Slipped Capital Femoral Epiphysis
Journal of Pediatric Case Reports — Vol. 1 , Issue 2
Published: April 1, 2026
1 School of Medicine, Wayne State University, Detroit, Michigan
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Slipped capital femoral epiphysis (SCFE) typically affects adolescents aged 8-15 and has a multifactorial etiology, with risk factors related to race, obesity, and seasonal variation. Patients typically present with a limp and pain localized to the groin, lateral or posterior hip, thigh, or ipsilateral knee. Radiographic findings include physeal widening, irregularity, and decreased epiphyseal height on anteroposterior views. Prompt recognition and surgical management are essential to prevent further slippage, preserve femoral head vascularity, and restore mobility.
Keywords
musculoskeletal, hips, trauma
Categories
Case Summary
An adolescent male was referred to an ambulatory orthopedic surgery clinic with a 1-week history of a painless limp.
Imaging Findings
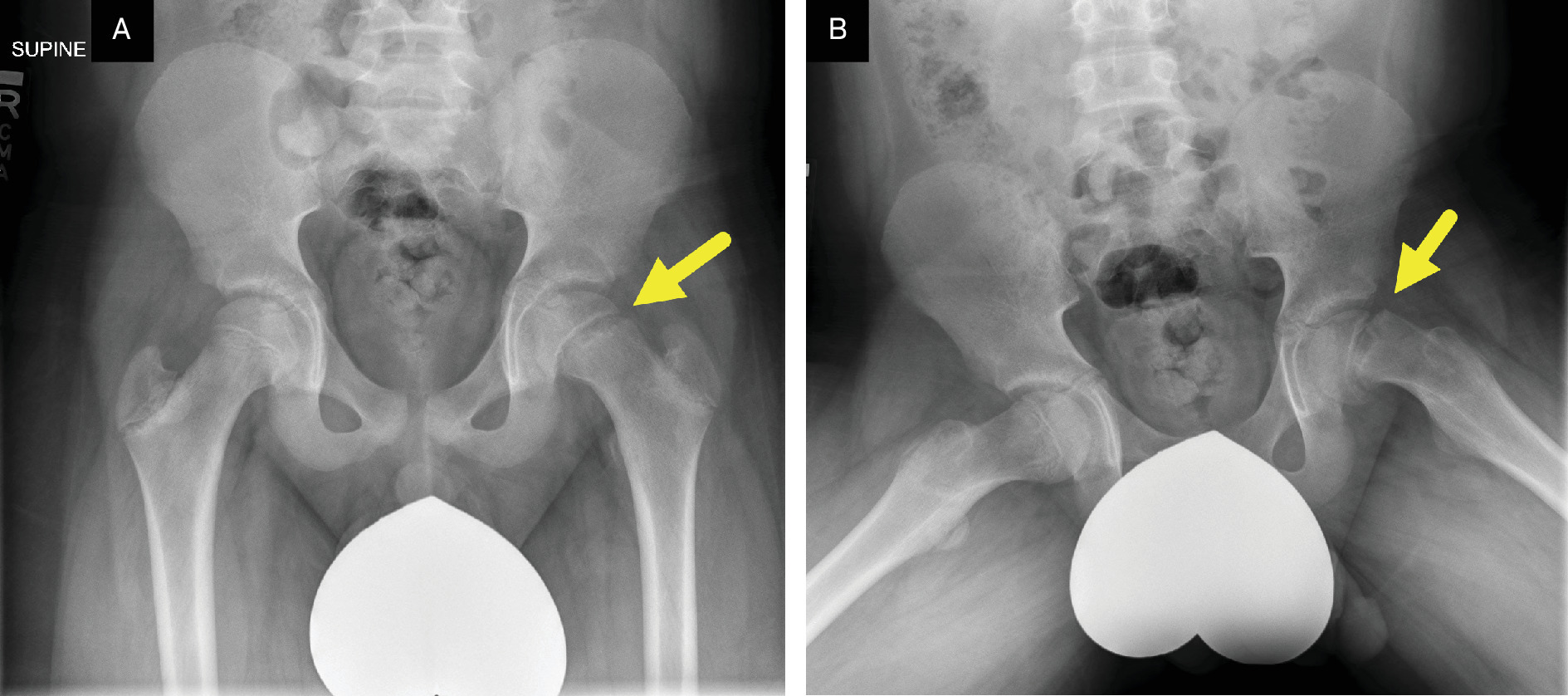
Radiograph of the hips (Figure 1) showed mild widening of the left proximal femoral physis and medial displacement of the left femoral head.
Diagnosis
Slipped capital femoral epiphysis (SCFE).
The differential diagnosis for SCFE includes idiopathic avascular necrosis of the femoral head (Legg-Calvé-Perthes disease), femoral neck stress fracture, adductor muscle strain, septic arthritis, or osteomyelitis.
Discussion
SCFE is the most common hip disorder in adolescents. It typically affects children between 8 and 15 years of age, with a US incidence of 10.8 cases per 100,000.1,2 Bilateral involvement occurs in 18-50% of patients, with 50-60% of those being simultaneous.3 In children who develop sequential bilateral SCFE, 80-90% of the contralateral slips occur within 18 months of the initial diagnosis.3
SCFE remains a diagnostic challenge due to its gradual onset and nonspecific symptoms, which often mimic other musculoskeletal conditions. Children typically present with chronic hip, groin, or thigh pain that may radiate to the ipsilateral knee. The pain usually worsens with activity and improves with rest. Additional clinical signs include limping, stiffness, and a reduced range of hip motion.4,5 A history of trauma is uncommon. SCFE occurs when the capital femoral epiphysis “slips,” displacing posteriorly and inferiorly through the weakened, fractured growth plate. While the condition is often idiopathic, contributing factors include mechanical shear stress across the physis and conditions that reduce physeal integrity or increase axial load, such as obesity and endocrine disorders.4
The risk of SCFE is influenced by several demographic factors. Males are significantly more likely to develop SCFE than females (OR 1.73; 95% CI, 1.51‐1.97).6 Seasonal variation has been observed in North America, with higher incidence rates during the summer and fall, likely due to increased activity.6 SCFE is also more common in the northeastern United States and among African American children. Prompt and accurate diagnosis is critical, as delayed treatment can lead to serious complications, including avascular necrosis (AVN) and early-onset degenerative hip arthritis.
Due to its nonspecific presentation, SCFE can be mistaken for other hip pathologies, including femoroacetabular impingement, Legg-Calvé-Perthes disease, and hip dysplasia. Given the risk of serious complications if left untreated, radiographs should be obtained in any child with SCFE included in the differential diagnosis.
SCFE is classified by clinical stability and severity, with newer classification systems emphasizing physeal stability due to its strong predictive value for complications such as AVN. Clinically, SCFE is divided into stable and unstable forms. In stable SCFE, the child can bear weight—with or without crutches—indicating preserved blood supply to the femoral head and a very low risk of AVN, often approaching 0%.7 These patients generally have favorable outcomes with appropriate treatment. In contrast, unstable SCFE is characterized by an inability to ambulate due to pain and physeal instability. This form is associated with a significantly higher risk of osteonecrosis, with reported rates ranging from 20% to 50%, and requires urgent surgical intervention to stabilize the physis and protect vascular integrity.7
Plain-film radiography remains the gold standard for diagnosing SCFE. Anteroposterior (AP) pelvis and frog-leg lateral views of both hips should be obtained in patients with symptoms of stable SCFE. In patients with suspected unstable SCFE, the frog-leg view should be avoided and replaced by a cross-table lateral view to minimize displacement risk. Key radiographic features of SCFE include physeal widening or irregularity compared with the contralateral side, decreased epiphyseal height on AP views, and loss of the anterior concavity of the femoral neck on lateral views. The “metaphyseal blanch sign”—a crescent-shaped area of increased density seen on AP radiographs—is caused by superimposition of the posteriorly and inferiorly displaced epiphysis over the metaphysis. Chronic SCFE may demonstrate metaphyseal cystic changes, remodeling, or a periosteal reaction. In severe or longstanding cases, chondrolysis and subchondral bone changes involving both the femur and acetabulum may also be observed.8
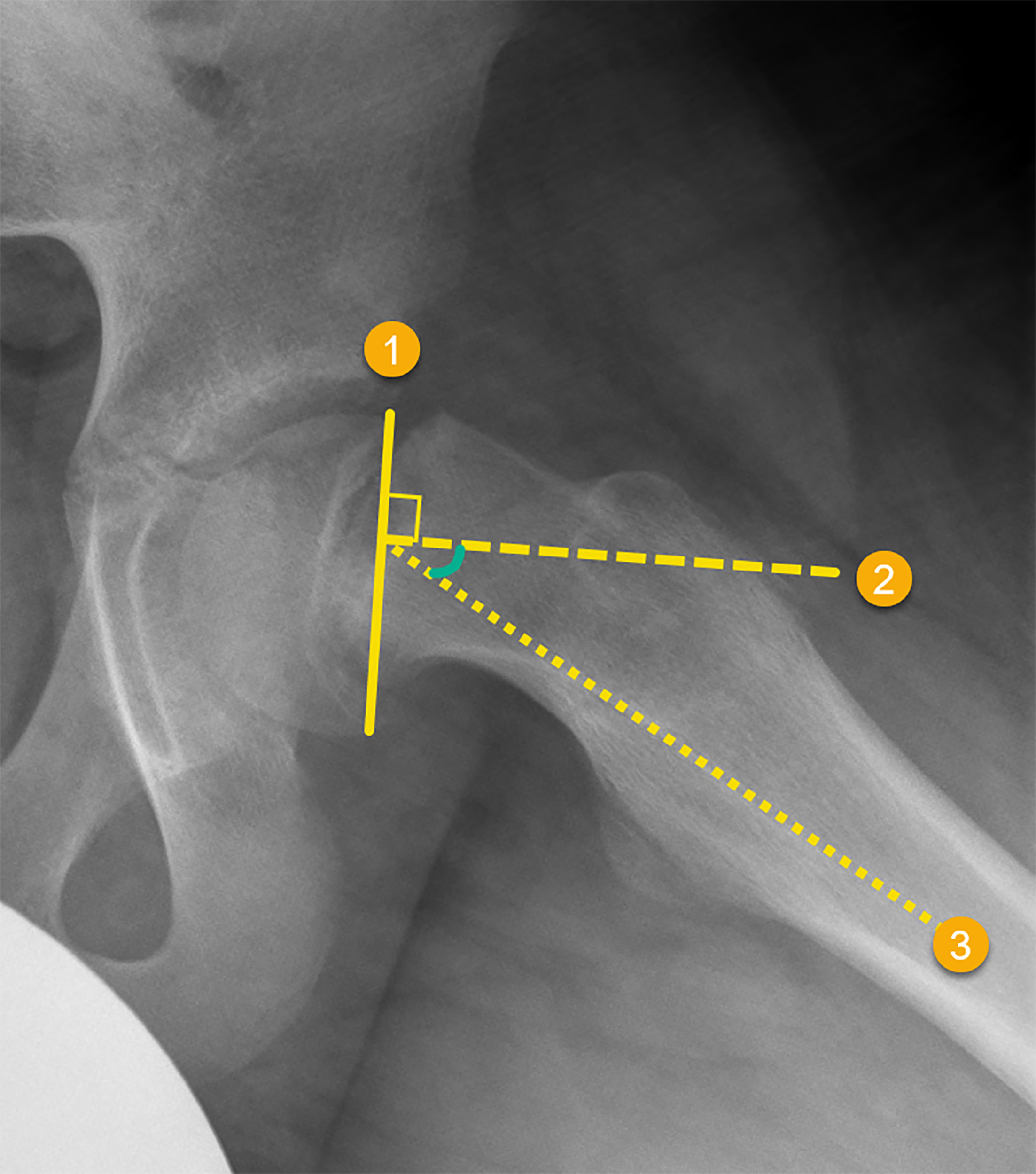
SCFE severity can be assessed radiographically using 2 primary methods: the percentage of epiphyseal displacement and the Southwick angle. The first method estimates the degree of slippage relative to the metaphyseal width: mild (< 1/3), moderate (1/3-1/2), and severe (>1/2). A more precise and prognostically useful measurement is the Southwick angle, typically assessed on frog-leg lateral radiographs. This angle is calculated in several steps (Figure 2). First, a line is drawn connecting the margins of the capital femoral epiphysis, a second line is drawn perpendicular to the first, and a third line is drawn along the axis of the femoral diaphysis. The angle between the second and third lines is measured. This value is then compared with the corresponding angle on the contralateral side, and the difference yields the final Southwick angle. Mild SCFE is defined as an angle less than 30°, moderate as 30-50°, and severe as greater than 50°.9 Increasing angular deformity is associated with a higher risk of early-onset degenerative hip disease.
In the early stages of SCFE, radiographs and CT scans may fail to detect subtle or impending slips. MRI is more sensitive than radiographs for detecting early or pre-slip changes. Early MRI findings include physeal widening, marrow edema (best seen on T1-weighted images), joint effusion (best appreciated on T2-weighted images), and early signs of slippage.10 Despite its higher sensitivity, MRI is typically reserved for cases in which SCFE is suspected but not confirmed on radiographs, or when further evaluation of complications is needed after diagnosis.
The primary goal of SCFE management is to prevent further slippage of the femoral head and to reduce the risk of complications such as AVN, chondrolysis, and early osteoarthritis. Chondrolysis—characterized by progressive cartilage loss and joint stiffness—affects 1-7% of patients.7 Residual deformities may lead to early osteoarthritis in 25-50% of cases.7
In situ screw fixation is the standard treatment for stable SCFE and serves to prevent further slippage. In more severe or unstable cases, the modified Dunn procedure aims to correct proximal femoral deformity, stabilize the epiphysis, and preserve the femoral head’s vascular supply, thereby reducing the risk of AVN. When indicated, capsulotomy may be performed to reduce intracapsular pressure and mitigate ischemic injury in patients with unstable SCFE.11 Despite these interventions, treatment remains technically complex, and careful surgical planning is essential to achieve optimal outcomes.
Conclusion
SCFE typically affects adolescents aged 8-15 and has a multifactorial etiology with risk factors related to race, obesity, and seasonal variation. Patients typically present with a limp and pain localized to the groin, lateral or posterior hip, thigh, or ipsilateral knee. Radiographic findings include physeal widening, irregularity, and decreased epiphyseal height on AP views. Prompt recognition and surgical management are essential to prevent further slippage, preserve femoral head vascularity, and restore mobility.
References
- Johns K, Mabrouk A, Tavarez M. In: StatPearls [Internet]. 2023.
- Lehmann C, Arons R, Loder R, Vitale M. The epidemiology of slipped capital femoral epiphysis: an update. J Pediatr Orthop. 2006;26(3):286-290. doi:10.1097/01.bpo.0000217718.10728.70.
- Loder R. The demographics of slipped capital femoral epiphysis an international multicenter study. Clin Orthop Relat Res. 1996;322(322):8-27. doi:10.1097/00003086-199601000-00003.
- Novais E, Millis M. Slipped capital femoral epiphysis: prevalence, pathogenesis, and natural history. Clin Orthop Relat Res. 2012;470(12):3432-3438. doi:10.1007/s11999-012-2452-y.
- Uvodich M, Schwend R, Stevanovic O. Patterns of pain in adolescents with slipped capital femoral epiphysis. J Pediatr. 2019;206:184-189. doi:10.1016/j.jpeds.2018.10.050.
- Miles D, Wilson A, Scull M, Moses W, Quigley R. A new look on the epidemiology of slipped capital femoral epiphysis: a topic revisited. J Pediatr Soc North Am. 2023;5(4). doi:10.55275/JPOSNA-2023-705.
- Peck D, Voss L, Voss T. Slipped capital femoral epiphysis: diagnosis and management. Am Fam Physician. 2017;95(12):779-784.
- Hesper T, Zilkens C, Bittersohl B, Krauspe R. Imaging modalities in patients with slipped capital femoral epiphysis. J Child Orthop. 2017;11(2):99-106. doi:10.1302/1863-2548-11-160276.
- Boyer D, Mickelson M, Ponseti I. Slipped capital femoral epiphysis. long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg. 1981;63(1):85-95. doi:10.2106/00004623-198163010-00011.
- Balch Samora J, Adler B, Druhan S. MRI in idiopathic, stable, slipped capital femoral epiphysis: evaluation of contralateral pre-slip. J Child Orthop. 2018;12(5):454-460. doi:10.1302/1863-2548.12.170204.
- Aprato A, Conti A, Bertolo F, Massè A. Slipped capital femoral epiphysis: current management strategies. Orthop Res Rev. 2019;11:47-54. doi:10.2147/ORR.S166735.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Slipped Capital Femoral Epiphysis. Journal of Pediatric Case Reports. 2026;1(2). doi:10.37549/JPCR-26-0085.