Spinal Muscular Atrophy
Journal of Pediatric Case Reports — Vol. 1 , Issue 2
Published: May 1, 2026
1 University of Arizona College of Medicine-Phoenix, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Spinal muscular atrophy (SMA) is an inherited neuromuscular disorder characterized by progressive muscle weakness. It has varying clinical severity, ranging from mild proximal muscle weakness to death from restrictive lung disease. The diagnosis is confirmed by genetic testing. Treatment includes survival motor neuron (SMN2) splicing modulator nusinersen, which may be challenging to administer intrathecally as patients develop varying degrees of scoliosis over time, making midline or paramedian lumbar punctures difficult. Patients with complex spinal anatomy may benefit from preprocedural and intraprocedural imaging to allow for a transforaminal approach for the intrathecal administration of nusinersen. Additional SMA treatments include risdiplam, a newer, oral splicing modulator, or SMN1 gene replacement therapy with Zolgensma.
Keywords
neuromuscular, spine, congenital
Categories
Case Summary
A 21-year-old man with type 1 spinal muscular atrophy (SMA) presented with initial onset of symptoms at 5 months of age, including delayed milestones and the inability to sit independently. The diagnosis was confirmed by genetic testing, with no copies of the survival motor neuron 1 (SMN1) gene and 3 copies of the SMN2 gene. The expanded Hammersmith Functional Motor Scale score is 0, and the Revised Upper Limb Module for SMA is 1. Additionally, he is ventilator dependent and requires BiPAP at night. Spinal fixation from C4 to S1 was performed for severe levoscoliosis. He began intrathecal (IT) nusinersen (Biogen, Cambridge, Massachusetts) at 17 years of age. Since beginning the IT nusinersen, he has greater hand movement and an improvement in his voice quality.
Imaging Findings
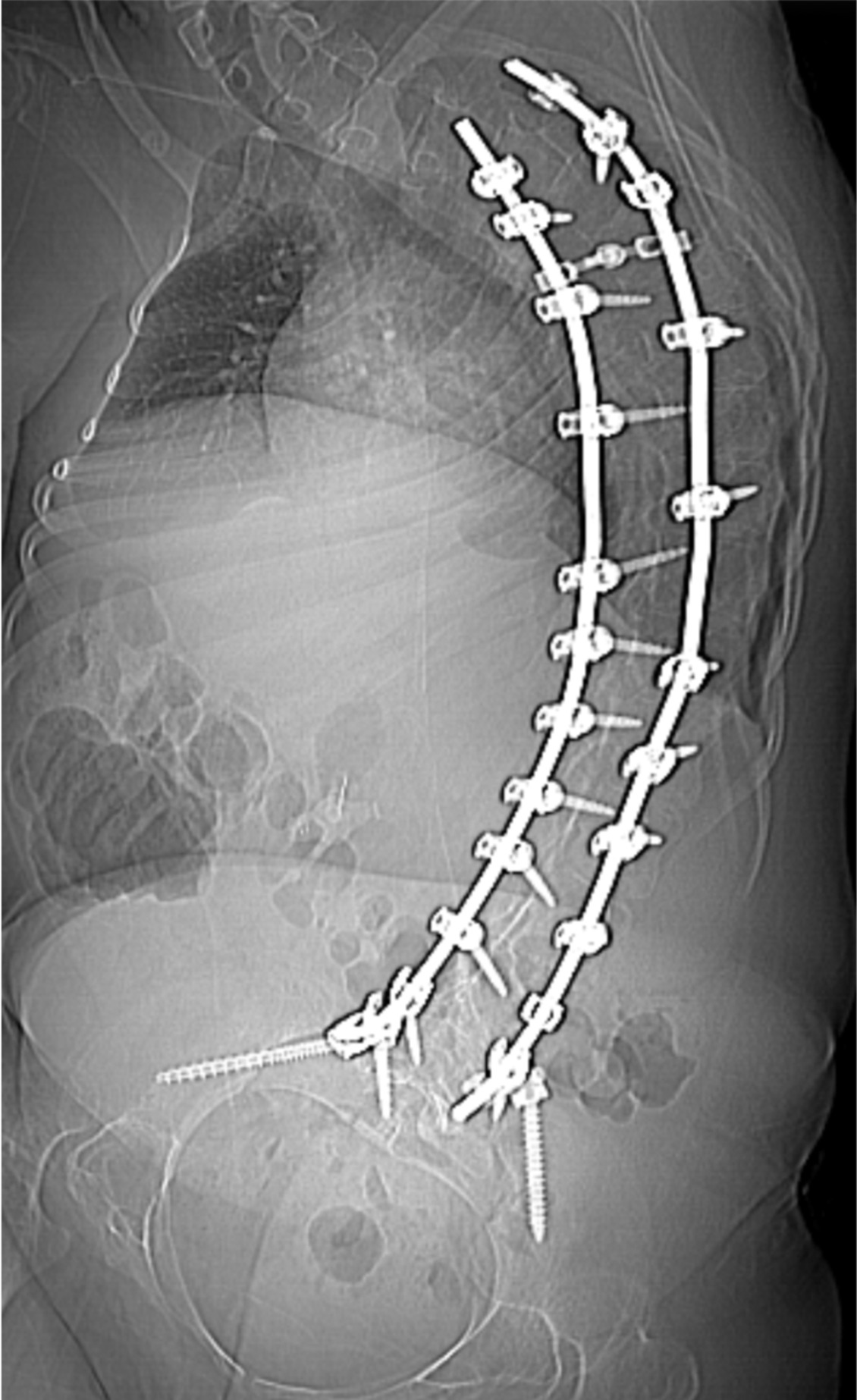
Figure 1. Scout image of a CT of the spine demonstrating the presence of a severe levoconvex rotary scoliosis of the thoracolumbar spine with spinal fixation.
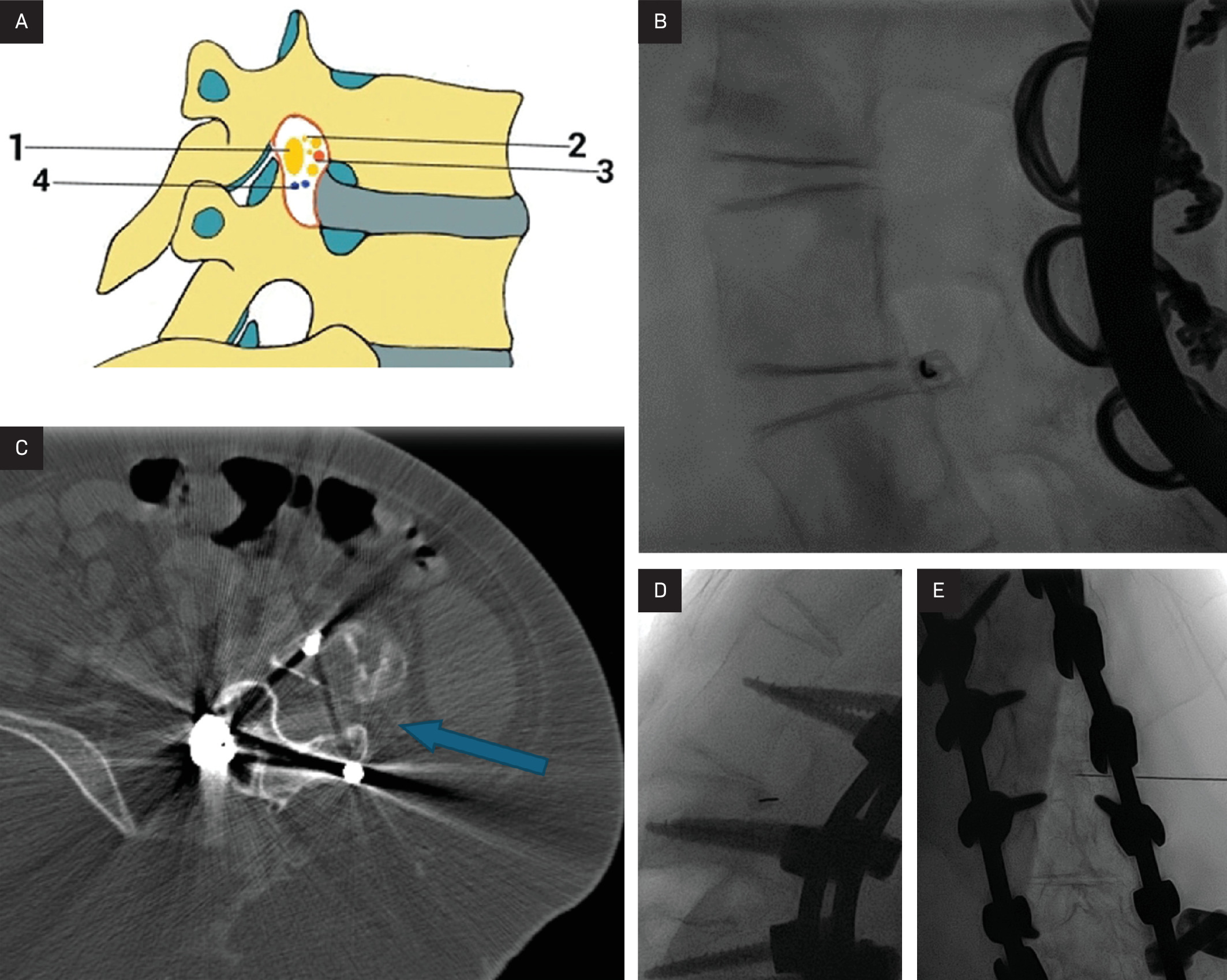
Figure 2A-C. 2A) CT axial image of the lumbar spine demonstrating planned left transforaminal access (blue arrow) for intrathecal nusinersen administration, 2B) Lateral fluoroscopic view of the lumbar spine with the spinal needle (blue arrow) entering the inferior-most aspect of the neural foramen for IT nusinersen, to avoid the neurovascular bundle in the upper 2/3 of the foramen, and 2C) Frontal fluoroscopic image demonstrating that the spinal needle tip (blue arrow) is near the midline of the thecal sac.
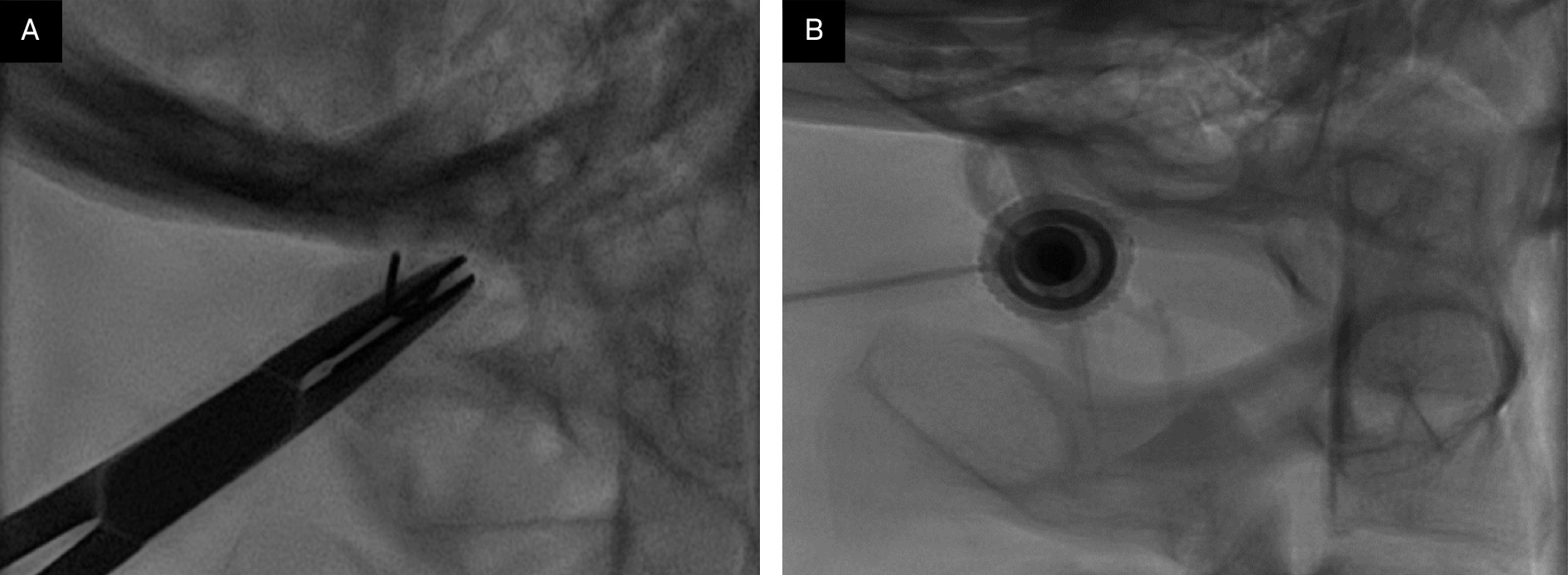
Figure 3. C1-2 puncture.
Diagnosis
SMA.
The differential diagnosis of SMA is extensive and includes many conditions that present with severe hypotonia. Possible conditions include congenital muscular and neuropathic disorders. For SMA types 3 and 4, a limb-girdle muscular dystrophy is the main differential diagnosis.
Discussion
SMA is an inherited, autosomal-recessive neuromuscular disorder most often caused by a homozygous deletion or mutation of the SMN1 gene on chromosome 5q13 with absent exon 7, which results in absent or deficient levels of SMN protein. A second and nearly identical gene, SMN2, produces low levels of functional SMN protein that fails to compensate for the loss of SMN1.1,2 SMN facilitates the assembly of spliceosomal small nuclear ribonucleoprotein particles, which are thought to function in motor neuron growth and neuromuscular maturation.3 Over time, SMA results in the degeneration of anterior horn cells in the spinal cord with associated destruction of alpha motor units in lower motor neurons.
SMA presents with varying clinical phenotypes and is classified into 5 main subtypes, based on severity and age of onset. All are characterized by progressive muscle weakness, reduced tone, and atrophy. However, cognition is not affected. Type 0 is congenital SMA, which presents early in neonatal life as severe hypotonia, early respiratory failure, and severe weakness, with death occurring at birth or within the first month of life without treatment. Type 1 is also known as Werdnig-Hoffman disease and presents in the first 6 months of life with limited head control, hypotonia, areflexia, weakness of intercostal muscles, swallowing difficulties, and tongue fasciculations. Type 2, Dubowitz disease, is of intermediate severity, presenting between 6 and 18 months of age. Children with SMA 2 can sit but have hypotonia, areflexia, progressive scoliosis, and restrictive lung disease. Mortality is most commonly due to respiratory compromise, but 70% of patients survive until age 25. Type 3, Kugelberg-Welander disease, is mild SMA presenting after 18 months of age, with progressive proximal weakness in the legs more than the arms. Type 3 patients are ambulatory and typically do not have restrictive lung disease. Additionally, their life expectancy is not affected. Finally, type 4 is adult-onset SMA. It has the mildest phenotype and presents in patients older than 21 years of age, with progressive mild proximal weakness typically not impairing ambulation or affecting life expectancy.4 With treatment, approximately two-thirds to three-fourths of patients achieve meaningful improvement such as better muscle strength, functional mobility, and breathing.
If clinical history and physical exam findings raise suspicion for SMA, the diagnosis is confirmed by molecular genetic testing to detect homozygous exon 7 deletion in the SMN1 gene, which is 100% specific for the diagnosis of SMA. Around 5% of patients with SMA are compound heterozygotes with a single SMN1 deletion and a frameshift, nonsense, or missense mutation in the other SMN1 copy. SMN2 differs from SMN1 by a single nucleotide, which disrupts a splice enhancer in exon 7, producing an unstable protein that is unable to compensate for the loss of SMN1. However, approximately 10-20% fully functional, full-length transcripts are generated from SMN2. There are 0-8 SMN2 copies in the genome, which is inversely correlated with disease severity. A higher copy number of SMN2 is often able to produce a milder type 2 or 3 phenotype of SMA. In the normal population, the SMN2 copy number varies from 0 to 3 copies, with 15% of normal individuals having no SMN2. An analysis of 625 unrelated Spanish patients with SMA showed that the majority of individuals with type 1 SMA had 1-2 SMN2 copies, most people with type 2 SMA had 3 gene copies, and those with type 3 had 3-4 SMN2 copies.5 SMN2 copy number detection may be performed to prognose disease severity.6 Additional tests, including electromyography, muscle biopsy, and creatine kinase, may also support the diagnosis, though these are not first-line tests.
There are no pathognomonic imaging findings diagnostic of SMA. However, over time children may develop scoliosis because of the imbalance between the flexor and extensor muscles of the trunk, typically leading to a C-shaped, neuromuscular curvature of the spine (Figure 1). If the degree of scoliosis is severe or progressive, instrumentation and spinal fusion are often necessary, as in this patient. The severity of the curvature, the vertebral rotation, and spinal fixation may make traditional IT access for nusinersen administration challenging.
Therapeutic approaches are multifold, including splicing modification of SMN2 via antisense oligonucleotides (ASO), small molecules that modulate SMN2 gene splicing, and SMN1 gene replacement therapy. Nusinersen (Spinraza, Biogen), the first molecular drug to treat SMA, is an intrathecally administered ASO that promotes the inclusion of exon 7 in mRNA transcripts of SMN2, resulting in translation of a higher level of fully functional SMN protein in liver, kidney, skeletal muscle, and central nervous system tissues. Patients with SMA have experienced significant improvement in motor function and extensions in life expectancy after receiving nusinersen.7 IT administration of nusinersen introduces unique challenges based on whether patients have simple or complex spinal anatomy (neuromuscular scoliosis, spinal fusion, or instrumentation) (Figure 1). There are several approaches that can be used to facilitate drug injection into the subarachnoid space. In children with uncomplicated spines, a midline lumbar puncture is performed. In those with complex spines, a transforaminal (Figure 2) or C1-2 approach may be performed (Figure 3). The authors prefer the transforaminal approach as it is safer and technically easier.8,9 Multiple reviews showed that complex SMA anatomy usually requires preprocedural imaging for route planning and intraprocedural guidance to access the subarachnoid space via the transforaminal approach.8,9
A newer, orally administered small molecule has also been developed to treat SMA, called risdiplam (Evrysdi, Genentech). This drug modulates SMN2 gene splicing by binding 2 pre-mRNA splice sites in exon 7, increasing the levels of full-length SMN mRNA and protein. It has enhanced specificity toward exon 7 splicing relative to other SMN2 splicing modifiers, decreasing the probability of off-target effects. Risdiplam crosses the blood-brain barrier, achieving systemic distribution with suitable half-life and predictable pharmacokinetics.10 Onasemnogene abeparvovec (Zolgensma, Novartis) is SMN1 gene replacement therapy, which uses a nonreplicating adeno-associated virus capsid carrying SMN1 complementary recombinant DNA to efficiently deliver wild-type SMN1 gene to motor neuron cells. A one-time intravenous injection leads to systemic expression of the SMN protein in SMA mice.11
Additionally, there are investigations relating to muscle-enhancing therapies that target SMN-independent factors and may provide additional therapeutic benefit in combination with SMN-targeting treatments. Reldesemtiv (an investigational drug) is a small-molecule troponin activator in fast skeletal muscles, reinforcing contraction and promoting muscle response to nervous stimulus.11 SRK-015 is a monoclonal antibody that selectively inhibits myostatin, promoting muscle cell growth, differentiation, and force in SMA mice.11 Additional research on SMN-independent factors is ongoing, and potential therapeutic targets include autophagosomes, which are increased in SMA motor neurons and may be decreased with IM injections of neurotrophic factor tetanus toxin heavy chain or intracerebroventricular administration of 3-MA.11 Additionally, SMA mice have been shown to have a deficiency in agrin expression, which is a synaptic organizer functioning in the efficiency of neuromuscular transmission, an effect that may be relieved with the administration of C-terminal fragment of agrin.12
Gene therapy has transformed types 0 and 1 SMA from a fatal disease into a treatable condition or decreases the severity of the disease. It is common for patients to show improved motor function and survival rates.
Conclusion
SMA is an inherited neuromuscular disorder characterized by progressive muscle weakness. It has varying clinical severity ranging from mild proximal muscle weakness to death from restrictive lung disease. The diagnosis is confirmed by genetic testing. Treatment includes SMN2 splicing modulator nusinersen, which may be challenging to administer intrathecally as patients develop varying degrees of scoliosis over time, making midline or paramedian lumbar punctures difficult. Patients with complex spinal anatomy may benefit from preprocedural and intraprocedural imaging to allow for a transforaminal approach for the IT administration of nusinersen. Additional SMA treatments include risdiplam, a newer, oral splicing modulator, or SMN1 gene replacement therapy with Zolgensma.
References
- Prior T, Leach M, Finanger E, Adam M, Ardinger H, Pagon R. GeneReviews® [Internet]. 2000.
- Kolb S, Kissel J. Spinal muscular atrophy. Neurol Clin. 2015;33(4):831-846. doi:10.1016/j.ncl.2015.07.004.
- Fan L, Simard L. Survival Motor Neuron (SMN) protein: role in neurite outgrowth and neuromuscular maturation during neuronal differentiation and development. Hum Mol Genet. 2002;11(14):1605-1614. doi:10.1093/hmg/11.14.1605.
- Burr P, Reddivari A. In: StatPearls [Internet]. 2021.
- Calucho M, Bernal S, Alías L. Correlation between SMA type and SMN2 copy number revisited: an analysis of 625 unrelated Spanish patients and a compilation of 2834 reported cases. Neuromuscul Disord. 2018;28(3):208-215. doi:10.1016/j.nmd.2018.01.003.
- Rouzier C, Chaussenot A, Paquis-Flucklinger V. Molecular diagnosis and genetic counseling for Spinal Muscular Atrophy (SMA). Arch Pediatr. 2020;27(7s):7S9-7S14. doi:10.1016/S0929-693X(20)30270-0.
- Paton D. Nusinersen: antisense oligonucleotide to increase SMN protein production in spinal muscular atrophy. Drugs Today (Barc). 2017;53(6):327-337. doi:10.1358/dot.2017.53.6.2652413.
- Mousa M, Aria D, Schaefer C. A comprehensive institutional overview of intrathecal nusinersen injections for spinal muscular atrophy. Pediatr Radiol. 2018;48(12):1797-1805. doi:10.1007/s00247-018-4206-9.
- Towbin R, Schaefer C, Kaye R, Abruzzo T, Aria D. The complex spine in children with spinal muscular atrophy: the transforaminal approach-A transformative technique. AJNR Am J Neuroradiol. 2019;40(8):1422-1426. doi:10.3174/ajnr.A6131.
- Ratni H, Ebeling M, Baird J. Discovery of risdiplam, a selective Survival of Motor Neuron-2 (SMN2) gene splicing modifier for the treatment of Spinal Muscular Atrophy (SMA). J Med Chem. 2018;61(15):6501-6517. doi:10.1021/acs.jmedchem.8b00741.
- Messina S, Sframeli M. New treatments in spinal muscular atrophy: positive results and new challenges. J Clin Med. 2020;9(7):2222. doi:10.3390/jcm9072222.
- Boido M, De Amicis E, Valsecchi V. Increasing agrin function antagonizes muscle atrophy and motor impairment in spinal muscular atrophy. Front Cell Neurosci. 2018;12:17. doi:10.3389/fncel.2018.00017.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Spinal Muscular Atrophy. Journal of Pediatric Case Reports. 2026;1(2). doi:10.37549/JPCR-26-0082.