Pleural Effusion and the Approach to Therapy: Simple Versus Complex Effusions
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -3
Published: November 1, 2025
1 Creighton University School of Medicine, Phoenix Regional Campus, Phoenix, Arizona
2 Phoenix Children’s Hospital, Phoenix, Arizona
3 Cincinnati Children’s Hospital and Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Treatment of a parapneumonic pleural effusion is largely dictated by effusion size and disease progression. Small and moderate effusions in stage 1 may be treated with antibiotics alone and supplemental thoracentesis if the patient develops respiratory distress. Large effusions may be addressed with chest tube insertion with or without fibrinolytics and/or video-assisted thoracoscopic surgery (VATS). Choosing between these 2 interventions depends on the disease progression. Currently, further investigation is required to identify when the cutoff occurs for intervening with chest tube drainage or VATS.
Keywords
pleural effusion therapy, thorax
Categories
Case Summary
A toddler presented with a short history of an upper respiratory infection with fever that progressed to respiratory distress. A second child, an infant, presented with a 1-week history of cough, congestion, and rhinorrhea, plus 1 day of fever. Diagnosed a few weeks prior with acute otitis media and upper respiratory infection, for which a 7-day course of antibiotics was completed. A 2-view chest radiograph and chest US were performed.
Imaging Findings
Two patients are presented.
History of Patient #1
A toddler with trisomy 21 and prior repair of an AV canal defect presented with a 3-day history of upper respiratory infection symptoms and fever. The toddler was diagnosed with pneumonia, which progressed to acute respiratory distress syndrome. A chest US was performed after bilateral pleural effusions were visualized on a chest radiograph.
History of Patient #2
An infant presented with a 1-week history of cough, congestion, and rhinorrhea, and 1 day of fever. The infant was diagnosed a few weeks prior with acute otitis media and upper respiratory infection, for which a 7-day course of antibiotics was completed. A 2-view chest radiograph and chest US were performed.
Diagnosis
Pleural effusion, simple and complex.
Differential diagnosis for pleural effusion includes transudative and exudative processes. Transudative causes stem from changes in capillary hydrostatic and/or oncotic pressure, driven by etiologies such as congestive heart failure and nephrotic syndrome. Exudative effusions may result from inflammatory processes such as infection (mainly pneumonia), malignancy (pulmonary or metastatic origin), and pulmonary embolism. Chylothorax and hemothorax may also be included in the differential diagnosis, although these are less common.
Discussion
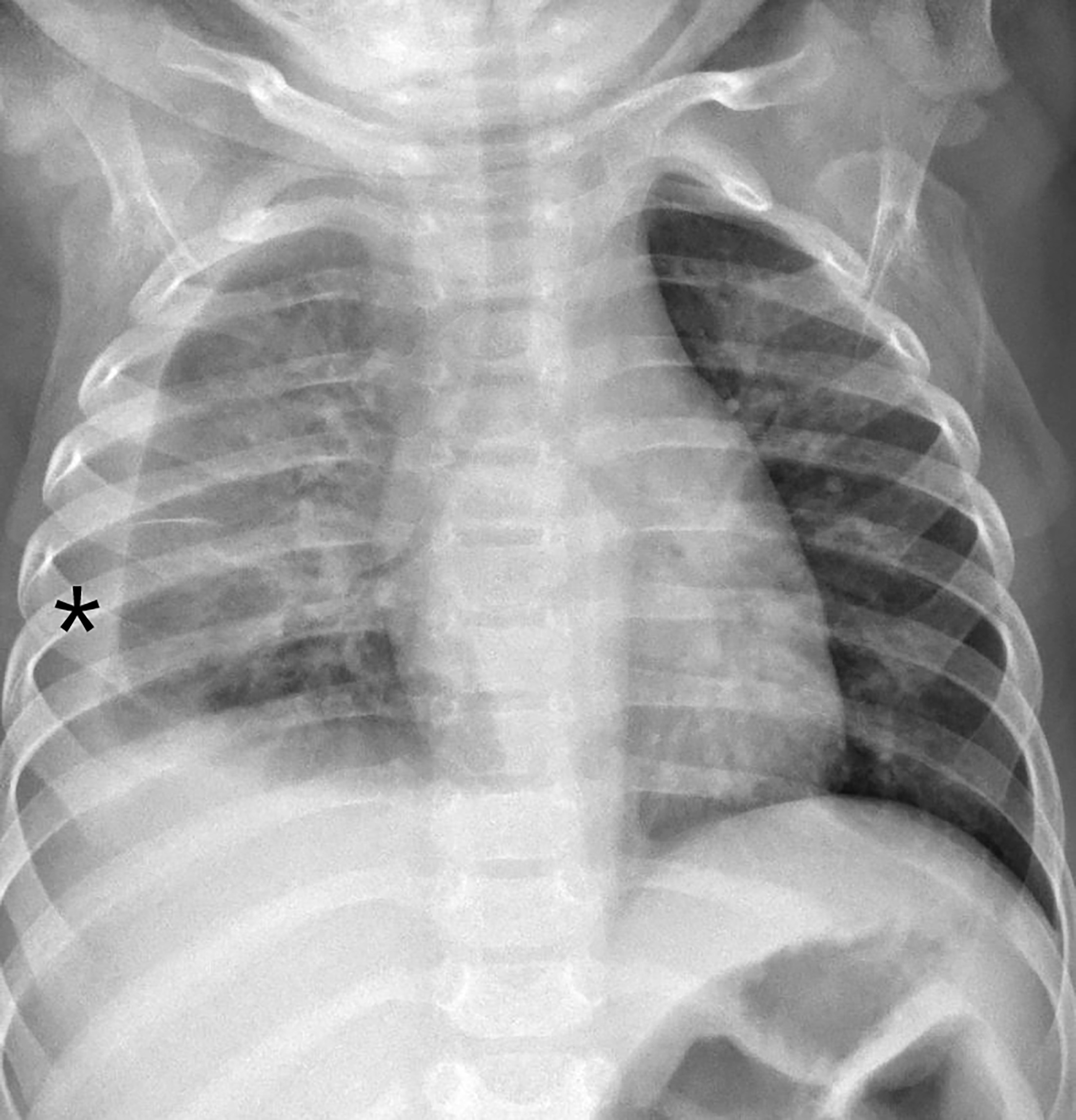
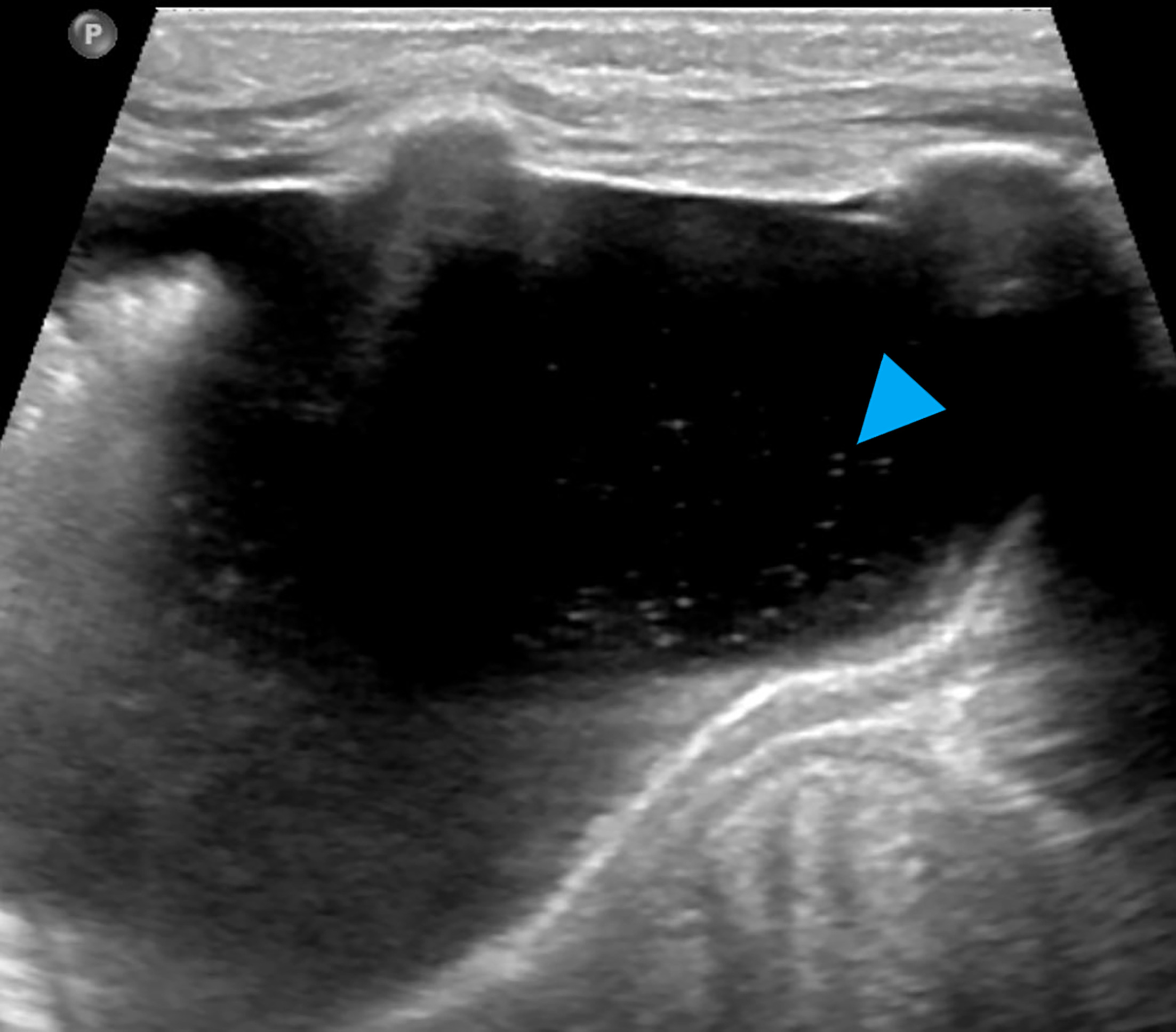
The primary imaging for the detection of a parapneumonic pleural effusion is frontal and lateral chest radiography (Figure 1). When an effusion is present, if large enough, there will be thoracic opacification with associated peripheral lung compression, possible displacement of the lung, and blunting of the costophrenic angle. Once an effusion is detected, chest US can be used to ascertain further characteristics, including effusion size, quality of the fluid (simple or complex), and/or the presence of septations and loculations. Simple effusions will appear anechoic or hypoechoic with unrestricted flow of pleural fluid. In contrast, complex effusions will appear echogenic (dirty) with septations of variable thickness, limiting the motion of pleural fluid.
Pleural effusion is the filling of the pleural space with fluid. This process can either be transudative or exudative. In transudative effusions, an increase in capillary hydrostatic pressure or decrease in capillary oncotic pressure leads to the movement of plasma into the pleural space (third spacing). In exudative effusions, an inflammatory response leads to increased permeability of capillary endothelium, increasing the outflow of plasma in addition to immune cells, pathogens, and proteins. As a result, effusion contents differ between a transudate and an exudate. For an effusion to be considered exudative, at least 1 of 3 Light’s criteria must be met: (1) pleural fluid protein to serum protein ratio is >0.5, or (2) pleural fluid lactate dehydrogenase (LDH) to serum LDH ratio is >0.6, or (3) pleural fluid LDH is >2/3 the upper limit of normal. In children, the most common causes of pleural effusion are infection, heart failure, and malignancy. Uncommon causes include collagen vascular diseases, gastrointestinal conditions, kidney diseases, and lymphatic abnormalities. In the pediatric population, 2-12% of patients with bacterial pneumonia have an associated pleural effusion. 1,2
Parapneumonic pleural effusions are further characterized by 3 stages. In stage 1, sterile exudate leaks into the space, flows freely, and typically lasts for less than 72 hours. This is known as the exudative stage, or a simple effusion. During stage 2, leukocyte and bacterial infiltration begins while fibrin is deposited throughout the pleural space, obstructing the free flow of exudate. This occurs anywhere from 72 hours to 2 weeks after infection and is known as the fibrinopurulent stage. The presence of septations now classifies the effusion as a complicated or complex effusion. Additionally, the septations can lead to pockets of thick, purulent fluid known as an empyema. Stage 3 of the disease process is the organizational stage, in which further fibrin deposition via fibroblast proliferation leads to the development of loculations and abscesses. This stage typically occurs 2 weeks after the onset of infection and results in the formation of an adhesive pleural peel. 1-4
Early detection and treatment of pneumonia reduce the risk of complications like parapneumonic effusion. Diagnosis is largely based on clinical presentation, in which the most common pediatric symptoms include cough, fever, anorexia, and dyspnea. 4 From there, chest radiography is used to assess the thoracic cavity. If an effusion is detected, chest US is then used to characterize the fluid within the pleural space and guide minimally invasive procedures if necessary. US is particularly suitable for the pediatric population, given that it is mobile and can be brought to bedside, does not expose the patient to ionizing radiation, is cost-effective, widely available, and easily accessible. 5 In simple effusions, the fluid will appear anechoic or hypoechoic, and it will move freely within the pleural space during respiration (Figure 2). In contrast, exudate will appear echoic, may show restricted motions with positioning and respirations, and internal septations will be detectable in complicated effusions (Figure 3). 6

Although it is used less frequently, contrast-enhanced US (CEUS) also provides supplemental information in those with complicated effusions. First, intravenous CEUS identifies necrosis within lung consolidations, which appear as nonenhancing lesions. Additionally, it highlights areas of parapneumonic effusion that appear initially as consolidation on grayscale US, which directs antibiotic treatment to include catheter drainage with fibrinolytics. 7 At this time, it is unclear if CEUS impacts decision-making and outcomes regarding the treatment of children with complex pleural effusions. Double-blind studies are necessary to determine the utility of CEUS for this indication.
There are 3 procedures that may be utilized in the treatment of a pleural effusion. 8 The first 2 interventions—thoracentesis and chest tube insertion—are minimally invasive and usually sufficient to treat stage 1 and 2 effusions. These may be performed at the bedside or in the interventional radiology suite under US guidance and with or without anesthesia, depending on the cooperativity and overall health of the patient. In addition to draining an effusion, chest tube insertion allows for the delivery of fibrinolytic agents, which is useful if the fluid collection is in the early phase of stage 2. Finally, video-assisted thoracoscopic surgery (VATS) is an invasive procedure that is generally reserved for stage 3 collections or collections unsuccessfully treated with catheter drainage and fibrinolytics. Unlike thoracentesis and chest tube insertion, VATS is performed in an operating room under anesthesia.
The size of the fluid collection is the first feature to consider when treating a pleural effusion. In small effusions (<10 mm or <25% thoracic opacification), antibiotic treatment alone may be sufficient. If the fluid collection is moderate (>10 mm and 25-50% thoracic opacification), respiratory compromise becomes an additional factor. If the patient is asymptomatic, antibiotics alone may still suffice, with thoracentesis serving as an appropriate supplement if the patient becomes symptomatic or fluid culture is needed. However, if the patient progresses to significant respiratory distress, the effusion should be treated as a large collection (>10 mm and > 50% opacification). In this case, chest tube drainage with or without fibrinolytics and VATS are appropriate interventions. 8
While chest tube drainage clearly has its benefits, a recent meta-analysis on surgical intervention for pediatric empyema found that VATS offered a reduced hospital length of stay and reintervention rate compared with chest tube drainage (9.6% versus 22.5%). Additionally, there was no statistically significant difference in perioperative complication rates (4.7% for VATS vs 8.0% for chest tube insertion). Pneumothorax was the primary complication for VATS, while the main untoward effect of chest tube insertion was localized pain from the chest tube and upon administration of the fibrinolytic. 9 A potential area of further study is the identification of a predictable window during stage 2 where chest tube insertion with fibrinolytics is still viable.
Conclusion
Treatment of a parapneumonic pleural effusion is largely dictated by effusion size and disease progression. Small and moderate effusions in stage 1 may be treated with antibiotics alone and supplemental thoracentesis if the patient develops respiratory distress. Large effusions may be addressed with chest tube insertion with or without fibrinolytics and/or VATS. Choosing between these 2 interventions depends on the disease progression. Currently, further investigation is required to identify when the cutoff occurs for intervening with chest tube drainage or VATS.
References
- Towbin R, Baskin K, Aria D, Schaefer C, Towbin R, Baskin K. Pediatric Interventional Radiology. 2015:98-108.
- Cashen K, Petersen T. Pleural effusions and pneumothoraces. Pediatr Rev. 2017;38(4):170-181. doi:10.1542/pir.2016-0088.
- Kunisaki S, Leys C. Surgical pulmonary and pleural diseases in children: lung malformations, empyema, and spontaneous pneumothorax. Adv Pediatr. 2020;67:145-169. doi:10.1016/j.yapd.2020.03.006.
- Calder A, Owens C. Imaging of parapneumonic pleural effusions and empyema in children. Pediatr Radiol. 2009;39(6):527-537. doi:10.1007/s00247-008-1133-1.
- Rea D, Temple M, Marshalleck F. Pediatric Interventional Radiology. 2014. doi:10.1007/978-1-4419-5856-3_19.
- Goh Y, Kapur J. Sonography of the pediatric chest. J Ultrasound Med. 2016;35(5):1067-1080. doi:10.7863/ultra.15.06006.
- Rafailidis V, Andronikou S, Mentzel H. Contrast-enhanced ultrasound of pediatric lungs. Pediatr Radiol. 2021;51(12):2340-2350. doi:10.1007/s00247-020-04914-8.
- Feola G, Hogan M, Baskin K. Quality improvement standards for the treatment of pediatric empyema. Journal of Vascular and Interventional Radiology. 2018;29(10):1415-1422. doi:10.1016/j.jvir.2018.04.027.
- Pacilli M, Nataraja R. Management of paediatric empyema by video-assisted thoracoscopic surgery (VATS) versus chest drain with fibrinolysis: systematic review and meta-analysis. Paediatr Respir Rev. 2019;30:42-48. doi:10.1016/j.prrv.2018.09.001.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Pleural Effusion and the Approach to Therapy: Simple Versus Complex Effusions. Applied Radiology. 2025;1(1):1-3. doi:10.37549/JPCR-25-0025.