Pulmonary Agenesis
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 1, 2026
1 Midwestern University Arizona College of Osteopathic Medicine, Glendale Arizona, Glendale, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pulmonary agenesis is a rare developmental malformation that presents with nonspecific respiratory symptoms, a small hemithorax, and unilateral absence of breath sounds. Diagnosis is based on clinical suspicion and imaging findings. Radiological workup is essential for diagnosis and helps to distinguish pulmonary agenesis from other developmental malformations, such as pulmonary atresia and aplasia, and acquired conditions, such as foreign bodies and pneumonia.
Keywords
thorax, airway, congenital
Categories
Case Summary
A twin female toddler born at 32 weeks of gestation presented with tachypnea on exertion. The toddler’s medical history includes a vascular ring, gastrostomy tube dependence, and agenesis of the left lung and pulmonary veins.
Imaging Findings
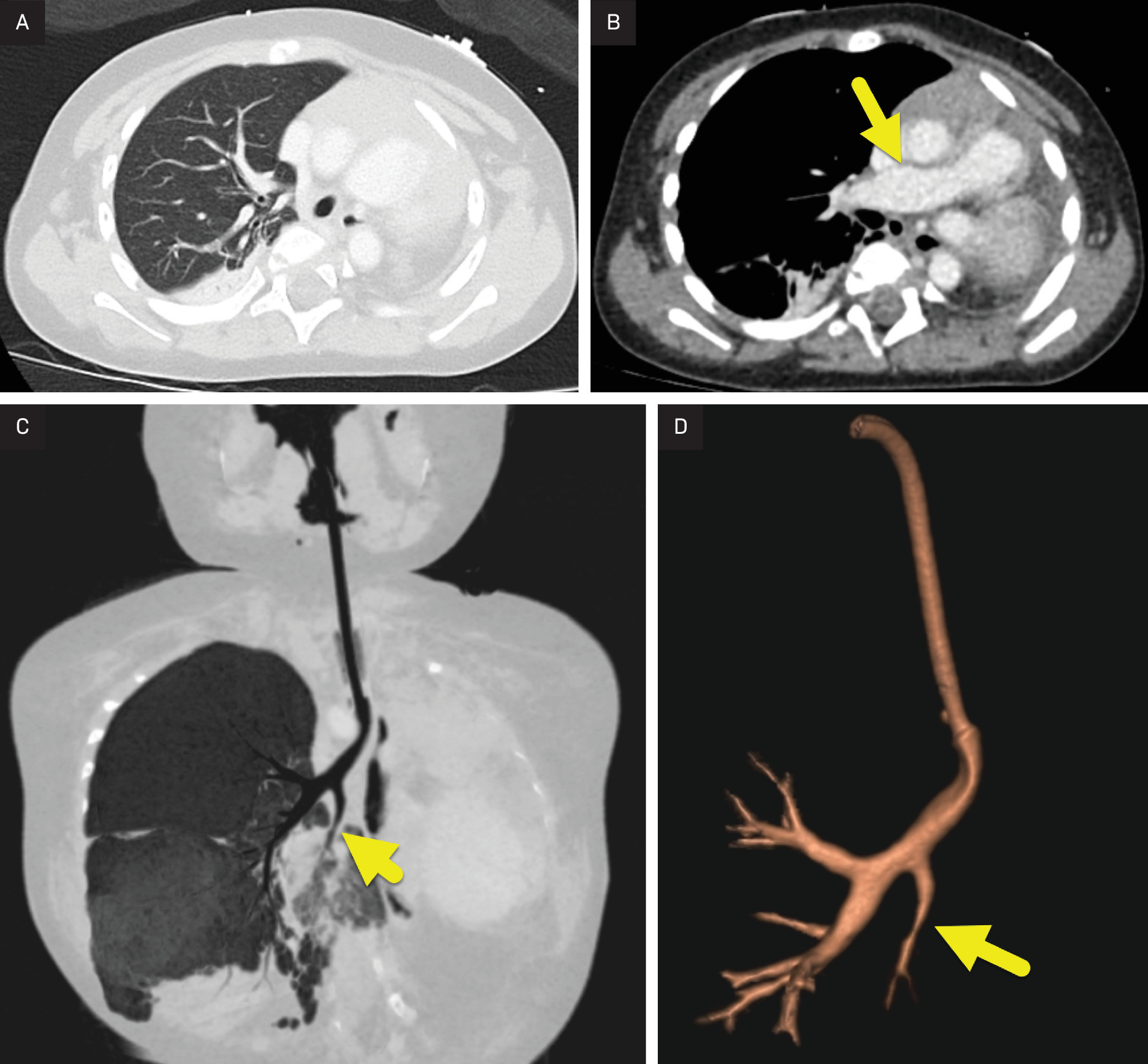
Chest radiograph (Figure 1) demonstrated a hyperinflated right lung with a mediastinal shift toward an opaque and small left hemithorax. There was no visible aeration of the left tracheobronchial tree. Contrast-enhanced CT (CECT) (Figure 2) displayed leftward mediastinal shift, with the absence of the left lung and pulmonary vasculature. Bronchoscopy confirmed absence of the left mainstem bronchus.

Diagnosis
Pulmonary agenesis.
The differential diagnosis for tachypnea on exertion includes respiratory pathology such as bronchopulmonary dysplasia, asthma, and pneumonia. Nonrespiratory causes include developmental heart defects and metabolic disturbance. The differential diagnosis for radiographic imaging demonstrating an opaque hemithorax with contralateral lung hyperinflation includes pulmonary agenesis, pulmonary aplasia, atelectasis, and pneumonectomy.
Discussion
Pulmonary agenesis (PA) is a developmental malformation with absence of one or both lungs, bronchi, pulmonary parenchyma, and vasculature.1 This developmental anomaly should not be confused with pulmonary atresia, a heart valve defect resulting in an absent pulmonary valve. While bilateral pulmonary agenesis may occur, it is not compatible with life. Patients with unilateral agenesis have a variable prognosis, with 50% dying within the first 5 years of life and others having a normal lifespan with minimal symptoms.2-5 Mortality rates in patients with unilateral pulmonary agenesis vary based on the presence of recurrent infections, associated malformations, and the side of agenesis. Right-sided pulmonary agenesis has a higher risk of mortality due to more pronounced mediastinal shift and resultant tracheal compression.2
Pulmonary agenesis is rare, occurring in 1 in 10,000-15,000 births.3 Unilateral pulmonary agenesis occurs on the right and left sides with equal frequency. It may occur in isolation or as part of a group of related developmental malformations, with the latter portending a worse prognosis.6 If not diagnosed in utero, patients may present with nonspecific symptoms. An ultimate diagnosis is made with chest imaging. Radiological workup begins with a chest radiograph, which shows a hyperinflated contralateral lung and a small hemithorax with ipsilateral mediastinal shift.4 Transthoracic echocardiogram with Doppler may also be utilized to evaluate for agenesis of pulmonary vasculature on the affected side.
Diagnosis is confirmed with CECT displaying a single mainstem bronchus, unilateral absence of lung parenchyma, compensatory hyperinflated contralateral lung, and a single-branch pulmonary artery. CT can also highlight tracheobronchial branching abnormality.4 Intravenous contrast can demonstrate associated vascular abnormalities such as pulmonary artery hypoplasia, right aortic arch, anomalous venous return, septal defects, and Tetralogy of Fallot.
Of note, CECT may also help distinguish unilateral pulmonary agenesis from the similar, yet distinct unilateral pulmonary aplasia. While both malformations involve the absence of pulmonary parenchyma and vasculature, pulmonary aplasia maintains 2 mainstem bronchi, one of which ends in a blind-ended pouch. This is due to developmental arrest occurring at a later stage in fetal lung development after the formation of the mainstem bronchi.
Although bronchoscopy is not necessary for confirming the diagnosis of pulmonary agenesis, it may be used instead of imaging if the differential diagnosis includes other causes of unilateral absence of breath sounds.7, 8 If bronchoscopy is performed, the absence of a mainstem bronchus on the affected side confirms the diagnosis of unilateral pulmonary agenesis.
Respiratory insufficiency may occur in patients with unilateral pulmonary agenesis due to recurrent respiratory infections, tracheal compression, and pulmonary hypertension.2,4 Because infection is a significant source of morbidity, patients may be treated with prophylactic antibiotics. Additionally, because mediastinal shift may lead to tracheal kinking and compression, tracheal stenting or tracheoplasty may be performed to improve aeration of the lung.9
The outcome of children with PA is variable and is associated with associated anomalies and the degree of respiratory failure. In general, over 50% of infants die by age 5 years, with about a third passing in the first year. In contrast, children with no associated malformations often live into adulthood.
Conclusion
Pulmonary agenesis is a rare developmental malformation that presents with nonspecific respiratory symptoms, a small hemithorax, and unilateral absence of breath sounds. Diagnosis is based on clinical suspicion and imaging findings. Radiological workup is essential for diagnosis and helps to distinguish pulmonary agenesis from other developmental malformations, such as pulmonary atresia and aplasia, and acquired conditions, such as foreign bodies and pneumonia.
References
- Fukuoka S, Yamamura K, Nagata H. Clinical outcomes of pulmonary agenesis: a systematic review of the literature. Pediatr Pulmonol. 2022;57(12):3060-3068. doi:10.1002/ppul.26135.
- Jentzsch N. Unilateral pulmonary agenesis. J Bras Pneumol. 2014;40(3):322-324. doi:10.1590/s1806-37132014000300017.
- Kumar B, Kandpal D, Sharma C, Sinha D. Right lung agenesis. Afr J Paediatr Surg. 2008;5(2):102-104. doi:10.4103/0189-6725.44189.
- Chassagnon G, Morel B, Carpentier E, Ducou Le Pointe H, Sirinelli D. Tracheobronchial branching abnormalities: lobe-based classification scheme. Radiographics. 2016;36(2):358-373. doi:10.1148/rg.2016150115.
- Dinamarco P, Ponce C. Pulmonary agenesis and respiratory failure in childhood. Autops Case Rep. 2015;5(1):29-32. doi:10.4322/acr.2014.046.
- Malcon M, Malcon C, Cavada M, Caruso P, Real L. Unilateral pulmonary agenesis. J Bras Pneumol. 2012;38(4):526-529. doi:10.1590/s1806-37132012000400016.
- Alwan A, Y, Mohammoud S M, Assefa AZ Y. Incidental pulmonary agenesis with multiple associated anomalies: A case report.. Radiol Case Rep.. 2023;18(10):3724-3728. doi:10.1016/j.radcr.2023.08.002..
- Shrikhande D, Singh G, Kunal A, Niranjan B, Kumar C. Unilateral pulmonary agenesis-a rare cause of respiratory distress in infancy. Med J Armed Forces India. 2012;68(2):176-178. doi:10.1016/S0377-1237(12)60026-4.
- Khurram M, Rao S, Vamshipriya A. Pulmonary agenesis: a case report with review of literature. Qatar Med J. 2013;2013(2):38-40. doi:10.5339/qmj.2013.14.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Pulmonary Agenesis. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0079.