1 John Sealy School of Medicine, University of Texas Medical Branch, Galveston, Texas
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital and University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Fibromatosis colli is the most frequent cause of congenital torticollis. Patients most commonly present in the first few weeks of life with a palpable mass of the sternocleidomastoid muscle. Other signs and symptoms include preferential head tilting and limited neck range of motion. US is the preferred initial imaging modality and reveals a fusiform or ellipsoid mass of the sternocleidomastoid muscle with clearly defined margins. Patients are treated with physical therapy aimed at stretching the affected muscle.
Keywords
fibromatosis colli, wry neck, congenital
Categories
Case Summary
A male neonate was referred for US due to a left neck mass that had doubled in size over the past week.
Imaging Findings
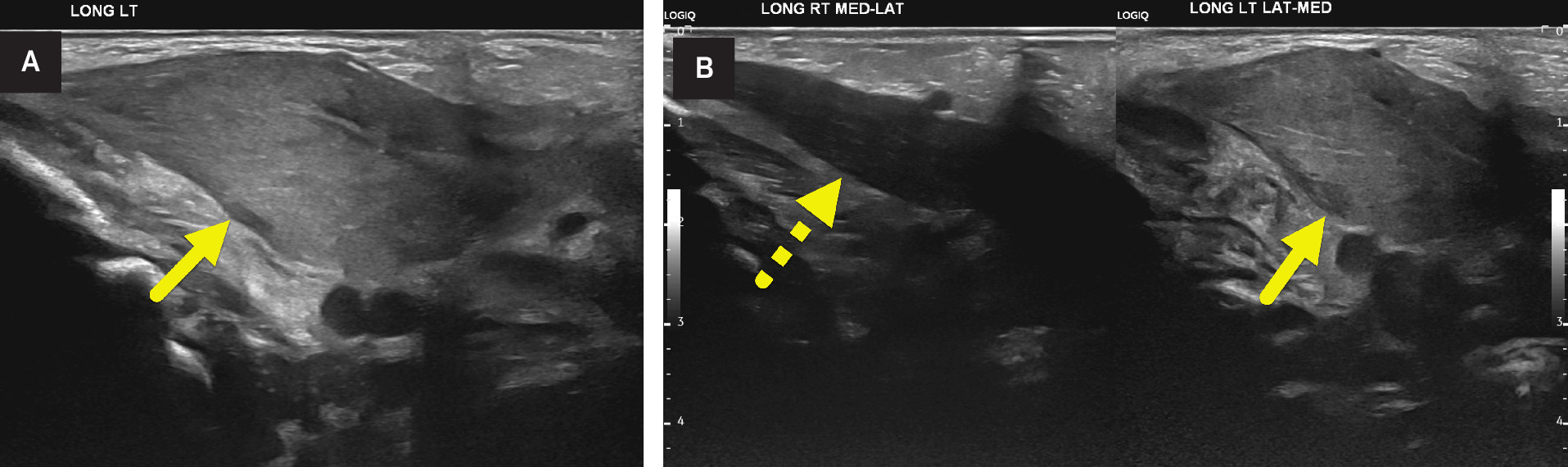
US (Figure 1) showed a hyperechoic mass-like enlargement of the left sternocleidomastoid muscle (SCM). The muscle had a fusiform shape in the longitudinal plane.
Diagnosis
Torticollis secondary to fibromatosis colli.
The differential diagnosis includes rhabdomyosarcoma, fibrosarcoma, neuroblastoma, branchial cleft cyst, and cervical lymphadenopathy. 1
Discussion
Torticollis, colloquially known as wry neck, is defined as a rotation of the head and neck due to contraction or fibrosis of the SCM or vertebral anomalies. 2 Vertebral abnormalities that may be identified include anomalies of C1 and C2, hemivertebrae, and fused vertebrae as in Klippel-Feil syndrome. Cases can be classified as either congenital or acquired after birth, with the vast majority categorized as congenital. 3 Congenital torticollis has been theorized to be caused by trauma during delivery, intrauterine malposition, and/or muscle ischemia. Congenital torticollis is the most common type of torticollis. Other causes are acquired and include trauma, gastroesophageal reflux disease, and soft-tissue neck infections.
Patients with congenital torticollis present with a limited range of motion of the head and neck and facial asymmetry because of shortening of the SCM. Prior research has shown that 2-29% of patients with congenital muscular torticollis also have developmental dysplasia of the hip. However, the incidence is controversial. The association is thought to be due to limited space in the uterus. 4
Fibromatosis colli is a rare condition of unknown cause that affects 0.4% of newborns. Patients present in the first few weeks of life with torticollis and neck swelling (more common on the right side). 5 Fibromatosis colli represents a benign proliferation of fibrous tissue within the SCM that may be caused by muscle compression and stretching. 5 Additionally, cervical venous compression during childbirth may decrease blood supply to the area, leading to compartment syndrome with edema, degeneration of muscle fibers, and fibrosis. Ultimately, this may lead to the deposition of type III collagen and fibrosis in the SCM. 6
US is the imaging modality of choice for the initial assessment of a pediatric neck mass and congenital torticollis due to its high diagnostic capability, low cost, lack of exposure to ionizing radiation, and is performed without sedation. 7 The modality has a sensitivity of 100% for detecting fibromatosis colli. 5 US images demonstrate a fusiform- or ellipsoid-shaped mass of variable echogenicity within the SCM. On real-time examination, the mass moves in sync with the SCM. 8
Other imaging is not needed to make or confirm the diagnosis. However, occasionally it is performed for other indications. CT shows isodense, diffuse enlargement of the affected SCM with normal surrounding fascial planes. 9 No calcifications, fat-stranding, or edema is seen. MRI can also show fusiform enlargement of the affected SCM. The muscle may appear slightly hyperintense on T2-weighted images. 10 Biopsy is not needed for diagnosis. If performed, it shows numerous spindle-shaped fibroblasts, multinucleated regenerating muscle giant cells, and atrophic muscle fibers. 11
Fibromatosis colli is treated conservatively with stretching exercise programs to elongate the SCM, correct the abnormal head position, and prevent the development of permanent torticollis and craniofacial asymmetry. The condition resolves in 90% of patients with physical therapy. 11 In cases refractory to conservative measures, tenotomy is offered.
Conclusion
Fibromatosis colli is the most common cause of congenital torticollis. Patients most commonly present in the first few weeks of life with a palpable mass of the SCM. Other signs and symptoms include preferential head tilting and limited neck range of motion. US is the preferred initial imaging modality and reveals a fusiform or ellipsoid mass of the SCM with clearly defined margins. Patients are treated with physical therapy aimed at stretching the affected muscle.
References
- Blythe W, Logan T, Holmes D, Drake A. Fibromatosis colli: a common cause of neonatal torticollis. Am Fam Physician. 1996;54(6):1965-1967.
- Tomczak K, Rosman N. Torticollis. J Child Neurol. 2013;28(3):365-378. doi:10.1177/0883073812469294.
- Gross P, Chipman D, Doyle S. The tilts, twists, and turns of torticollis. Curr Opin Pediatr. 2023;35(1):118-123. doi:10.1097/MOP.0000000000001194.
- von Heideken J, Green D, Burke S. The relationship between developmental dysplasia of the hip and congenital muscular torticollis. J Pediatr Orthop. 2006;26(6):805-808. doi:10.1097/01.bpo.0000235398.41913.51.
- Nasri S, Afilal I, Missaoui Z. Fibromatosis colli: a case report. Radiol Case Rep. 2022;17(3):693-695. doi:10.1016/j.radcr.2021.12.009.
- Li D, Wang K, Zhang W, Wang J. Expression of bax/bcl-2, TGF-β1, and type III collagen fiber in congenital muscular torticollis. Med Sci Monit. 2018;24:7869-7874. doi:10.12659/MSM.909064.
- Penny S. Sonographic diagnosis of fibromatosis colli. J Diagn Med Sonogr. 2006;22(6):399-402. doi:10.1177/8756479306294249.
- Patrick L, O’Shea P, Simoneaux S, Gay B, Atkinson G. Fibromatoses of childhood: the spectrum of radiographic findings. AJR Am J Roentgenol. 1996;166(1):163-169. doi:10.2214/ajr.166.1.8571869.
- Crawford S, Harnsberger H, Johnson L, Aoki J, Giley J. Fibromatosis colli of infancy: CT and sonographic findings. AJR Am J Roentgenol. 1988;151(6):1183-1184. doi:10.2214/ajr.151.6.1183.
- Ablin D, Jain K, Howell L, West D. Ultrasound and MR imaging of fibromatosis colli (sternomastoid tumor of infancy). Pediatr Radiol. 1998;28(4):230-233. doi:10.1007/s002470050337.
- Khan S, Jetley S, Jairajpuri Z, Husain M. Fibromatosis colli - a rare cytological diagnosis in infantile neck swellings. J Clin Diagn Res. 2014;8(11):FD08-FD09. doi:10.7860/JCDR/2014/10840.5154.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Torticollis in Neonates. Applied Radiology. 2025. doi:10.37549/JPCR-25-0017.