Tracheobronchomalacia
Journal of Pediatric Case Reports — Vol. 1 , Issue 1
Published: April 1, 2026
1 University of Arizona College of Medicine-Phoenix Campus, Phoenix, Arizona
2 Department of Radiology, Phoenix Children’s Hospital, Phoenix, Arizona
3 Department of Radiology, Cincinnati Children’s Hospital, University of Cincinnati College of Medicine, Cincinnati, Ohio
* Corresponding author: Richard B. Towbin (rtowbin@gmail.com)
Abstract
Pediatric tracheobronchomalacia is typically classified as primary disease. Patients commonly present with a “barking” or “brassy” cough, wheezing, and stridor. Other signs and symptoms include cyanosis, breathing difficulties, and frequent respiratory tract infections. Dynamic CT or MRI is the preferred imaging modality. On imaging, the airway is shown to collapse during expiration. Patients are supported medically in most instances. However, those with severe symptoms may be treated surgically.
Keywords
airway, chest, congenital
Categories
Case Summary
An older child with a history of cystic fibrosis presented for surveillance CT imaging.
Imaging Findings
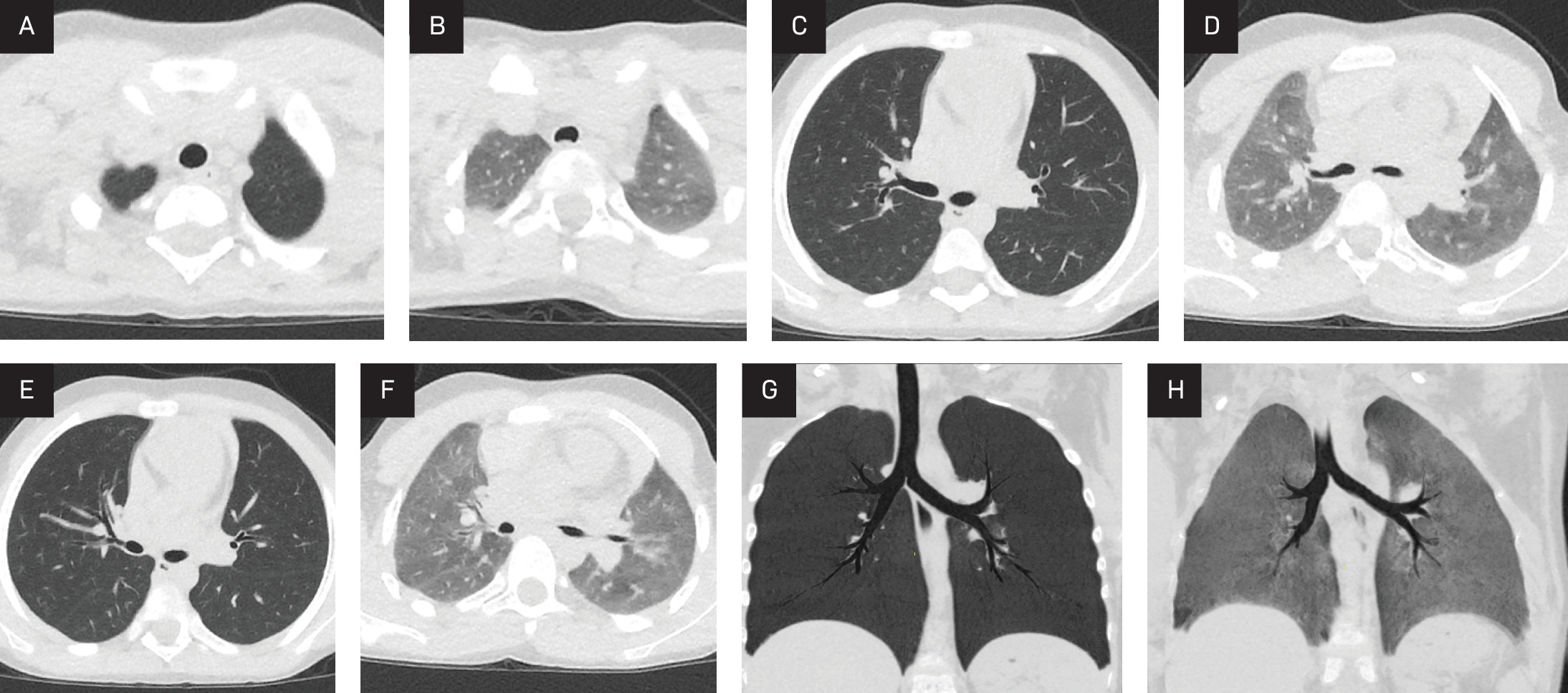
High-resolution chest CT (Figure 1) with inspiration and expiration shows a smaller caliber of the trachea and bronchi on expiration.
Diagnosis
Tracheobronchomalacia.
The clinical differential diagnosis for tracheobronchomalacia in adolescents includes subglottic stenosis, epiglottitis, vocal cord paralysis, bronchiolitis, subglottic stenosis, and syndromes such as Ehlers-Danlos.
Discussion
Tracheobronchomalacia refers to the dynamic collapse of large airways.1 The broad nature of the term makes it difficult to make a precise diagnosis. Tracheobronchomalacia can be primary in patients born with a collapsible airway, which may occur because of abnormal division of the esophagus and trachea during foregut separation.2 Causes include idiopathic, prematurity, or a result of genetic conditions such as Ehlers-Danlos syndrome, Hunter and Hurler syndromes, and trisomy 9 and 21. Secondary tracheomalacia can be from chronic pulmonary inflammation, trauma, masses compressing the airway, and long-term compression that weakens the tracheal cartilage. It is also associated with conditions that cause breakdown of the tracheal cartilage, such as prolonged tracheobronchitis, compression of nearby anatomy, intubation, and relapsing polychondritis, to name a few.2 Most children with tracheobronchomalacia have primary disease.
Primary tracheobronchomalacia occurs with an incidence between 1 in 1445 and 1 in 2100 live births. Most affected children are male (58-82% of cases). While it is more common in premature infants, tracheobronchomalacia can occur in term infants. Minor airway collapse may improve by 1-2 years of age. However, children with congenital cartilage disorders may experience worsening of symptoms over time.
Children with primary tracheobronchomalacia present with a “barking” or “brassy” cough, breathing difficulties, wheezing, biphasic stridor, cyanosis, and repeated respiratory tract infections.
Although tracheobronchomalacia has traditionally been diagnosed using laryngoscopy and bronchoscopy, noninvasive airway imaging has become increasingly popular.3 Inspiratory-expiratory airway fluoroscopy has been used with increasing frequency. However, recent studies have shown it to have low sensitivity and specificity, making it a less useful tool.4 Dynamic MRI and CT have also been used to diagnose tracheobronchomalacia. One study found that dynamic CT is highly accurate, performing similarly to laryngoscopy and bronchoscopy in diagnosis and visualization of tracheobronchomalacia.5 The non-invasive nature of the CT makes it a valuable diagnostic tool and first diagnostic choice in many instances. At maximal inspiration, the trachea should appear round or oval and the lungs expanded. Normally, at maximal expiration, the aeration of the lungs decreases. However, the appearance of the trachea is unchanged. In patients with tracheobronchomalacia, the trachea collapses with flattening or forward bowing of the posterior tracheal wall, causing 50% or more expiratory reduction in the cross-sectional area of the trachea or bronchi, which is diagnostic.6 When tracheobronchomalacia is comorbid with cartilaginous disorders, concentric narrowing may also be seen.
Tracheobronchomalacia is managed medically or, in severe cases, with surgery. Currently, there is no standard therapy. Medical management can include medications to decrease mucous secretions, low-dose inhaled corticosteroids to decrease inflammation, and control of gastroesophageal reflux. Surgical intervention is available for children with severe disease who do not improve with medical management. Common surgical interventions include silicone or mesh stent placement, tracheostomy, anterior/posterior tracheopexy, or tracheobronchial resection and reconstruction.7,8
Conclusion
Pediatric tracheobronchomalacia is typically classified as primary disease. Patients most commonly present with a “barking” or “brassy” cough, wheezing, and stridor. Other signs and symptoms include cyanosis, breathing difficulties, and frequent respiratory tract infections. Dynamic CT or MRI is the preferred imaging modality. On imaging, the airway is shown to collapse during expiration. Patients are supported medically in most instances. However, those with severe symptoms may be treated surgically.
References
- Yang D, Cascella M. Tracheomalacia. . 2021.
- Choi S, Lawlor C, Rahbar R. Diagnosis, classification, and management of pediatric tracheobronchomalacia: a review. JAMA Otolaryngol Head Neck Surg. 2019;3:265-275. doi:10.1001/jamaoto.2018.3276.
- McLaren C, Roebuck D. Imaging tracheobronchomalacia in the 21st century. J Med Imaging Radiat Oncol. 2012;56(2):129-131. doi:10.1111/j.1754-9485.2012.02357.x.
- Emmett S, Megow A, Woods C, Wood J. Poor correlation between airway fluoroscopy and rigid bronchoscopic evaluation in paediatric tracheomalacia. Int J Pediatr Otorhinolaryngol. 2022;158:111157. doi:10.1016/j.ijporl.2022.111157.
- Ngerncham M, Lee E, Zurakowski D, Tracy D, Jennings R. Tracheobronchomalacia in pediatric patients with esophageal atresia: comparison of diagnostic laryngoscopy/bronchoscopy and dynamic airway multidetector computed tomography. J Pediatr Surg. 2015;50(3):402-407. doi:10.1016/j.jpedsurg.2014.08.021.
- Lee E, Boiselle P. Tracheobronchomalacia in infants and children: multidetector CT evaluation. Radiology. 2009;252(1):7-22. doi:10.1148/radiol.2513081280.
- Kamran A, Zendejas B, Jennings R. Current concepts in tracheobronchomalacia: diagnosis and treatment. Semin Pediatr Surg. 2021;30(3):151062. doi:10.1016/sempedsurg.2021.151062.
- Shieh H, Smithers C, Hamilton T. Posterior tracheopexy for severe tracheomalacia. J Pediatr Surg. 2017;52(6):951-955. doi:10.1016/j.pedsurg.2017.03.018.
Disclosures
The authors have no conflicts of interest to disclose. None of the authors received outside funding for the production of this original manuscript and no part of this article has been previously published elsewhere.
Citation
. Tracheobronchomalacia. Journal of Pediatric Case Reports. 2026;1(1). doi:10.37549/JPCR-26-0076.