Pectus Excavatum
Journal of Pediatric Case Reports — Vol. 1 , Issue 2
Published: April 1, 2026
1 Creighton University School of Medicine, Omaha, Nebraska
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pectus excavatum, commonly known as sunken or funnel chest, is the most common congenital chest wall deformity. It affects approximately 1 in 40 0 to 1 in 100 0 live births,¹ with males being 3-5 times more likely to be affected than females.¹ This structural anomaly can compress the heart and lungs, potentially leading to functional impairment. CT or MRI can both be used to assess pectus excavatum. The evaluation of pectus excavatum primarily utilizes the Haller index (HI) to determine the severity of sternal depression. A mild deformity is considered when HI values are between > 2 and 3. 2, moderate deformity is noted with HI between 3. 2 and 3. 5, and a severe deformity is indicated by an HI of > 3. 5. Patients typically require surgical correction if their HI values exceed 3. 2, while normal values range between 2. 0 and 3. 0. If needed, pectus excavatum is treated surgically. The Nuss procedure is a minimally invasive surgical technique for pectus excavatum repair. This procedure involves the insertion of a curved substernal bar into the chest through 2 lateral thoracic incisions.
Keywords
thorax, sternum, congenital
Categories
Case Summary
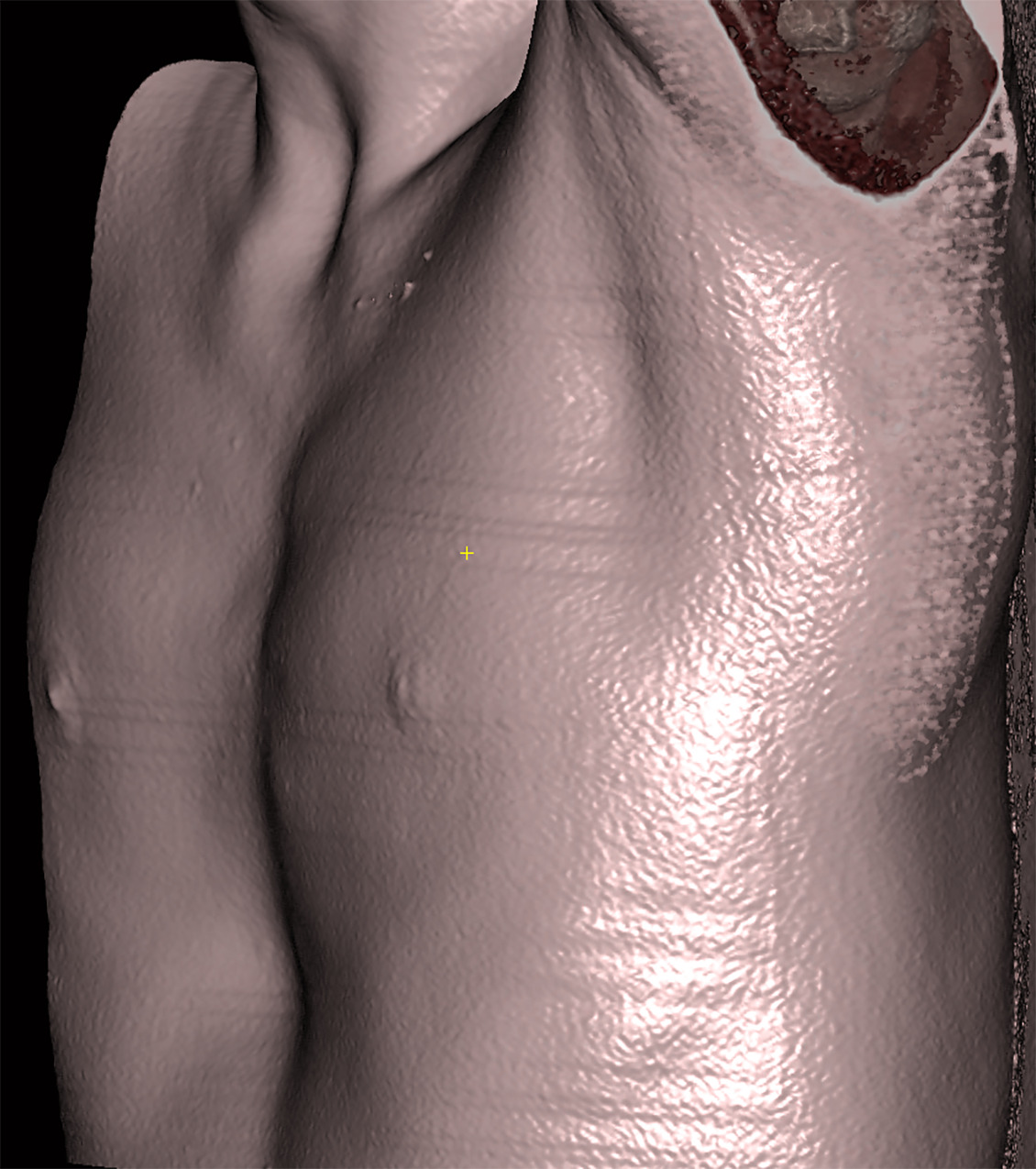
An adolescent male presented to the chest wall deformity clinic with a visible pectus excavatum deformity.
Imaging Findings
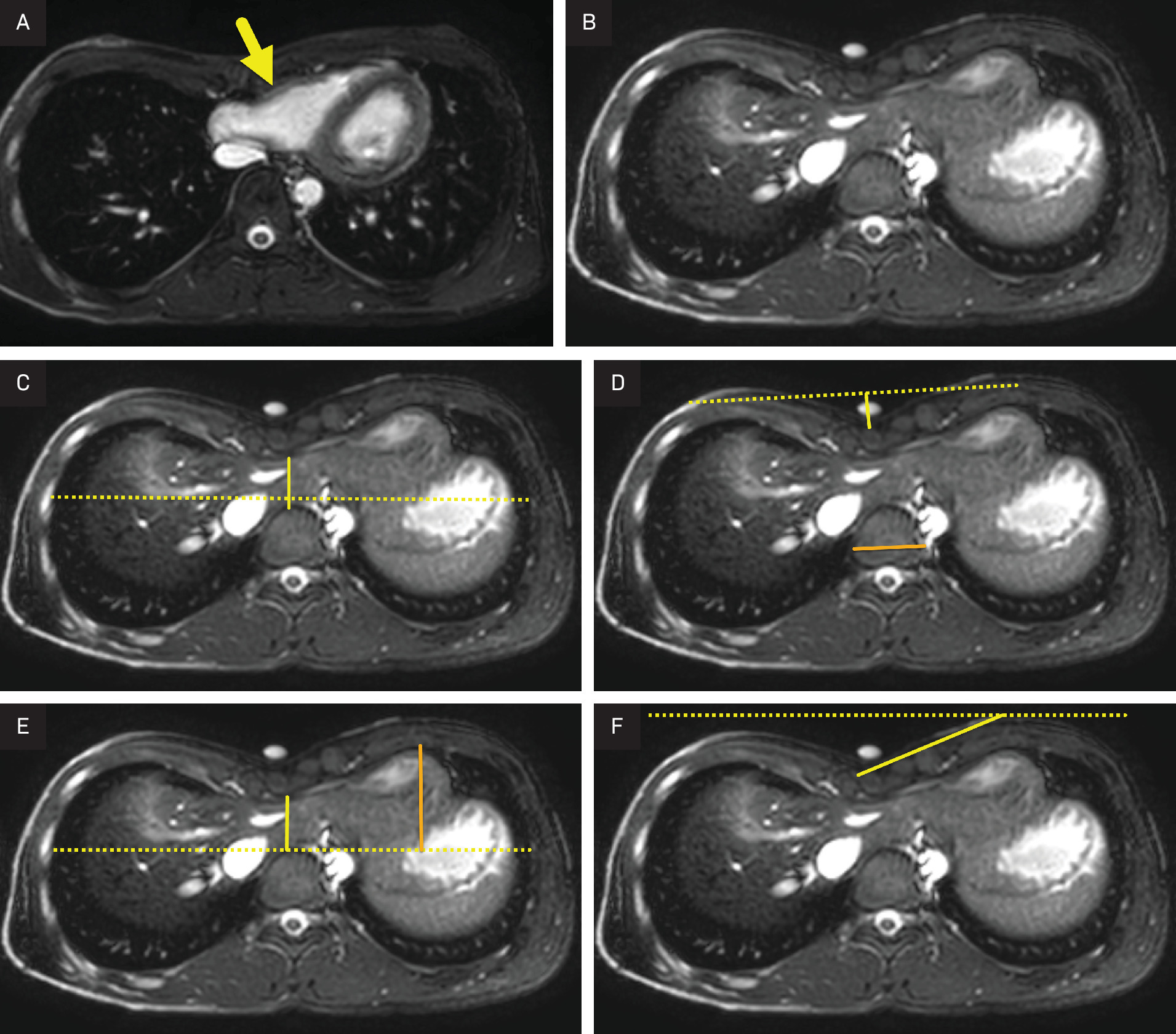
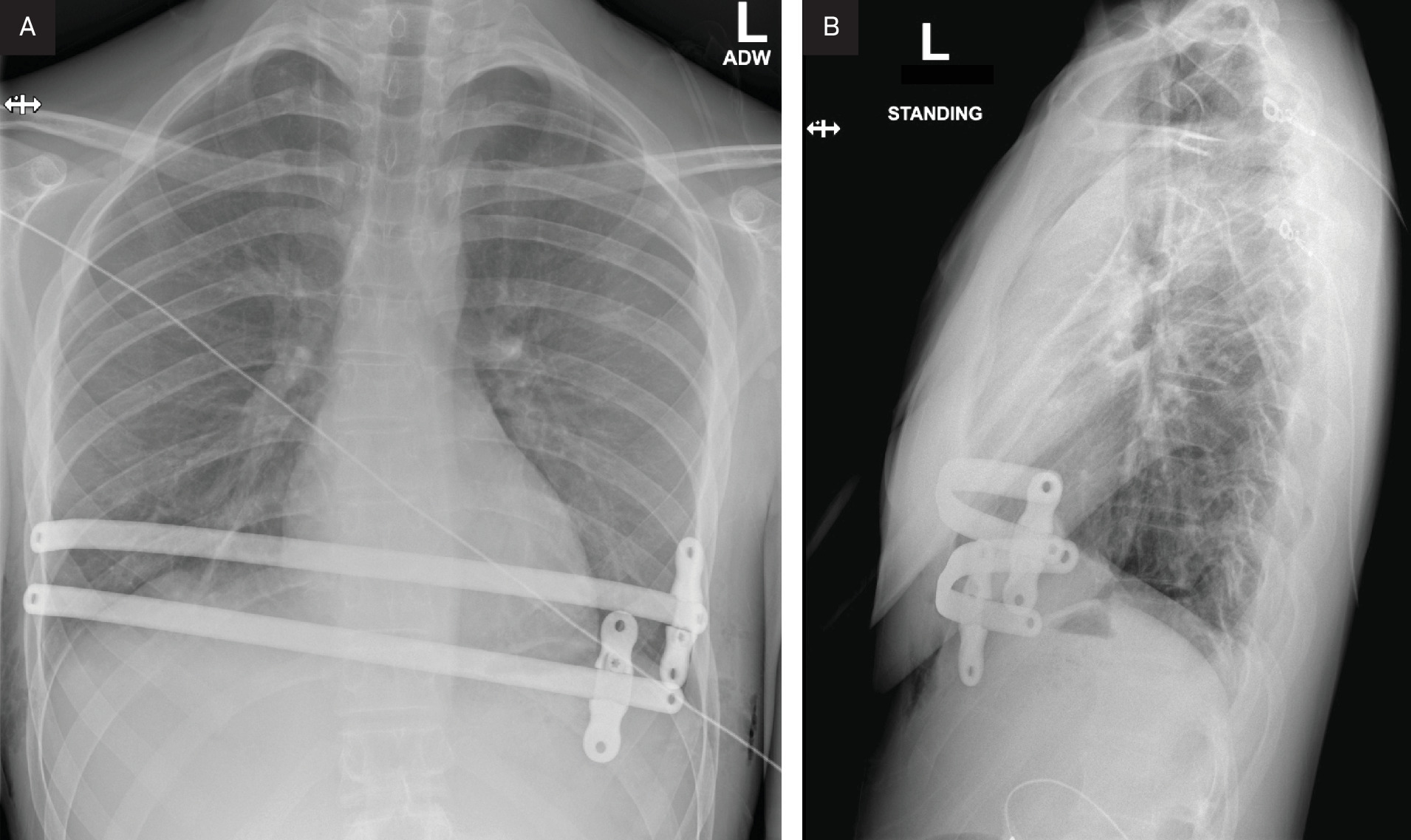
Cardiac MRI ( Figure 1 ) and chest CT ( Figure 2 ) showed a severe pectus excavatum deformity with a Haller index (HI) of 1 0. The chest wall deformity was compressing the heart at the atrioventricular junction. The pectus deformity was treated by placing 2 pectus bars ( Figure 3 ).
Diagnosis
Pectus excavatum
Discussion
Pectus excavatum, commonly known as sunken or funnel chest, is the most common congenital chest wall deformity, accounting for 9 0% of all such deformities in children. It affects approximately 1 in 40 0 to 1 in 100 0 live births, 1 with males being 3-5 times more likely to be affected than females. 1 The deformity primarily results from an excessive growth of connective tissue, causing the sternum to invert. Depending on the rotation pattern of the sternum, pectus excavatum can be symmetrical or asymmetrical. 1 In either pattern, this structural anomaly can compress the heart and lungs, potentially leading to functional impairment.
In addition to its physical manifestations, pectus excavatum is frequently associated with syndromes, further complicating its clinical presentation. Notably, patients with pectus excavatum have a significantly higher propensity for concurrent connective tissue disorders; for instance, they are 16. 7 times more likely to have Marfan syndrome compared with the general population (5 % versus 0. 3%). 2 Beyond Marfan syndrome, this deformity is linked with a variety of other congenital genetic disorders, including Ehlers-Danlos syndrome, Noonan syndrome, neurofibromatosis type 1, Turner syndrome, and autism spectrum disorder. 3
Patients with pectus excavatum commonly report a range of symptoms that significantly impact their daily activities and quality of life. The most frequently reported symptoms include exercise intolerance, chest pain, and shortness of breath. Although exercise intolerance is prevalent, most patients do not exhibit cardiac symptoms at rest. This discrepancy can be attributed to the inhibition of cardiac return and the subsequent decrease in cardiac output during physical activity, which results from the anatomical compression of the chest. 1 Additionally, some patients may experience a persistent cough. 4 Furthermore, the distinctive physical appearance associated with pectus excavatum often affects the morale of adolescent patients, contributing to poor self-esteem and body image issues.
On physical examination, there is an inward displacement of the sternum and surrounding costal cartilages. 1 Sternal depression leads to a reduced sternovertebral distance and causes a leftward displacement of the heart. The cardiac displacement is often observable on an EKG as an axis deviation. 1 Pulmonary function tests may reveal decreased forced vital capacity , forced expiratory volume in one second, and the average forced expiratory flow rate between 2 5% and 75 % of the vital capacity. 5
CT or MRI can both be used to assess pectus excavatum. If CT is used, imaging can be focused to reduce radiation. If this strategy is used, the deepest portion of the sternal depression is identified using a B b. This location is then used as the center p oint for imaging. The technologist can then expand the field of view 5 cm above and below the BB. If MR is performed, the whole chest can be imaged. The benefits of MRI include the lack of radiation and the ability to simultaneously assess cardiac function and the chest wall deformity, thus avoiding echocardiogram. 6
The evaluation of pectus excavatum primarily utilizes the HI to determine the severity of sternal depression. The HI is calculated by measuring the maximal internal transverse diameter of the chest from rib margin to rib margin, divided by the minimal anteroposterior depth of the chest from the vertebral body to the sternum at the same level. A mild deformity is considered when HI values are between > 2 and 3. 2, moderate deformity is noted with HI between 3. 2 and 3. 5, and a severe deformity is indicated by an HI of > 3. 5. Patients typically require surgical correction if their HI values exceed 3. 2, while normal values range between 2. 0 and 3.0. 7
In addition to the HI , several other measures are used to describe the chest wall deformity. These indices guide surgical planning and provide supportive evidence to ensure that surgery is needed.
Correction i ndex ( CI ): This measure evaluates the degree of sternal depression relative to the anterior chest wall. It is calculated by drawing a line (line a) from the posterior aspect of the sternum at its deepest point to a horizontal line drawn along the anterior aspect of the vertebral body. A second line (line b) is then drawn on the same image from the most anterior portion of the inner chest wall to the same horizontal line. The CI is then calculated as a percentage using the formula: (Length of line b − Length of line a)/Length of line b) × 100 %. A CI greater than 1 0% is considered abnormal, indicating significant deformity that may benefit from surgical intervention.
Depression i ndex ( DI ): The DI uses the vertebral body diameter as a baseline to assess the severity of the chest depression relative to an individual’s size. It is calculated by identifying the deepest site of sternal depression. A line is then drawn connecting the anterior aspect of the ribs. A second line (depth) is drawn from the first line to the deepest portion of the anterior sternum. Finally, a third line is drawn measuring the width of the vertebral body on the same image. The DI is then calculated as the depth/width. A DI greater than 0. 2 is abnormal, suggesting a notable inward depression of the sternum.
Sternal t orsion a ngle ( STA ): The STA measures the angular deviation of the sternum, providing a quantitative assessment of the torsional deformation of the chest wall. This measure is particularly useful in surgical planning and assessing the asymmetry of the chest wall deformity. It is measured by determining the angle between a true horizontal line outside the patient and a line along the anterior aspect of the sternum. By convention, a right side-down sternal tilt is reported using negative numbers and described as counterclockwise, while a left-side down tilt is reported using positive numbers and described as clockwise.
If needed, pectus excavatum is treated surgically. The Nuss procedure is a minimally invasive surgical technique for pectus excavatum repair. This procedure involves the insertion of a curved substernal bar into the chest through 2 lateral thoracic incisions. The bar is carefully guided through the mediastinum using thoracoscopy and is typically removed after 2 -4 years. 8 One of the major advantages of this approach is that it avoids the need for costal cartilage resection or sternal osteotomy, thereby reducing recovery time and postoperative complications. 9
Eligibility for the Nuss procedure requires meeting at least 2 of the following 6 criteria:
Symptomatic manifestation of the deformity
Severe pectus excavatum deformity observable on physical examination
An HI >3. 2
Pulmonary function tests showing restrictive or obstructive patterns
Evidence of cardiac compression or displacement
Significant impact on the patient’s body image and self-esteem 8
These criteria ensure that the procedure is reserved for patients who will most likely benefit from surgical intervention, taking into consideration both physical health impacts and psychological well-being.
A 2016 review demonstrated highly favorable outcomes for the Nuss procedure, with 9 8% of patients achieving excellent results, characterized by normal chest anatomy and minimal residual sternal depression. 8 Post-surgery, patients commonly experience significant improvements in cardiovascular function, including increased stroke volume and cardiac output, as well as gradual enhancements in pulmonary function following the removal of the substernal bar. 8
Despite the high success rate, certain complications have been noted. Initially, bar displacements requiring surgical revision were reported at a rate of 3. 7% and overcorrections occurred in approximately 3. 1% of cases. To address these issues, refinements such as the incorporation of stabilizers and subcostal sutures have been implemented, substantially reducing the rate of bar displacement to 1 %. 8 These adjustments have improved the procedure’s safety and efficacy, further solidifying its role as a critical intervention for severe pectus excavatum.
Pectus excavatum, the most common congenital chest wall deformity, affects both physical health and psychological well-being. 10 It is characterized by inward displacement of the sternum, which, in severe cases, can compress the heart and lungs, leading to functional impairments. The condition is associated with various syndromes and can impact a patient’s quality of life due to symptoms such as exercise intolerance and poor body image. Diagnosis relies on imaging techniques such as CT and MRI, along with objective indices, including the HI, CI, DI, and STA, all of which help assess severity and guide surgical decision-making. When treatment is necessary, the Nuss procedure is the preferred corrective approach, improving both anatomical and functional outcomes. Despite potential complications, ongoing refinements in surgical techniques continue to enhance the procedure’s safety and effectiveness.
Conclusion
Pectus excavatum, commonly known as sunken or funnel chest, is the most common congenital chest wall deformity. It affects approximately 1 in 40 0 to 1 in 100 0 live births, 1 with males being 3-5 times more likely to be affected than females. 1 This structural anomaly can compress the heart and lungs , potentially leading to functional impairment.
CT or MRI can both be used to assess pectus excavatum. The evaluation of pectus excavatum primarily utilizes the HI to determine the severity of sternal depression. A mild deformity is considered when HI values are between > 2 and 3. 2, moderate deformity is noted with HI between 3. 2 and 3. 5, and a severe deformity is indicated by an HI of > 3. 5. Patients typically require surgical correction if their HI values exceed 3. 2, while normal values range between 2. 0 and 3. 0. If needed, pectus excavatum is treated surgically. The Nuss procedure is a minimally invasive surgical technique for pectus excavatum repair. This procedure involves the insertion of a curved substernal bar into the chest through 2 lateral thoracic incisions.
References
- Fokin A, Steuerwald N, Ahrens W, Allen K. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg. 2009;21(1):44-57. doi:10.1053/j.semtcvs.2009.03.001.
- Behr C, Denning N, Kallis M. The incidence of Marfan syndrome and cardiac anomalies in patients presenting with pectus deformities. J Pediatr Surg. 2019;54(9):1926-1928. doi:10.1016/j.jpedsurg.2018.11.017.
- Billar R, Manoubi W, Kant S. Association between pectus excavatum and congenital genetic disorders: a systematic review and practical guide for the treating physician. J Pediatr Surg. 2021;56(12):2239-2252. doi:10.1016/j.jpedsurg.2021.04.0164.
- Donato B, Linnaus M, Velazco C. Severe pectus excavatum with tracheal compression presenting with chronic cough. J Pediatr Surg Case Rep. 2018;33:14-16. doi:10.1016/j.epsc.2018.03.004.
- Kelly R, Obermeyer R, Nuss D. Diminished pulmonary function in pectus excavatum: from denying the problem to finding the mechanism. Ann Cardiothorac Surg. 2016;5(5):466-475. doi:10.21037/acs.2016.09.09.
- Birkemeier K, Podberesky D, Salisbury S, Serai S. Limited, fast magnetic resonance imaging as an alternative for preoperative evaluation of pectus excavatum: a feasibility study. J Thorac Imaging. 2012;27(6):393-397. doi:10.1097/RTI.0b013e31822da1b6.
- Daunt S, Cohen J, Miller S. Age-related normal ranges for the haller index in children. Pediatr Radiol. 2004;34(4):326-330. doi:10.1007/s00247-003-1116-1.
- Nuss D, Obermeyer R, Kelly R. Nuss bar procedure: past, present and future. Ann Cardiothorac Surg. 2016;5(5):422-433. doi:10.21037/acs.2016.08.05.
- Nuss D, Kelly R. Minimally invasive surgical correction of chest wall deformities in children (Nuss procedure). Adv Pediatr. 2008;55:395-410. doi:10.1016/j.yapd.2008.07.012.
- Zuidema W, Oosterhuis J, Zijp G. Early consequences of pectus excavatum surgery on self-esteem and general quality of life. World J Surg. 2018;42(8):2502-2506. doi:10.1007/s00268-018-4526-9.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Pectus Excavatum. Journal of Pediatric Case Reports. 2026;1(2). doi:10.37549/JPCR-26-0086.