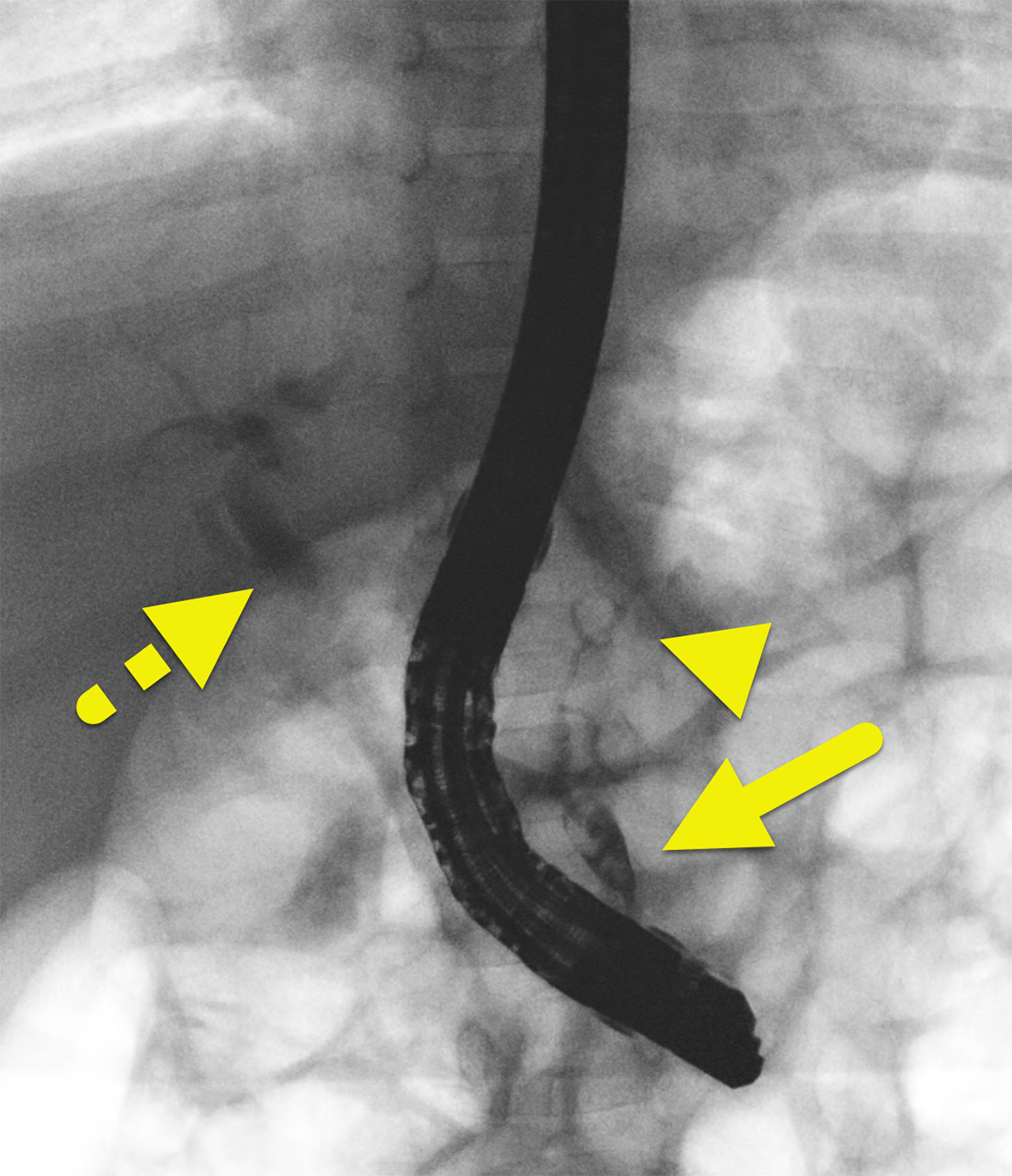
Abdominal US (Figure 1) showed marked dilation of the common bile duct with debris in the gallbladder. No stone was visible. Subsequent MR cholangiopancreatography (MRCP) (Figure 2) showed acute interstitial pancreatitis with an enlarged edematous gland and peripancreatic edema. There was also marked intra- and extrahepatic bile duct dilation. A focal filling defect was present in the distal common bile duct. The pancreatic duct joins the common bile duct approximately 3 cm before inserting into the duodenum. The finding was confirmed on endoscopic retrograde cholangiopancreatography (ERCP) (Figure 3). During this procedure, the duct was cleared using a balloon catheter and a biliary stent was placed. Repeat MRCP (Figure 4) continued to show dilated intra- and extrahepatic bile ducts as well as anomalous pancreaticobiliary junction. The finding confirmed a type 4 choledochal cyst.

Diagnosis
Pancreaticobiliary maljunction (PBM) with type 4 choledochal cyst
Discussion
PBM (also known as anomalous pancreaticobiliary junction) is an uncommon congenital anomaly affecting the confluence of the pancreatic duct and the common bile duct. 1 Normally, the 2 ducts join within the duodenal wall. In patients with PBM, the confluence of the ducts is located outside the duodenal wall, forming a long common channel. 2,3 PBM can be classified into 2 groups: with and without biliary dilation. Of the 2 types, biliary dilation occurs more frequently and has its own classification systems based on the site of the dilation that can include cases of congenital biliary dilation not associated with PBM. 2,4 Such cases were formerly known as choledochal cysts and are now defined as local dilation of the extrahepatic bile duct. 2
Patients with PBM and biliary dilation are usually symptomatic and identified during childhood. In these patients, symptoms include abdominal pain, vomiting, jaundice, and fever. Serum bilirubin, amylase, and hepatobiliary enzymes generally increase when the patient becomes symptomatic but are frequently normal during asymptomatic periods. 2,3 Patients with PBM without biliary dilation are typically asymptomatic and diagnosed during adulthood. 5
Diagnosis can be made by ERCP or MRCP. These studies show the union of the pancreatic and common bile ducts outside the duodenal wall. The resultant common channel is typically longer than 1 cm in length. 5-9 The long common channel can lead to reflux of pancreatic fluid into the bile duct causing pancreatitis. During image review, the radiologist should evaluate the common channel to determine if it is stenotic, similar in caliber to the common bile duct, or dilated. Additionally, the radiologist should determine if the common bile duct is dilated. To make a confident diagnosis of a dilated common bile duct, other causes of bile duct dilation (such as obstruction) should be excluded. 7,8 ERCP may be useful as it allows the endoscopist to better measure the length of the channel and sample fluid within the bile duct. An amylase level higher than 8000 UI/L within the bile duct is diagnostic of an anomalous pancreaticobiliary junction. 1
Patients with PBM exhibit an elevated risk of gallbladder carcinoma and cholangiocarcinoma, with rates reaching 22% in those with biliary dilatation and 42% in those without biliary dilatation, according to findings from a comprehensive Japanese nationwide survey. 10 The same survey found that cases with dilation have a higher frequency of bile duct cancer (32% of the cases) compared with cases without dilation, where cancer developed almost exclusively in the gallbladder (88% of the cases). 10 Patients with PBM and biliary system malignancies are diagnosed with cancer 10-15 years earlier than patients without PBM. 2 Therefore, noninvasive imaging investigation is recommended in patients with unexpected findings of gallbladder wall thickening on ultrasonography, which may suggest the presence of PBM. 2,5,7 Pathophysiological evidence suggests that malignant transformation occurs due to the inadequate regulation of the pancreaticobiliary junction by the sphincter of Oddi. This causes 2-way pancreatobiliary and biliopancreatic reflux that leads to epithelial injury, hyperplasia, and metaplasia. 2,4 Bile reflux also results in an elevated risk for other conditions such as acute pancreatitis and gallstone formation, the first being more frequent in children and the latter in adults. 2-5
Prophylactic flow-diversion surgery with resection of the bile duct and the establishment of a bilioenteric anastomosis is the preferred approach for managing patients with PBM with biliary dilation. This surgery is recommended to prevent the onset of biliary malignancy, and there is no clear evidence of when it should be performed. Surgery is usually done soon after the diagnosis. 2 Due to the heightened risk of carcinogenesis post-surgery, internal drainage procedures are commonly employed. Conversely, the optimal treatment for PBM without biliary dilatation remains a matter of debate. Most institutions perform a standalone prophylactic cholecystectomy, as most biliary malignancies that arise in patients without biliary dilatation are gallbladder cancers. 2,5,11
Conclusion
PBM is a rare congenital anomaly occurring when the junction of the pancreatic and biliary ducts occurs outside of the duodenal wall. Patients with this anomaly have a higher risk of acute pancreatitis and biliary tract cancer. Therefore, patients ultimately undergo prophylactic surgery.
References
- Ragot E, Mabrut J, Ouaïssi M. Pancreaticobiliary maljunctions in European patients with bile duct cysts: results of the multicenter study of the French Surgical Association (AFC). World J Surg. 2017;41(2):538-545. doi:10.1007/s00268-016-3684-x.
- Kamisawa T, Kaneko K, Itoi T, Ando H. Pancreaticobiliary maljunction and congenital biliary dilatation. Lancet Gastroenterol Hepatol. 2017;2(8):610-618. doi:10.1016/S2468-1253(17)30002-X.
- Kamisawa T, Takuma K, Anjiki H. Pancreaticobiliary maljunction. Clin Gastroenterol Hepatol. 2009;7(11 suppl):S84-S88. doi:10.1016/j.cgh.2009.08.024.
- Kamisawa T, Egawa N, Nakajima H. Origin of the long common channel based on pancreatographic findings in pancreaticobiliary maljunction. Dig Liver Dis. 2005;37(5):363-367. doi:10.1016/j.dld.2004.11.007.
- Ishibashi H, Shimada M, Kamisawa T. Japanese clinical practice guidelines for congenital biliary dilatation. J Hepatobiliary Pancreat Sci. 2017;24(1):1-16. doi:10.1002/jhbp.415.
- Matos C, Nicaise N, Devière J. Choledochal cysts: comparison of findings at MR cholangiopancreatography and endoscopic retrograde cholangiopancreatography in eight patients. Radiology. 1998;209(2):443-448. doi:10.1148/radiology.209.2.9807571.
- Hamada Y, Ando H, Kamisawa T. Diagnostic criteria for congenital biliary dilatation 2015. J Hepatobiliary Pancreat Sci. 2016;23(6):342-346. doi:10.1002/jhbp.346.
- Fumino S, Ono S, Kimura O, Deguchi E, Iwai N. Diagnostic impact of computed tomography cholangiography and magnetic resonance cholangiopancreatography on pancreaticobiliary maljunction. J Pediatr Surg. 2011;46(7):1373-1378. doi:10.1016/j.jpedsurg.2011.01.026.
- Sugai M, Ishido K, Endoh M, Hada R, Munakata H. Sonographic demonstration of wall thickness of the gallbladder in pediatric patients with pancreatico-biliary maljunction. J Hepatobiliary Pancreat Sci. 2010;17(3):345-348. doi:10.1007/s00534-009-0252-x.
- Morine Y, Shimada M, Takamatsu H. Clinical features of pancreaticobiliary maljunction: update analysis of 2nd Japan-nationwide survey. J Hepatobiliary Pancreat Sci. 2013;20(5):472-480. doi:10.1007/s00534-013-0606-2.
- Matsumoto Y, Fujii H, Itakura J. Recent advances in pancreaticobiliary maljunction. J Hepatobiliary Pancreat Surg. 2002;9(1):45-54. doi:10.1007/s005340200004.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Pancreaticobiliary Maljunction. Applied Radiology. 2025. doi:10.37549/JPCR-25-0069.