Thyroglossal Duct Cyst
Applied Radiology — Vol. 1 , Issue 1 , pp. 1 -3
Published: September 1, 2025
1 University of Arizona College of Medicine-Phoenix Campus, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Thyroglossal duct cysts are embryonic remnants of the thyroglossal duct. Although various imaging modalities such as sonography, CT, and MRI can be used to diagnose thyroglossal duct cysts, sonography remains the initial imaging technique used. CT and MRI can be used in selected cases.
Keywords
congenital anomaly, thyroid gland
Categories
Case Summary
An infant with a midline lumbar cutaneous hemangioma and a sacral dimple underwent MRI to evaluate for a tethered cord after an US revealed a low-lying conus medullaris. The MRI identified an asymptomatic small cystic mass at the root of the tongue.
Imaging Findings
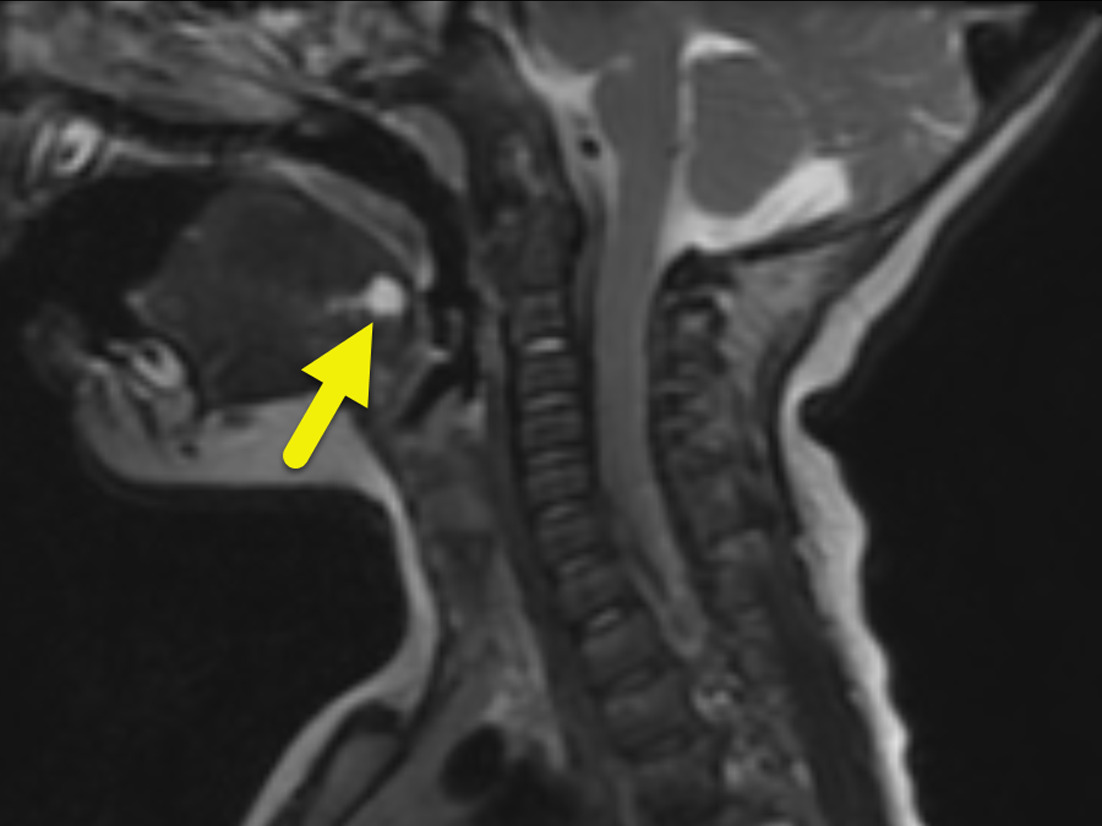
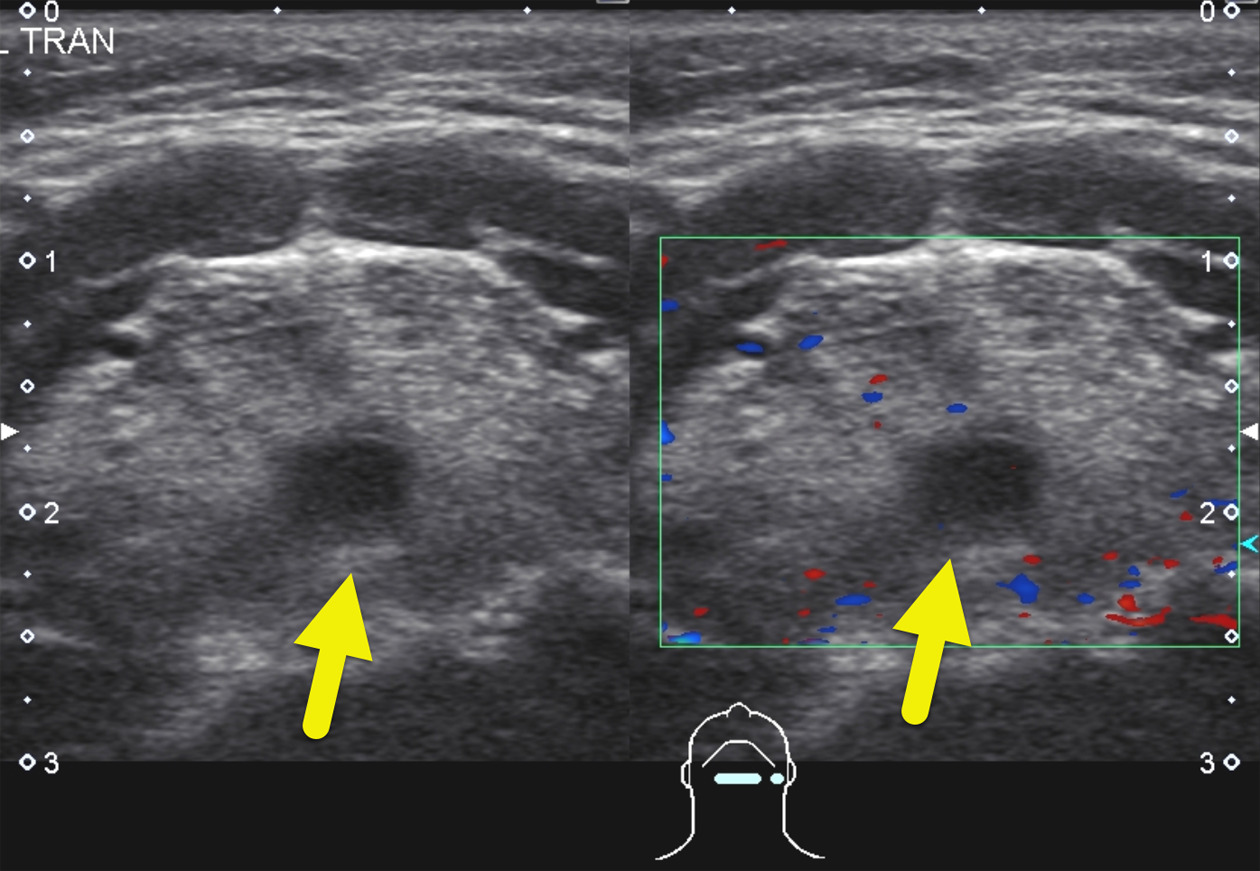
Initial MRI (Figure 1) showed a 5 mm T2, hyperintense mass at the root of the tongue. Follow-up US (Figure 2) confirmed the mass. On US, it appeared hypoechoic with no internal complexity or color Doppler flow.
Diagnosis
Thyroglossal duct cyst
Differential Diagnosis
Lingual thyroid, dermoid and epidermoid cysts, foregut duplication cysts, and hemangioma 1
Discussion
A thyroglossal duct cyst (TGDC) is the most common congenital neck mass. They arise during the development of the thyroid. The thyroid anlage, an endodermal structure formed during the 4th week of gestation and derived from the 1st and 2nd pharyngeal pouches, descends caudally from the root of the tongue to its final position below the hyoid bone at the root of the neck by the 7th week of gestation. As the thyroid anlage descends, it forms the thyroglossal duct. The duct obliterates by the 10th week of gestation. However, failure to do so will result in a TGDC. 2 Therefore, a TGDC can occur at any point along the course of the thyroglossal duct, from the foramen cecum at the root of tongue to the thyroid gland. Most TGDCs occur at or below the hyoid bone. While up to 25% of TGDCs are suprahyoid, the majority of these are identified in children. 1
TGDCs are relatively common, occurring in 7% of the general population. 3 Management is dependent upon the cyst’s status and size as well as the patient’s symptoms and suitability for surgery. If a TGDC is infected, patients should be treated with antibiotics. Surgical or percutaneous drainage of larger, more complex infected cysts may be needed. 4 Ultimately, most cysts are resected due to the risk of infection or malignancy. The Sistrunk procedure is most performed. This procedure involves the resection of the cyst, mid-portion of the hyoid bone, and the remaining thyroglossal duct remnant to prevent recurrence. 5 Occasionally, patients who are not suitable candidates for surgery are treated with percutaneous injection of ethanol. 6
TGDCs are typically diagnosed via imaging with US, CT, or MRI. MRI shows hypointense T1-weighted and hyperintense T2-weighted signal due to the fluid content. However, hyperintense signal on T1-weighted images may denote infected, hemorrhagic, or proteinaceous cyst fluid (Figure 1). 7 On US, uncomplicated cysts are anechoic or hypoechoic masses with no internal color Doppler flow (Figure 2). 7 CT demonstrates a smooth, well-circumscribed mass with thin walls and occasional septations or wall enhancement if complicated by infection.
Thyroglossal duct carcinoma occurs in <1% of patients with a TGDC. Up to 95% of these carcinomas arise from remnant thyroid tissue within the TGDC. 8 The vast majority of these malignancies are papillary thyroid carcinomas. 8 The non-thyrogenic tumors arising from a TGDC are squamous cell in origin. 9 On imaging, a solid mass and calcification within the cyst are potential worrisome findings that should lead to a fine needle aspiration biopsy. When a biopsy is performed, TGDCs will demonstrate thyroid follicles with ductal or cystic epithelium that may be pseudostratified columnar, ciliated columnar, simple cuboidal, squamous, or transitional. 10 Features concerning for malignancy include high degree of cellularity, papillary formations, and cells with enlarged nuclei.
The differential diagnosis for cystic neck masses includes dermoid cysts and branchial cleft. Dermoid cysts are located more superficially than TGDCs. They are derived from both ectoderm and mesoderm. Thus, they have keratinizing squamous epithelium, along with other dermal derivatives, on histology. 4,5 Branchial cleft cysts are part of a spectrum of branchial cleft anomalies. While their imaging appearance is like a TGDC, they occur more laterally, with a location dependent on the affected branchial apparatus. 5
The differential diagnosis for a congenital mass at the root of the tongue includes lingual thyroid, dermoid and epidermoid cysts, foregut duplication cysts, and hemangioma. 1 A lingual thyroid also represents a failure of thyroid anlage migration. In this anomaly, the thyroid or a portion of the thyroid remains at the foramen cecum. This appears as a solid mass on imaging. 123-I or 99m-Tc scans may be performed to confirm the diagnosis. 1 Dermoid and epidermoid cysts may occur at the root of the tongue or the floor of the mouth. 1 They can be difficult to distinguish on imaging. Dermoid tumors may contain fat elements while epidermoids are more cystic and have restricted diffusion. 1 Foregut duplication cysts occurring at the root of the tongue are rare. 1 They more commonly occur within the mediastinum or abdomen.
Conclusion
TGDCs are embryonic remnants of the thyroglossal duct. Although various imaging modalities such as sonography, CT, and MRI can be used to diagnose TGDCs, sonography remains the initial imaging technique used. CT and MRI can be used in selected cases.
References
- Fang W, Wiggins R, Illner A. Primary lesions of the root of the tongue. Radiographics. 2011;31(7):1907-1922. doi:10.1148/rg.317095738.
- Chou J, Walters A, Hage R. Thyroglossal duct cysts: anatomy, embryology and treatment. Surg Radiol Anat. 2013;35(10):875-881. doi:10.1007/s00276-013-1115-3.
- Amos J, Shermetaro C. StatPearls. 2022.
- Al-Dajani N, Wootton S. Cervical lymphadenitis, suppurative parotitis, thyroiditis, and infected cysts. Infect Dis Clin North Am. 2007;21(2). doi:10.1016/j.idc.2007.03.004l.
- Quintanilla-Dieck L, Penn E. Congenital neck masses. Clin Perinatol. 2018;45(4):769-785. doi:10.1016/j.clp.2018.07.012.
- Baskin H. Percutaneous ethanol injection of thyroglossal duct cysts. Endocr Pract. 2006;12(4):355-357. doi:10.4158/EP.12.4.355.
- Ahuja A, Wong K, King A, Yuen E. Imaging for thyroglossal duct cyst: the bare essentials. Clin Radiol. 2005;60(2):141-148. doi:10.1016/j.crad.2004.08.009.
- Glastonbury C, Davidson H, Haller J, Harnsberger H. The CT and MR imaging features of carcinoma arising in thyroglossal duct remnants. AJNR Am J Neuroradiol. 2000;21(4):770-774.
- Rayess H, Monk I, Svider P. Thyroglossal duct cyst carcinoma: a systematic review of clinical features and outcomes. Otolaryngol Head Neck Surg. 2017;156(5):794-802. doi:10.1177/0194599817696504.
- Yang Y, Haghir S, Wanamaker J, Powers C. Diagnosis of papillary carcinoma in a thyroglossal duct cyst by fine-needle aspiration biopsy. Arch Pathol Lab Med. 2000;124(1):139-142. doi:10.5858/2000-124-0139-DOPCIA.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Thyroglossal Duct Cyst. Applied Radiology. 2025;1(1):1-3. doi:10.37549/JPCR-25-0005.