Segond Fracture with an Anterior Cruciate Ligament Tear
Applied Radiology
Published: November 1, 2025
1 School of Osteopathic Medicine, Rowan University, Glassboro, New Jersey
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Children’s Mercy Hospital, Kansas City, Missouri
4 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
The “lateral capsular sign,” an elliptical-shaped skeletal fragment along the outside edge of the tibial plateau, is a characteristic of a Segond fracture usually associated with an anterior cruciate ligament (ACL) tear. Although this sign can be seen on conventional radiographs, MRI offers a more thorough evaluation of knee joint structures and verifies ACL involvement. Imaging should be used to explore for other potential injuries and diagnoses, such as the arcuate sign indicating fibular head avulsion. The best therapeutic approach requires a prompt and precise diagnosis. Surgery to correct the avulsion and ACL reconstruction are frequently used in the management of Segond fractures with ACL tears. With surgical intervention, there is a favorable prognosis.
Keywords
musculoskeletal trauma, knee, sports injury
Categories
Case Summary
A teenager presented to the orthopedic service after sustaining a knee injury playing competitive soccer. He felt a “pop” after planting his foot and trying to cut in a different direction during a play. Significant pain and swelling developed rapidly, prompting him to seek specialty care.
Imaging Findings
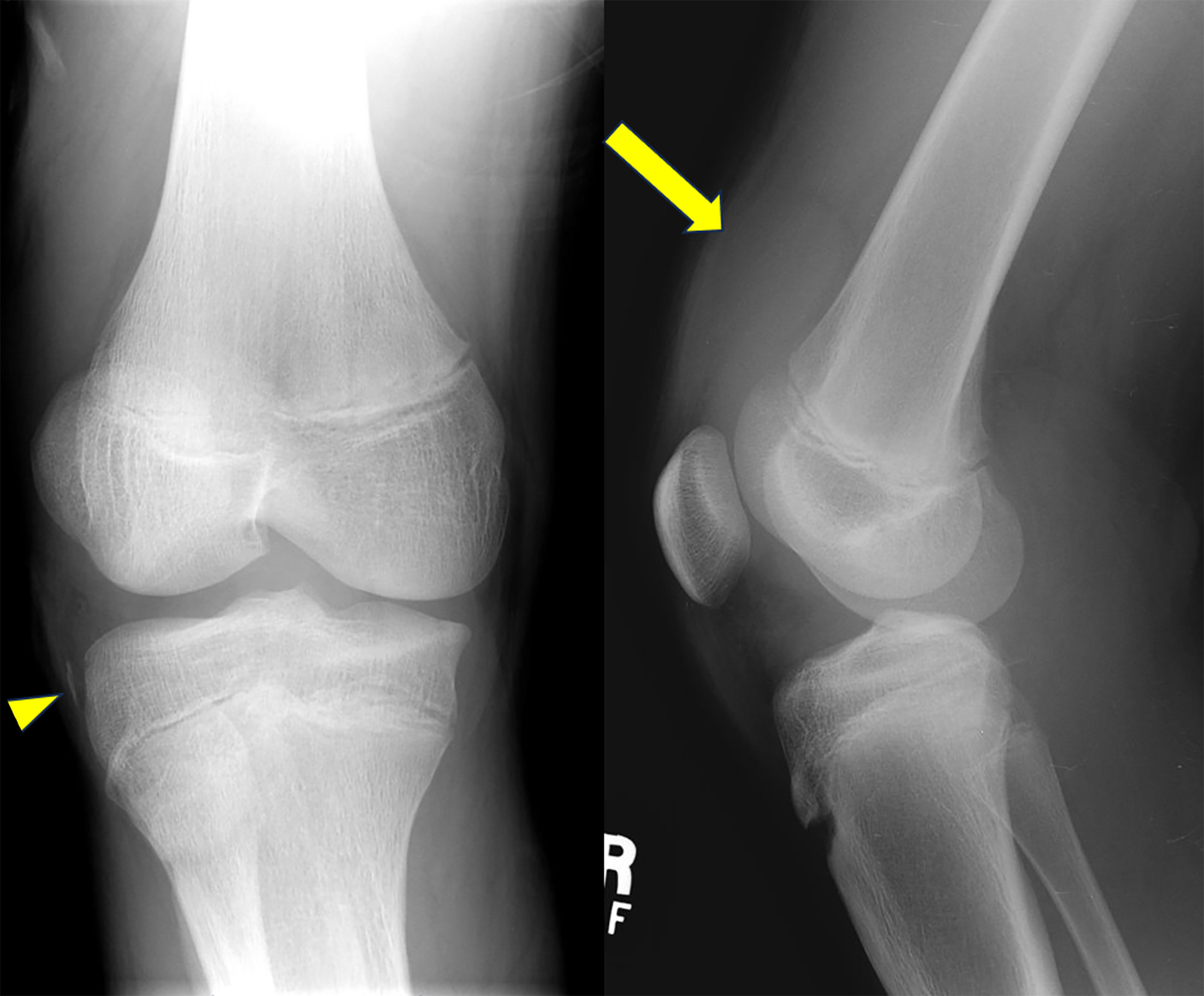
A Segond fracture is suggested by an elliptical or curvilinear-shaped bone fragment positioned parallel to the lateral margin of the tibial plateau just below the articular surface on a knee radiograph (Figures 1 and 2). 1 The avulsed bone fragment may be difficult to see on radiographs. CT may be necessary for confirmation. The associated anterior cruciate ligament (ACL) tear would not be identified. The “lateral capsular sign” is the descriptive term used to describe the radiographic appearance. 2 On a plain radiograph, an anteroposterior view (AP) of the patellofemoral joint is the best view to see the lateral capsular sign. 3
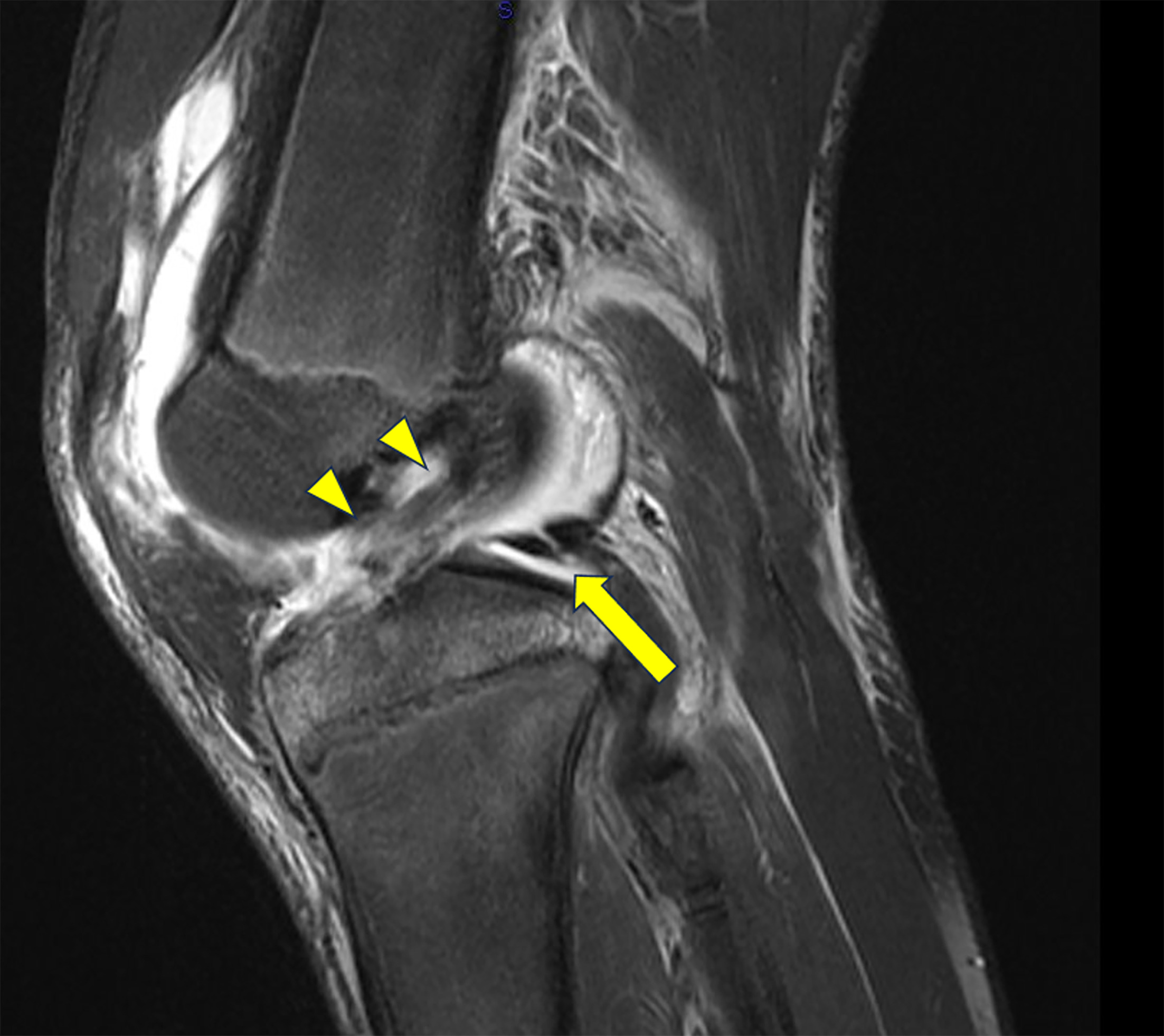
MRI is the preferred modality for full examination of the knee joint to demonstrate the extent of the injury to the ACL, the most common deep knee structure to be damaged. 4
Diagnosis
Segond fracture with ACL tear.
The differential diagnosis is an avulsion fracture of the fibular head resulting in the arcuate sign on imaging. This sign is seen on radiographs and cross-sectional imaging and indicates an avulsion fracture to the fibular head. The fibular head avulsion is a fracture at the insertion of the posterolateral ligaments. On AP view, one may see a linear lucency through the fibular head that generally is seen as a horizontal bone fragment. This stands in contrast with the Segond fracture, which involves the lateral capsular sign that is indicative of an avulsion fracture at the tibial head and is more vertical in position. 1,5
Other differential considerations include iliotibial band (ITB) avulsion, a fracture resulting from compression, occurring either in the lateral condyle of the tibia or the femoral condyle, accompanied by fragmentation, and posterolateral tibial plateau fracture. Imaging can be used to confirm one diagnosis over another. The key aspect to look for is the location of the avulsion. For instance, in ITB avulsion, the imaging would show the avulsion at the lateral condyle of the proximal tibia (Gerdy’s tubercle). 1
Discussion
Segond fractures are avulsion fractures, where a bony fragment is avulsed from the lateral margin of the tibial plateau with an associated tear in the ACL. 5
Segond fractures with ACL damage usually result from a traumatic event to the lateral aspect of the knee that results when there is a forceful internal rotation and varus stress on the knee. 6
This type of fracture is associated with rupture of the ACL as well as internal derangements, particularly meniscal and collateral ligament injuries. 2 In adults, a Segond fracture is predictive for the presence of a torn ACL in 75-100% of cases. However, for the pediatric population, this may not be the case, as Segond fractures can occur in isolation. Segond fractures are uncommon in adolescence, with only 6% of cases of ACL repairs. 3
There is currently speculation over the role played by the relatively recently discovered anterolateral ligament in the underlying structure that becomes initially compromised in a Segond fracture. 2
On imaging, the curvilinear avulsed bone fragment (lateral capsular sign) is found adjacent to the proximal portion of the tibia. 1,2 (Figure 1) Plain x-rays can make the diagnosis. The presence of the lateral capsular sign suggests the diagnosis of the Segond fracture. It is important to note, however, that an MRI is important to diagnose and define an internal derangement of the knee and the possible association of an ACL tear (Figure 2). 1,5
Treatment of a Segond fracture depends on the extent of the injury, especially the presence of an ACL tear or other internal derangement. The fracture itself does not usually need treatment. Initial treatment is usually conservative and supportive. Surgical repair is usually focused on the injured ACL. Follow-up 2 years after surgical repair of a Segond fracture and reconstruction of the ACL demonstrated positive outcomes with no major complications. 7 There was no sign of deterioration of the range of motion of the knee joint in this period. It is unknown whether Segond fractures heal spontaneously or require surgical intervention. 7
Generally, prognosis appears favorable for Segond fractures. Surgical repair is not always required to repair such a fracture. Also, Segond fractures may be able to heal without intervention. However, other associated injuries to ligaments and menisci could be a limiting factor. 3,8 If conservative treatment is contemplated, MR examination should be considered to examine the knee joint.
Conclusion
The “lateral capsular sign,” an elliptical-shaped skeletal fragment along the outside edge of the tibial plateau, is a characteristic of a Segond fracture usually associated with an ACL tear. Although this sign can be seen on conventional radiographs, MRI offers a more thorough evaluation of knee joint structures and verifies ACL involvement. Imaging should be used to explore for other potential injuries and diagnoses, such as the arcuate sign indicating fibular head avulsion. The best therapeutic approach requires a prompt and precise diagnosis. Surgery to correct the avulsion and ACL reconstruction are frequently used in the management of Segond fractures with ACL tears. With surgical intervention, there is a favorable prognosis.
References
- Davis D, Post W. Segond fracture: lateral capsular ligament avulsion. J Orthop Sports Phys Ther. 1997;25(2):103-106. doi:10.2519/jospt.1997.25.2.103.
- Ringenberg J, Sealy D, Tiller R. Isolated Segond fracture in a pediatric patient. Phys Sportsmed. 2015;43(2):188-191. doi:10.1080/00913847.2015.1037229.
- Skinner E, Davis D, Varacallo M. StatPearls. 2023.
- Roberts C, Towers J, Spangehl M, Carrino J, Morrison W. Advanced MR imaging of the cruciate ligaments. Radiol Clin North Am. 2007;45(6):1003-1016. doi:10.1016/j.rcl.2007.08.007.
- Yeo P, Seah A, Visvalingam V. Anterior cruciate ligament rupture and associated segond fracture: incidence and effect on associated ligamentous and meniscal injuries. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2022;30:36-40. doi:10.1016/j.asmart.2022.09.002.
- Albtoush O, Horger M, Springer F, Fritz J. Avulsion fracture of the medial collateral ligament association with Segond fracture. Clin Imaging. 2019;53:32-34. doi:10.1016/j.clinimag.2018.09.006.
- Ferretti A, Monaco E, Wolf M. Surgical treatment of segond fractures in acute anterior cruciate ligament reconstruction. Orthop J Sports Med. 2017;5(10). doi:10.1177/2325967117729997.
- Slagstad I, Parkar A, Strand T, Inderhaug E. Incidence and prognostic significance of the segond fracture in patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med. 2020;48(5):1063-1068. doi:10.1177/0363546520905557.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Segond Fracture with an Anterior Cruciate Ligament Tear. Applied Radiology. 2025. doi:10.37549/JPCR-25-0026.